
Abstract
OBJECTIVES
Anti-obesity bias is pervasive among medical professionals, students, and trainees. Stigmatization of patients leads to suboptimal care and clinical outcomes. Educational strategies in medical training are needed to reverse these attitudes. The aim of this study was to evaluate the effect of an innovative didactic intervention and a standardized patient (SP) exercise on attitudes towards patients with obesity among medical students.
METHODS
In 2016, a quasi-experimental study design was used at a US medical school. The class was divided into 2 groups according to a pre-determined protocol based on their clinical schedule, one assessed after exposure to a SP group and the other after exposure to the SP and an interactive lecture (IL + SP group) with real patients. The Attitudes about Treating Patients with Obesity and The Perceived Causes of Obesity questionnaires measured changes in several domains. A generalized estimating equations model was used to estimate the effect of the interventions both within and between groups.
RESULTS
Both groups showed improvements in negative and positive attitudes, although the reduction in scores for the negative attitude domain did not reach statistical significance in the IL + SP group (for the SP group, P = .01 and < .001, respectively; for the IL + SP group, P = .15 and .01, respectively). For perceived causes of obesity, there were no statistically significant changes for pre–post survey measures within each group, except for the physiologic causes domain in the SP group (P = .03). The addition of an IL to a SP curriculum did not result in any changes for any domain in between-group analyses.
CONCLUSIONS
Although adding a novel intervention utilizing real patients to a SP curriculum failed to show an additional educational benefit, our study showed that it is possible to influence attitudes of medical students regarding patients with obesity.
Introduction
Over 40% of the American adult population has obesity. 1 Globally, it is estimated that 600 million adults are obese. 2 From a public health perspective, many believe that reversal of these trends will occur only with social and political regulation of the food industry and physical environment. 3 Until that occurs however, obesity rates will continue to climb, and society will bear the burden of its heavy economic impact. The health profession will continue devoting considerable resources to the management of its comorbidities, and individuals will suffer relentless emotional and physical ramifications. Not only has obesity been characterized as a disease by the World Health Organization, the Canadian Medical Association, 4 and the American Medical Association, 5 but it is also considered a chronic, relapsing, metabolic condition. 6 This concept is not without controversy however, and although they continue to evolve, insurance policies for evidence-based obesity treatments remain inconsistent in the United States. 5 Future medical professionals therefore have a moral and ethical responsibility to possess at least basic competency in the management of patients who suffer the consequences of excess adiposity.
Unfortunately, contemporary evidence suggests that clinicians lack awareness regarding the complexity of obesity and have little, if any, formal education or training in its treatment. 7 A survey of Canadian final-year medical students revealed a low level of knowledge and competence for managing patients with obesity. 8 Excess weight has been shown to be a commonly and strongly stigmatized characteristic. 9 Primary care physicians, medical residents and students, nurses, and other providers hold negative opinions, both explicit and implicit, towards patients with obesity.10,11 Bias against individuals with excess weight has been shown to be as pervasive among healthcare professionals as it is among the general public. 11
Recently, international experts and scientific societies have formally called for efforts to end stigma and weight bias in academic institutions and professional organizations. 9 Notably, weight bias in the healthcare system is associated with inferior health outcomes, 12 avoidance of care, 13 and less cancer screening. 14 Breaking this cycle of stereotyping would therefore seem like a logical strategy in medical school and other professional curricula. A handful of studies have investigated interventions to combat discrimination in medical settings. Reports have consistently found that teaching students about the multifactorial etiology of obesity, particularly the contribution of genetic and environmental factors, was crucial to reducing measured weight bias.15,16 Various methods and strategies have been studied. Some specific evidence-based principles have been recommended for undergraduate medical education, such as brevity (<3 h) of interventions, the use of video-clips, supporting techniques to promote behavioral change, in-person contact, and teaching the pathophysiology of obesity. 17 To date however, there is no standardized curriculum for educating the nation's medical students around the care and management of patients with obesity. It remains unclear which types of educational approaches or methodologies are most effective and specifically which characteristics of the exposure contribute to reducing medical students’ negative feelings towards patients with excess weight.
The objective of this study was to assess the effect of an innovative interactive lecture (IL) and a standardized patient (SP) exercise on attitudes of third-year medical students towards patients with obesity.
Methods
The current study is a prospective education intervention using a quasi-experimental design with 2 questionnaires to assess pre- and post-measures. Our hypothesis was that the addition of an IL to an established SP exercise would result in further benefit for changing attitudes towards patients with obesity.
Sample
In March 2016, at the University of California San Diego (UCSD), 122 medical students participating in a required primary care education module on the topic of obesity were eligible to participate. The study was approved by the Institutional Review Board (IRB) at UCSD. In accordance with IRB endorsement, students were advised prior to the sessions that participation was voluntary, that completion of the surveys represented consent to participate and that anonymity was maintained. Declining to participate was the only exclusion criterion. Surveys were delivered and collected by members of the research team. Questionnaires were de-identified and labeled with pre-determined codes.
Intervention
Third-year medical students at UCSD participate in a primary care core clerkship which includes monthly 4-h sessions (including time for orientations and breaks) on different topics commonly encountered in the primary care setting. One of those sessions is dedicated to obesity. Although the didactic structure can vary between modules, all sessions include small group meetings with 6 to 8 students and 2 primary care faculty members. Some of the topics utilize SPs, portrayed by professional actors, and trained by education faculty members, in the specific condition encountered. The obesity module is composed of a large class lecture and an SP session in small group format facilitated by the faculty. The 1-h lecture was created and delivered by a faculty member certified by the American Board of Obesity Medicine (ABOM) and included content addressing the biology and pathophysiology of obesity and evidence-based therapy recommendations, including lifestyle and behavior modification, pharmacotherapy, and bariatric surgery. Importantly, an innovative strategy during the presentation was the presence of 4 real patients treated with the interventions discussed in the lecture: one with behavior therapy and pharmacotherapy, one with behavior therapy and a low-calorie diet using meal replacements, and 2 with bariatric surgery. Students were also required to read on these topics before the session. The intent of the IL was not only to provide the patients’ experiences relating to their respective therapies but also to foster an interactive environment whereby students could gain a better appreciation for the struggles, discrimination, and stigma individuals with obesity face in the healthcare system. The patients were unrehearsed. By combining the patients’ experiences with biological underpinnings of obesity, the aim was to change anti-obesity attitudes. The patients were prompted to explicitly address this towards the end of the lecture. Because the use of SPs had been the standard education activity for several years, the introduction of the IL was considered the novel intervention to evaluate. The effectiveness of the SP experience was not empirically examined prior to this study.
The SP encounter was created by an ABOM-certified faculty member and education professionals associated with medical teaching. The duration of the SP activity was 1-h and 45 min. The actors, all of whom had obesity, were trained to present with weight-related comorbidities commonly encountered in the primary care setting. Students volunteered to interview the SP across 3 different simulated visits, each lasting 10 to 15 min. As standard practice throughout the course, they take turns playing the role of the primary care physician, interspersed with feedback and discussion from the faculty facilitators and other students. Although time allowed for only 3 or 4 volunteers, all students participate in role playing at least once throughout the year across the various disease modules. They were instructed to use motivational interviewing (MI) techniques to elicit behavior changes that promote weight reduction. All students had exposure to MI skills in previous curricular activities. The SP initially exhibits resistance to recommendations for weight loss interventions but is trained to respond to effective MI techniques. The actors were also trained to provide feedback to the students on communication skills, MI competence, and effectiveness in fostering confidence for behavior change. By design, the interaction reflects real-world experience and can be frustrating to some students.
The class is normally divided into 2 groups, receiving the same education content on different days. Students are assigned to a specific day based on their clinical preceptorship schedules. Three days separate the sessions. The predetermined class assignment allowed for a quasi-experimental study design, as it was not practical to randomly assign students to specific class cohorts. The sequence of didactic activities was not thought to detract from their educational value. The first cohort received the SP exercise followed by the interactive patient lecture, with the pre–post assessment tools administered before and after the SP intervention only (SP group), considered the control group. The second cohort was provided the IL before the SP experience, with the assessment tools administered before the lecture and after the SP interaction. This group was considered the intervention group (IL + SP group). In the IL + SP group, the lecture was delivered before the SP activity for logistical convenience of distributing and collecting the questionnaires. For educational requirements, both groups received the same duration and content for each activity. It should therefore be noted that the IL + SP group had a longer total time of exposure between the pre–post surveys. Figure 1 shows the study design flowchart.

Study design flowchart: A flow diagram of the educational sequence in both groups and time points of the pre- and post-surveys. A readiness assessment test (not a component of this study) and the pre-survey were administered during the hour prior to the start of the educational activity. There was a 15 min break between the 2 activities. The total duration of the session was 4 h.
Surveys and outcome measures
To evaluate attitudes and biases towards obesity, students were administered 2 surveys: Attitudes about Treating Patients with Obesity (ATPO)10,18 and Perceived Causes of Obesity (PCO)11,19 before the beginning of the session (pretest), followed by a second set of the same surveys (posttest) at the corresponding time points. Both instruments were previously developed and validated to assess weight bias among healthcare trainees.10,19
The 23-item ATPO and the 14-item PCO questionnaires, each using a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree and 1 = not at all important, 5 = extremely important, respectively), were used to assess changes. Four items in the ATPO survey were discarded as they were not relevant to the responses being analyzed. The remaining 19 items in the ATPO are converted into 2 domains: negative attitudes (AT.N) about obesity and positive attitudes (AT.P) about obesity (Table 1). The items in the PCO questionnaires are converted into 3 domains: physiological causes (PC.P), behavioral causes (PC.B), and environmental causes (PC.E) (Table 2).11,19 A higher score indicates a greater attribution of the domain for causing obesity. (The actual questionnaires administered are available in the Supplemental material S1). These sub-scales have been used previously with acceptable scale reliability, 18 with slight modification for our study to better fit respective categories. We used comparison of responses to the ATPO to assess our primary outcome of interest, a change in attitudes among healthcare professionals treating individuals with obesity. The subjects of our study had experienced at least 9 months on inpatient wards and outpatient clinics interacting with patients. Assessing perceptions about the causes of obesity using the PCO measure was our secondary outcome.

The items are divided into 2 domains: negative attitudes (AT.N) and positive attitudes (AT.P). Students responded using a 5-point Likert scale ranging from (5) strongly agree to (1) strongly disagree. Items 20-23 were excluded as they were not relevant to the outcomes being analyzed. The survey has been modified from the originally published version to reflect less stigmatizing language.
Negative attitudes.
Positive attitudes.

The items are divided into 3 domains: behavioral causes (PC.B), physiologic causes (PC.P), and environmental causes (PC.E). Students responded using a 5-point Likert scale ranging from (5) extremely important to (1) not at all important.
Behavioral factor.
Physiologic factor.
Environmental factor.
Demographic information (age, sex, race/ethnicity, and body mass index [BMI]) was collected to determine the degree, if any, of covariance.
Statistical analysis
Each domain of both surveys was analyzed using descriptive statistics including the mean and standard deviation (SD). Counts and percentages were used for categorical data. A generalized estimating equations (GEE) model was used to assess the effect of the didactic sessions on attitudes using a time-based model (pre-time and post-time). 20 For those domains with a significant time by cohort interaction detected, we further examined differences between the 2 groups of medical students to test the effect of the IL intervention. To investigate whether any differences identified were the result of demographic variables, we included age, sex, race, and BMI as covariates in the model to assess whether the significance changed for time by cohort interaction. For each domain of items, α was set at 0.05. Effect sizes were estimated by calculating partial eta squared (η2). Details are provided in Supplemental material S2. For missing data, the GEE analysis allows for the use of respondent data with at least one observation at pre- or post-intervention.
To assess both the effect of the obesity module on survey measures in both groups and to assess the effect of the IL intervention on the treatment group, we used the following GEE model: Hypothesis 1:
We test the treatment effect for each group by:
H0: β1 = 0 (no treatment effect for the SP group)
H0: β1 + β3 = 0 (no treatment effect for the IL + SP group)
Hypothesis 2:
We test whether the interactive lecture has an effect on the pre-post changes by
H0: β3 = 0
The data were analyzed using “geepack” version 1.3-1 with R version 3.6.3 (R Core Team). 21
Results
Sample characteristics
Considering the overall class size, 122 students were eligible; 73 in the SP group and 49 in the IL + SP group. Four chose not to participate, 1 student and 3 students in each group, respectively. The numerical imbalance between the 2 groups reflects the distribution of availability based on their clinical preceptorship assignments. Overall, the demographic characteristics between the 2 groups were well balanced, with a mean age of 26.8 years, 44.1% female (n = 52), and normal BMI (Table 3). More than 40% (n = 52) of the students were Asian, approximately one-third (n = 35) were Caucasian, and the remainder were a composite of African American, Hispanic/Latino, or not specified. Subjects with missing data are tabulated in Table 4.
Characteristics of third-year medical students participating in a primary care clerkship obesity education session.
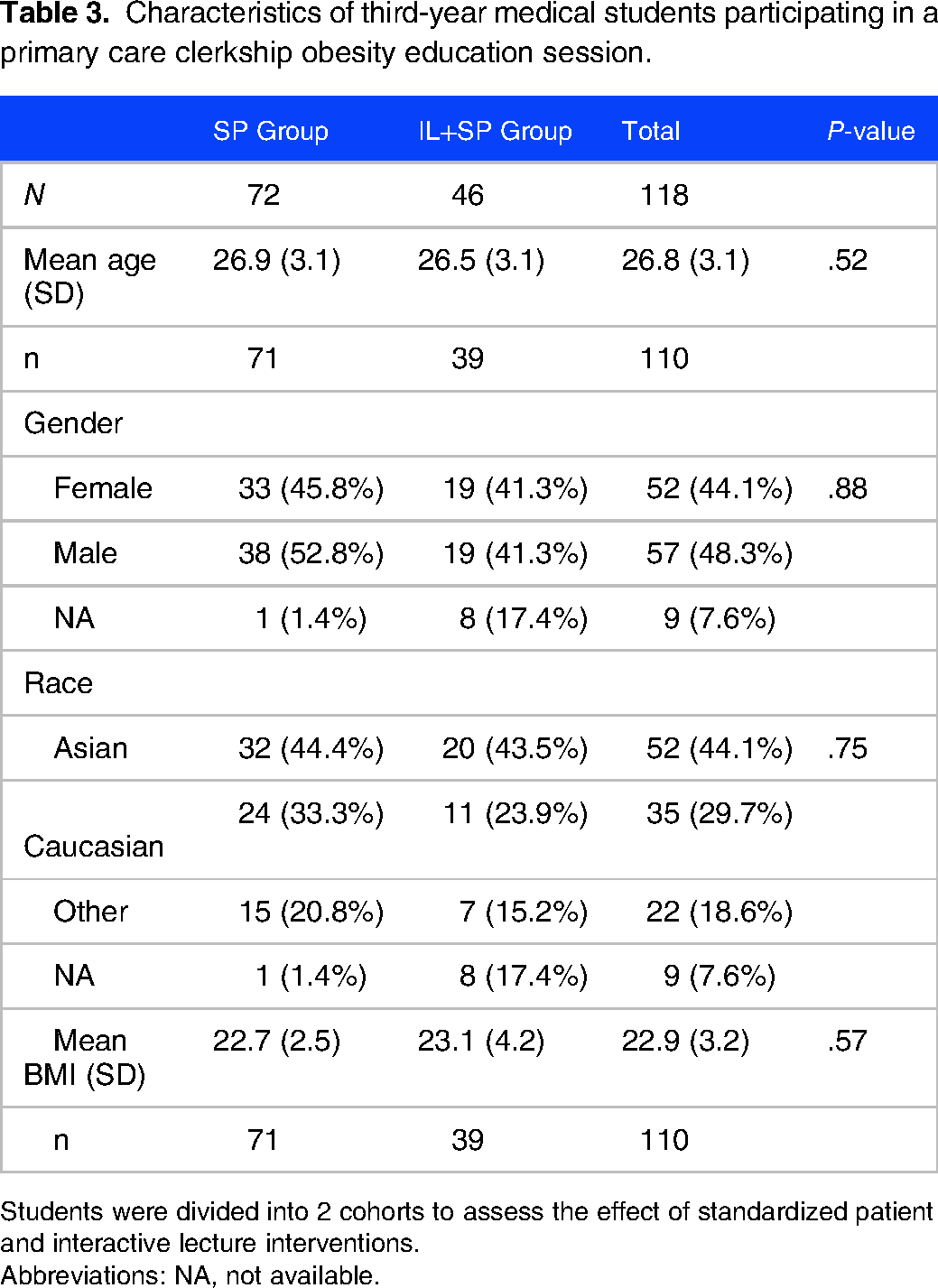
Students were divided into 2 cohorts to assess the effect of standardized patient and interactive lecture interventions.
Abbreviations: NA, not available.
Changes in mean scores of survey measures among 2 cohorts of third year medical students.

Students participating in a primary care clerkship obesity education session at a US medical school divided to assess the effect of standardized patient and interactive lecture interventions. The SP group underwent pre- and post-assessments before and after the SP exercise only. The IL + SP group underwent pre- and post-assessments before and after the IL intervention and SP exercise.
Abbreviations: AT.N and AT.P, negative and positive attitude domains, respectively, for the ATPO questionnaire; IL, interactive lecture; NA, not available; PC.B, PC.E, and PC.P, behavioral, environmental, and physiologic causes of obesity domains, respectively, for the PCO questionnaire; SP, standardized patient.
Scores are reported as mean values (SD).
Attitudes about treating patients with obesity
Table 4 shows the results of the primary outcome measure scores. The obesity module resulted in a reduction of AT.N scores for both cohorts. Using our GEE model, the SP exercise was associated with a statistically significant effect of lowering negative attitudes (P = .01, partial η2 = 0.009). However, the change in the IL + SP group did not result in statistical significance (P = .15). Both the SP and IL + SP interventions resulted in a statistically significant improvement in positive attitudes (P < .001, partial η2 = 0.084 and P = .01, partial η2 = 0.037, respectively). Figure 2A shows the effect of the interventions on the direction of change for negative and positive attitudes. Using our model, addition of the IL intervention did not result in any significant difference for changes in negative or positive attitudes between the 2 groups (P = .84 and P = .47, respectively), shown in Table S3 in the Supplemental material.

Changes in measures of anti-obesity attitudes and perceived causes of obesity among third-year medical students. Pre- and post-test results for the medical student class presented as composite scores, IL+ SP group, and SP group. Panel 2A shows the results of the ATPO items and panel 2B shows the results for the PCO items. Asterisks mark changes in scores with P < .05. The results are reported as the mean scores with corresponding 95% confidence intervals.
Perceived causes of obesity
There was a reduction in the mean score for the physiologic causes domain in the SP group and an increase in the IL + SP group (Table 4), but only the former reached statistical significance (P = .03, partial η2 = 0.005 and P = .67, respectively). Both groups demonstrated an increase in mean scores for the behavioral causes domain for the PCO questionnaire, but neither reached statistical significance. There was no significant change in the environmental causes domain for either group. When comparing the 2 groups for effect of adding the IL to SP intervention, there was no significant change for any of the domains (PC.B, P = .87; PC.E, P = .41; PC.P, P = .13; Table S3). Figure 2B shows the effect of the interventions on the direction of change for the PCO domains.
Demographic covariates (age, sex, ethnicity, BMI) had no significant effect on changes within any of the domains for either questionnaire (data not shown).
Discussion
Our study sought to evaluate the effect of an IL format, added to a SP exercise, on changes in anti-obesity attitudes among third-year medical students. Although our investigation revealed that the use of SPs improved attitudes (an educational activity not previously tested in our course), our GEE model did not support our stated hypothesis. Both groups demonstrated statistically significant increases in positive attitudes and the SP group, but not the IL + SP group, a decrease in negative attitudes. Effect sizes were small for all estimates. For our secondary outcome measures regarding perceived causes of obesity, only the SP group demonstrated a statistically significant change (with a small effect size) in the domain of physiologic causes, but not in the other domains.
To our knowledge, this is the first report describing an educational activity combining traditional content delivery with real patient experiences in an interactive format. The intervention of the IL did not, however, result in a significant difference in change for any of the domains in the between-group analyses. There are several possible explanations. First, it is possible that the SP component of the module was sufficient for this purpose using the measures in the present study. Second, it is also possible that the faculty facilitators in the SP small group sessions exerted a powerful influence on the items measured as they were trained by the obesity module leaders. Third, the students may have been “primed” by previous education. During the first 2 years of medical school, they were exposed to lectures on metabolism, human weight regulation, and genetics of obesity. Additionally, one of the required readings for the educational session in the present study informed students on the same concepts. 22 Fourth, this sample of learners had a mean BMI in the normal category, which may have impacted the outcome measures. Finally, the unpredictable nature of unrehearsed real patients in medical education has been identified as a limitation. 23 Our patients were unrehearsed, and it is possible that the self-perceptions of their own experiences were discordant with the intended goal of the lecture, namely the importance of uncontrollable contributors to obesity (neuro-enteroendocrine regulation of weight) and evidence-based therapies, potentially causing confusion and ambivalence among students.
Others have shown that educational interventions can promote favorable attitudes towards patients with overweight and obesity.16,24,25 There are few reports in the literature specifically assessing the effectiveness of SPs for changing anti-obesity attitudes, and the results are mixed. One study evaluated the correlation between the acceptance of negative attributes of individuals with obesity among learners and patient-centered behaviors using a simulated clinical scenario, but it was not an intervention study. 26 Using SPs after an IL on counseling and behavior change in another study, students’ attitudes on the utility of counseling did not improve, but in this project the focus was on nutrition counseling, without specific attention to weight reduction. 27 One study similar to our use of SPs demonstrated a reduction of anti-obesity stereotyping and increased empathy, but there was no control group. 24
One issue of concern with all analyses using questionnaires is whether the correct tool is utilized to answer the main study question. The ATPO measure has been shown to have adequate scale reliability among cohorts similar to the ones used in the present study.10,12 Likewise, the PCO measure has been utilized previously with good reliability.11,19 In our analysis, however, there was no effect of the educational activity on the learners’ perceptions, with the exception of one domain in one cohort. The psychometric properties of this questionnaire in previous studies were based on populations that were very different than ours. The subscale categorization in our analysis was slightly modified, which needs to be recognized as a possible limitation. Moreover, the items in this tool were somewhat vague and may have reduced the validity with respect to the content delivered in the lecture. Knowledge regarding biological and genetic underpinnings of human weight regulation has advanced since development of this instrument and perhaps a more updated questionnaire would improve its psychometric properties.
Although both groups demonstrated desirable changes in attitudes towards patients with obesity, effect sizes were small. It is not clear whether a different educational strategy or content would have resulted in a stronger quantitative change. It is also possible that these students had favorable baseline attitudes towards treating patients with obesity, with differential changes unlikely to be altered by only one brief intervention. In fact, previous work has also suggested that among medical professionals in training, there may be less weight bias in comparison to their instructors and more experienced peers in practice. 10 Others have documented a high degree of stigmatizing attitudes among primary care physicians. 11 It is unclear whether there is a true discordance between learners and their contemporary practicing counterparts and if so, whether this is a generational difference or a result of the refractory nature of weight management in real clinical settings.
The discordance in the significance of change for the negative attitudes domain in the ATPO may be from lack of statistical power given the relatively small sample size, but we cannot rule out a negative impact of the IL on the SP activity due to temporal proximity of the 2 interventions, or vice versa. Although the IL did not demonstrate a significant change in the between-group analysis, our data suggest that, in contrast to the SP exercise alone, it may have exerted an undesirable effect on negative attitudes. We did not assess a group of students before and after the lecture without an SP activity, making it difficult to reach any conclusions regarding the effect of the lecture alone. Evaluating more longitudinal educational interventions throughout the course of the medical school curriculum and temporally separating divergent strategies may help isolate their effects on learners. Future studies should assess the value of using SPs compared to interventions that may require less cost and resources.
Although the best educational intervention for reducing anti-obesity stigma and bias among students and trainees in healthcare professions remains to be identified, adequate attention for curriculum development remains very challenging. 28 Because obesity medicine is rarely covered on licensing and certification examinations, education and training programs have little incentive to prioritize obesity topics in already crowded curricula.29,30 Obesity education and training have been shown to improve confidence and competence for treating patients with excess weight. 31 Recently, competencies have been developed for training programs, hopefully standardizing the development of obesity medicine education in medical schools. 32
Our study has limitations that should be recognized. First, our sample size was relatively small and limited to 1 year at 1 institution. A post-hoc power analysis was not performed due to its inherent limitations on analytical validity and reliability. 33 Future studies should aim to span a longer time period and multiple medical schools to enhance validity, reliability, and generalizability. Second, the obesity module was of short duration and the longitudinal assessment measured only immediate effects. It is unclear whether the changes seen in attitudes are durable or whether they extinguish with time. Third, it is possible that the use of other measures would yield different results. Disparate findings have been documented in other studies. 16 Fourth, a quasi-experimental study design is not without significant limitations. Although this approach may have better internal and external validity than retrospective observational studies, we cannot rule out other unrecognized confounders contributing to our findings. For example, we did not confirm the presence or absence of contamination between the 2 groups. Lastly, it should be noted that many items in the ATPO survey addressed attitudes of practitioners treating people with obesity. Although students in the present study possessed at least 9 months of clinical clerkships interacting with patients, their relative lack of clinical experience may have impacted the external validity of this particular instrument.
Conclusions
Anti-obesity bias and stigma are major obstacles to the provision of high quality and effective clinical care. Medical schools should therefore develop education interventions to reduce negative attitudes towards patients with obesity. Our study adds to other work showing the positive impact of using SPs to this end. We can conclude that our educational exercise, using a trained SP, with or without the provision of content and context using a patient IL, resulted in the desired outcome of changing anti-obesity attitudes among medical students. Although a novel approach of combining a traditional lecture with an interactive patient panel did not add value using the measures chosen for this analysis, much more research is needed to find educational interventions that effectively and efficiently reduce weight bias among our future physicians.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231207683 - Supplemental material for Exploring the Effect of Adding an Interactive Lecture to a Standardized Patient Curriculum on the Attitudes of Third-Year Medical Students About Patients With Obesity: A Quasi-Experimental Study
Supplemental material, sj-docx-1-mde-10.1177_23821205231207683 for Exploring the Effect of Adding an Interactive Lecture to a Standardized Patient Curriculum on the Attitudes of Third-Year Medical Students About Patients With Obesity: A Quasi-Experimental Study by Eduardo Grunvald, Jennie Wei, Tuo Lin, Kun Yang, Xin M Tu, Ottar Lunde, Evelyn Ross, Jessica Cheng, Jennifer DeConde and Neil Farber in Journal of Medical Education and Curricular Development
Footnotes
Abbreviations
Acknowledgements
The authors would like to thank Robert MacAulay, MMHPE and Peggy Wallace, PhD for their expertise in developing the standardized patient case. They are grateful to the course directors Dave Bazzo, MD and Joe Ramsdell, MD for providing liberty to adjust the didactic sequence to accommodate the study design. The authors thank the faculty facilitators for cooperation and implementation of the research study. Data collection and coordination of course schedules would not have been possible without the administrative assistance of Olivia Anonas and Felipe Zatarain. The authors would also like to thank the standardized patient actors for their talent. They are deeply indebted to the real patients for sharing their personal experiences.
Author Contributions
Conception and design: EG, JW, OL, NF. Provision and collection of surveys to students: JW, ER, JC. Compilation and creation of database: JW, ER, JC. Data analysis and interpretation: TL, KY, XMT, EG. Manuscript writing: EG, JW, JD. Supervision of entire project: EG. Intellectual contribution and final approval of manuscript: all authors.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EG has received consulting fees from Novo Nordisk, Currax Pharmaceuticals, and Gelesis, Inc. He has also received research support from the Obesity Treatment Foundation (Grant No OTF001), The Litwin IBD Pioneers Program Crohn’s and Colitis Foundation, Aardvark Therapeutics, and Eli Lilly. All other authors had no competing financial or nonfinancial interests for this work.
FUNDING
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was partially supported by the National Institutes of Health, Grant UL1TR001442. The content is solely the responsibility of the author(s) and does not necessarily represent the official views of the NIH.
Ethical approval and informed consent
The present study was approved by the UCSD IRB as exempt from full review (Project No 160416). All research activities were conducted in accordance with institutional ethical standards and regulations. In accordance with IRB approval and endorsement, students were verbally advised before the sessions that participation was voluntary, completion of the research surveys represented informed consent, and anonymity was maintained.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.