
Abstract
OBJECTIVE
Food insecurity is a social determinant of health (SDOH) affecting 1 in 10 households per year in the United States and has major impacts on the course of chronic health conditions. It is beneficial to introduce screening and appropriate treatment plans to medical students. This study utilized a novel case-based learning exercise (CBLE) to assess confidence, attitudes and improvements in knowledge on recognizing and addressing food insecurity.
METHODS
A CBLE focused on food insecurity was developed to be implemented in a 2-h session as part of the curriculum for all first-year medical students at the Medical University of South Carolina. The CBLE included a case for discussion, followed by an interview with a standardized patient. Students received invitations to complete pre- and post-CBLE assessment surveys.
RESULTS
Completion of both pre- and post-surveys was achieved by 29% of students (48 out of 166). Knowledge around the formal definition of “food insecurity,” how to recognize food insecurity versus hunger, and how to screen for food insecurity all increased significantly (P < .05). Responses relating to the association between certain chronic diseases and food insecurity did not change pre and post-CBLE.
CONCLUSION
This novel CBLE was successfully implemented within a 2-h teaching session and improved knowledge on recognizing food insecurity in practice. However, additional learning exercises are likely needed to improve knowledge of the relationship between food insecurity and chronic disease states. Nonetheless, the CBLE structure provided students with multiple formats of learning and integration of skills, which shows promise and may be applicable to improve knowledge of other SDOHs.
Introduction
Food insecurity (FI) affects approximately 1 in 10 households at some point during a single year in the United States. Achieving optimal control of chronic diseases—including Type 2 diabetes, hypertension, and depression—is adversely affected by food insecurity regardless of age and ethnic or racial groups.1–3 Inclusion of didactic material regarding various social determinants of health (SDOH) in undergraduate medical curricula is widely accepted as important and cogent to their professional education. 4 While students are often given some degree of instruction on food insecurity during didactic sessions in preclinical classes covering SDOH, the mode of delivery is widely variable, and assessment of their learning is often limited to attitudinal change. 5 Students are infrequently given the opportunity to problem solve or provide instruction on screening for FI during patient interactions. Further, most institutions have minimal, if any, instruction for students on how to address FI when identified in screening. Medical professionals express reluctance to screen for food insecurity in part due to their lack of competence in appropriate screening, concerns about embarrassing parents of pediatric patients, 6 as well as lack of knowledge on how to proceed after positive screening has occurred. However, studies have shown that parents of pediatric patients respond favorably to their clinician screening for food insecurity 7 despite their own embarrassment that is sometimes reported. A recent study in 2020 reflected that the physician–patient relationship was not hindered by screening for food insecurity in primary care settings and that patients largely viewed this screening positively. 8
In this study, we review the successful implementation of a novel curricular element focused on food insecurity. The current small group learning session is a mandatory session for all first-year preclinical medical students at the Medical University of South Carolina (MUSC). In choosing this setting the didactic and practical application of the information can be learned and cemented during practicum in a standardized patient encounter, which has been shown to add value in teaching students how to navigate difficult patient encounters. 9 This model can be implemented at other institutions in order to strengthen the SDOH curriculum.
Current contributions in MedEd Portal broadly address SDOH, 10 some examine specific areas11,12 but none focus on food insecurity screening and recommendations for providers in regard to management. Literature supports and encourages healthcare settings, especially those with underserved patient populations, to implement food insecurity screening and referral programs as well as participation in an experiential integrative service for medical students which have improved students’ understanding of food insecurity.13,14 Educational interventions regarding food insecurity are shown to improve knowledge and attitudes toward screening for food insecurity and lead to measurable patient and system-level changes. 15 Given the importance of this singular social determinant in patient health and welfare, a feasible curricular activity devoted to teaching students how best to identify and address it is beneficial as not all teaching facilities will be able to institute the experiential integrative models of service for this purpose. The present study responds to this need.
Methods
All first-year medical students at MUSC are enrolled in and required to complete clinical skills an 18-month longitudinal course with several components including clinical skills small group sessions. In the first academic year, each clinical skills small group meets approximately once a week each semester, for a 2-h period, on a specific day of the week. The clinical skills small groups have approximately nine students in each group with two faculty preceptors. Faculty preceptors guide students through planned sessions that include various learning components such as a review of material covered in modules viewed prior to class, student presentations, interviewing and communication skills, physical exam skills, standardized patient encounters, and student-led case-based learning exercises (CBLE). For each session, a subset of students is preassigned, from a random selection, to complete certain activities.
As part of the Fundamentals of Patient Care Theme, all students receive lectures related to healthcare disparities and SDOH. During the gastrointestinal block of the pre-clerkship curriculum, students received lectures related to addressing food insecurity. These sessions took place prior to the CBLE on screening for food insecurity.
We prearranged and scheduled this small group session focused on food insecurity to take place after students received their SDOH lecture on food insecurity. For this specific session, we provided students with the student version of the CBLE (see Appendix A) to review prior to class and gave them instructions on how to prepare for the student-led discussion (flipped classroom format). The CBLE contained a description of a patient scenario/case, questions to consider for discussion, and links to resources for review of relevant material.
During the scheduled session, small groups met to complete the CBLE, with students leading the discussion. We assigned the preselected subset of students to also complete a standardized patient encounter as part of the session that day. During the standardized patient encounters, student interviewers obtained a full history and offered counselling if appropriate, while the remainder of the small group and preceptors participated through observation and offering feedback. Group discussion of pertinent points raised by students or standardized patients occurred at the end of the session.
As part of the assessment for the session, we emailed all students a link to a survey hosted by REDcap. The survey was developed by the PI, with assistance from the Services, Pricing, and Application for Research Centers of the SC Clinical Translational Research Institute at the Medical University of South Carolina. The survey used in this study is not validated or previously pilot-tested therefore this study presents the initial pilot data available for the use of this instrument. The survey was reviewed and the process for distribution to the medical students was approved by the College of Medicine Education Dean's Council as is mandatory at this institution. It was reviewed and approved as exempt by the IRB who considered completion of the survey as informed consent. Viewing this as a pilot study, we considered our sample size of 166 students, representing 100% of the freshman College of Medicine class, as the maximum number of subjects we could approach for this pilot study thus a power calculation was not performed. The entire study was undertaken during the first two weeks of February 2020 when all students would have received the curricular material and had their mandatory small group activity occur. A review of results occurred after this period of time. The nature of the study involved ascertaining whether or not the completion of this curricular element led to changes in attitudes among students regarding screening for food insecurity in patients as well as changes in their knowledge regarding this topic. The survey contained nine (9) (Appendix B) questions on the demographics and background, and 21 questions (Appendix C) on the assessment for the session, including measures of attitudes as well as knowledge base, and prior experience with food insecurity. We communicated to all students in a written invitation to complete the survey that completion was voluntary and not linked to their grades received for this curricular element. We then sent the initial preassessment survey was to all first-year students during the week prior to their scheduled small group meetings. Subjective feedback from both students and preceptors would have been given and discussed as a small group during their individual sessions but was not requested or recorded as part of this assessment. The entire class was invited to complete the postsession survey in the 3 days after the end of the week.
Statistical analysis: We analyzed pre- and postsurvey using NcNemar's test for categorical variables and Wilcoxon signed rank test for ordinal variables, in IBM SPSS Statistics 25. P-values were calculated to determine if the results were statistically significant, which was determined at a P-value of 0.05.
Results
A total of (166 students) completed the learning activity as clinical skills small group sessions are mandatory for all students. The first-year medical student class was composed of 55% female and 45% male. Twenty percent were underrepresented in medicine, 93% were in-state students, and 7% were out-of-state students. Facilitators are faculty and residents at the Medical University in fields of medicine, psychology, or licensed social workers.
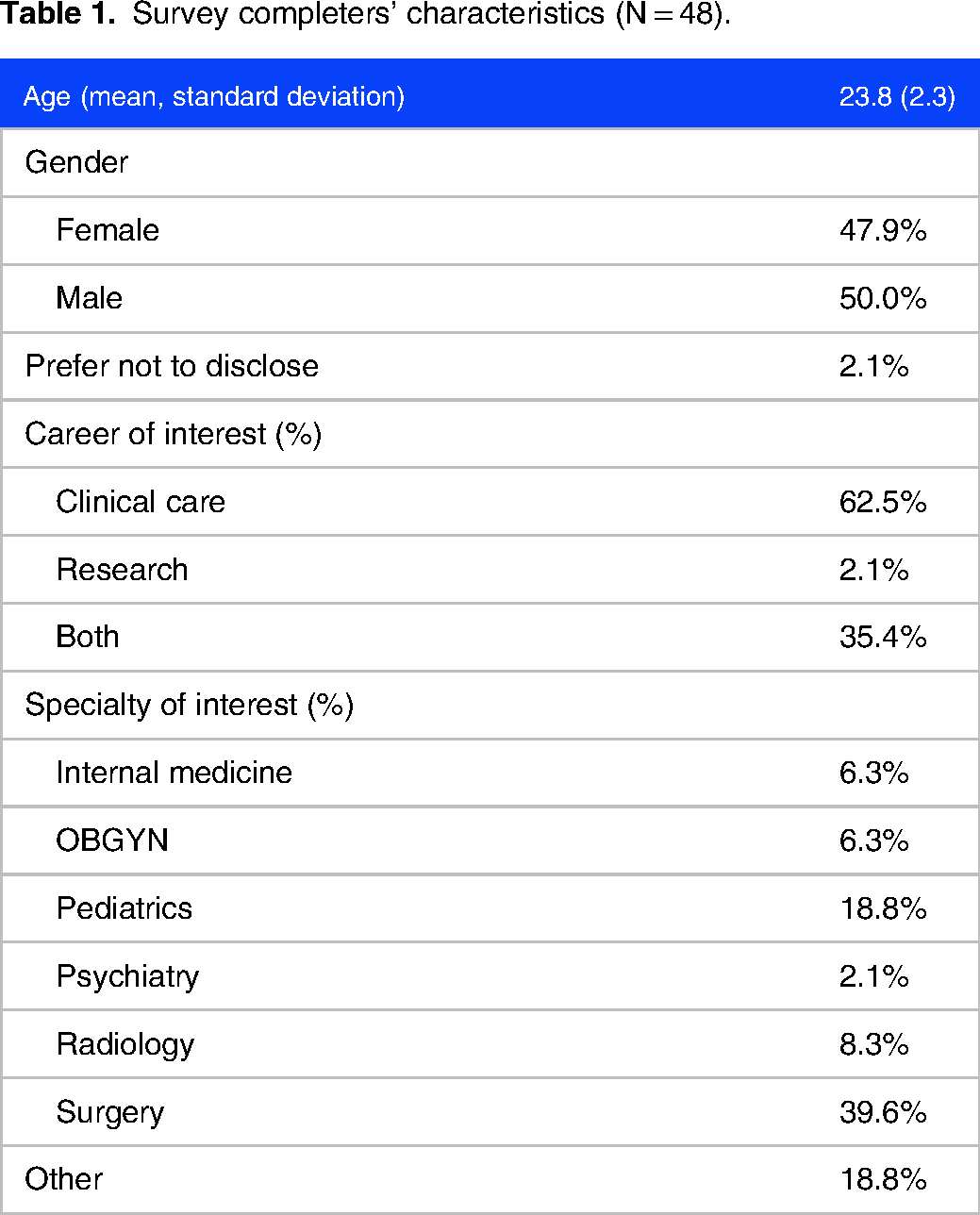
The survey results showed 88 complete responses for pre and 50 for post. The total completed corresponding pre–post surveys that we could include for analysis was 48 (29.9%). In these completed surveys, the students were majority male, 23.81 years old on average (2.27 SD) and they showed a spread across medical specialties when asked about their interest for the future (Table 1). Most students (47 or 97.9%) planned to have a clinical component to their future practice of medicine. Only a small percentage of students (19 or 39.6%) reported knowing the formal definition of the term “food insecurity” prior to the CBLE as compared to 40 or 83.3% after the exercise (p < .001). In the portion of the assessment dedicated to knowledge, a majority of the students correctly identified the scenario as illustrating food insecurity as opposed to hunger, but there was still a significant increase after the CBLE was completed (36 students or 75.0% pre vs 45 or 93.8% post, P < .03). A majority of students correctly identified associations between diabetes and depression with food insecurity, but also incorrectly identified an association between gastrointestinal cancer and stroke with food insecurity. We did not see a significant change in these measures pre- and post-intervention. While practically all students (47 or 97.9%) thought it important to screen patients, few reported knowing how to do so or how to alter a medical plan prior to implementation of the curricular exercise (3 or 6.5% and 5 or 10.4% respectively). We saw a significantly higher number of students (46 or 95.8%) who reported knowing how to implement the validated two-question screener for food insecurity post-intervention (P < .001). Similarly, we saw a significant increase in the number of students (41 or 85.4%) who reported understanding how to incorporate changes in a medical care plan to address food insecurity at the end of the exercise (p < .001) (Table 2). In the section relating to patient interactions specifically, we only observed significant improvement in two questions: “patients will not answer accurately about access to food” (32 or 66.75 vs 41or 85.4% correct answers, p < 0.03) and “patients will appreciate being asked about their access to food” (36 or 75.0% vs 45 or 93.8% correct answers p < 0.02).
Survey completers’ characteristics (N = 48).
Survey completers’ reported confidence in incorporating food insecurity in their clinical care (N = 48).

Results are on a Likert scale from 1, “not confident,” to 5, “very confident.” All pre- and postdifferences were significant P < .001 as assessed with Wilcoxon Rank Sum Test.
Discussion
While food insecurity is often included in curricular components covering social determinants of health, there is rarely an opportunity for student problem-solving as well as direct implementation of the screening and patient interaction through the utilization of standardized patients. Given the data showing that medical professionals are reluctant to screen for FI given both their lack of nutrition knowledge as well as discomfort with referring patients to resources, the implementation of this module was a first step in addressing this early for trainees. 6 The data from this initial assessment showed strong positive results in terms of student understanding of how to screen for food insecurity as well as implementation into a plan of care. Given the prior research showing this as a roadblock to medical practitioners implementing screening, this alone accounts for a notable positive result. 6 There was also a strong shift in self-reported confidence in performing the screening within a medical setting. There were few questions aimed at assessing knowledge. Regarding food insecurity and chronic disease, knowledge was not impacted positively and may require additional learning exercises for exposure and integration of this information by the students. These domains can be further assessed in future studies through qualitative data gathering from participating students. In addition, attitudinal responses regarding patient expectations did not reflect the known patterns of patient responses in the current literature. 5 In the future, more discussion of patient-focused studies should be included to help address this. Importantly, despite their concerns about patient reception of screening, almost 100% of students did regard screening as important, thus we hope to overcome their perceptions of negative patient reception of screening through further education and teaching.
Small group sessions are popular and highly regarded by the first-year medical students at our institution, consistently rated as one of their favorite curricular elements during their preclinical years. It was a natural fit for the inclusion of this focus on food insecurity as we felt students needed not only to learn the material but to discuss it with preceptors in an encouraging and nonthreatening format. This format also uniquely allows for practicing the implementation of a screening tool with a standardized patient. The small group format allowed the three elements we found most necessary for learning: coverage of didactic material, problem-solving in small groups, and implementation through a standardized patient encounter.
The major limitation of this approach is that only a small section of students were able to implement the screening tool for practice with a standardized patient immediately given the constraints of time for small group sessions. While all students were able to complete the didactics and problem-solving aspects, three selected students from each small group were able to practice the final aspect of the exercise, which was interviewing a standardized patient to implement the screening tool and discussion. A recognized limitation in assessing changes in students’ knowledge through this activity is that it would require a longer survey of content-based questions. Given the pilot-based nature of this study, we chose to focus on a few high-yield content-based questions to enhance survey completion and assessment, but this can be expanded in the future for a more extensive assessment of how their knowledge base changes through this exercise. This novel approach shows promising evidence of content validity, demonstrating the items used in the screening tool with SPs adequately covered the relevant dimensions being measured. An assessment was not developed for preceptors/facilitators, and this may be valuable going forward as well to move toward assessing for construct validity. Additionally, further iterations of this intervention can be further analyzed with small focus group sessions of students who have completed the SP interviewing to further assess gains in confidence and knowledge in performing FI screening and review predictive validity with this novel approach.
We recognize the limitation regarding the surveys used in this study as they are not previously validated. With further testing, we hope this can change and provide even stronger statistical support for validation based on these surveys. The small sample size of respondents provides a further limitation to being able to generalize our results, however, as a pilot study it has provided an adequate starting point for further investigation.
Conclusion
This novel CBLE was successfully implemented within a 2-h teaching session and improved knowledge on recognizing food insecurity in practice. However, additional learning exercises are likely needed to improve knowledge of the relationship between food insecurity and chronic disease states. Limitations include a small sample size and it being implemented at one institution. Nonetheless, the CBLE structure provided students with multiple formats of learning and integration of skills. Given our ongoing focus on expanding student understanding of pertinent SDOH in patient care, this model of knowledge-problem solving-implementation all within the space of an afternoon session, appears to be feasible and effective. As our healthcare system moves forward in much-needed changes to the routine use of screening and referral systems for addressing social determinants of health, integrating curricular elements such as this early in medical student education will better prepare students for their roles in clinical teams and for overall patient care.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231203967 - Supplemental material for A Novel Case-Based Learning Activity With a Focus on Food Insecurity
Supplemental material, sj-docx-1-mde-10.1177_23821205231203967 for A Novel Case-Based Learning Activity With a Focus on Food Insecurity by Brandon D Brown, Sean P Haley, Carole R Berini and Anita N Ramsetty in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-2-mde-10.1177_23821205231203967 - Supplemental material for A Novel Case-Based Learning Activity With a Focus on Food Insecurity
Supplemental material, sj-pdf-2-mde-10.1177_23821205231203967 for A Novel Case-Based Learning Activity With a Focus on Food Insecurity by Brandon D Brown, Sean P Haley, Carole R Berini and Anita N Ramsetty in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-3-mde-10.1177_23821205231203967 - Supplemental material for A Novel Case-Based Learning Activity With a Focus on Food Insecurity
Supplemental material, sj-pdf-3-mde-10.1177_23821205231203967 for A Novel Case-Based Learning Activity With a Focus on Food Insecurity by Brandon D Brown, Sean P Haley, Carole R Berini and Anita N Ramsetty in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors would like to thank the Medical University of South Carolina's SC Clinical Translational Research Institute for assistance in the development of the tools used in this study, as well as the Office of Assessment and the curriculum committee for their diligent review of the study proposed.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Partial funding of faculty time devoted to this study was provided by a grant from the Josiah Macy Jr Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.