
Abstract
Background
Pathophysiology bridges basic and clinical sciences, offering essential insights into disease mechanisms, diagnosis, and treatment. However, lecture-based learning remains predominant in China, often lacking dynamic evaluation systems. In alignment with the “Healthy China 2030” initiative, innovative methods such as problem-based learning (PBL), case-based learning (CBL), team-based learning (TBL), and seminar are increasingly explored to enhance integrated and competency-based medical education.
Methods
Sixty third-year clinical medicine students were randomly assigned to either a traditional instruction group or a Combi-Method group following a standardized preclass exam. The Combi-Method integrated PBL, CBL, TBL, and seminars. Instruction was based on real-world clinical cases. Knowledge acquisition was assessed through a postclass quiz, including multiple-choice, short-answer, and case study questions on renal, pulmonary, and hepatic insufficiency.
Results
The 2 groups exhibited comparable baseline characteristics in age, gender, and preclass scores. The Combi-Method group achieved significantly higher scores in several domains, particularly in renal and pulmonary insufficiency, and demonstrated superior clinical reasoning and knowledge application. Although some areas showed no statistical difference, the overall performance favored the Combi-Method.
Conclusions
The Combi-Method proves to be an effective instructional model for pathophysiology, promoting deeper understanding, enhanced clinical reasoning, and knowledge integration. This approach aligns with the goals of competency-based medical education and supports its broader adoption in undergraduate medical curricula.
Keywords
Introduction
Pathophysiology serves as a “bridge” discipline that links basic medical sciences with clinical medicine, focusing on the mechanisms and patterns of functional and metabolic changes in the body during the onset, progression, and resolution of diseases. 1 By integrating experimental evidence and theoretical models from disciplines such as biology, physiology, anatomy, chemistry, and biochemistry, pathophysiology provides indispensable scientific foundations for the development of disease prevention strategies, the refinement of diagnostic criteria, and the identification of therapeutic targets. 2 As it is deeply connected with various subjects covered in undergraduate medical education, pathophysiology offers an ideal entry point for breaking away from the traditional compartmentalized teaching approach.3,4 However, in China, the teaching of pathophysiology still predominantly relies on lecture-based learning.1,5 Instructors often depend on standardized midterm or final exams to assess students’ knowledge acquisition, lacking a continuous, dynamic formative evaluation process throughout the semester.6,7 Notably, a significant portion of educational research still uses final exam scores as the primary metric of teaching quality, underscoring the pressing need to reform evaluation systems. 5
As one of the most populous countries, China has launched the “Healthy China 2030” initiative—an important strategic framework aimed at advancing national and global health. 8 This plan explicitly identifies the reform of medical education as a key component in achieving its goals. 8 Given the unique educational context, cultural setting, and healthcare system in China, exploring and developing innovative teaching strategies tailored to these specific conditions is essential. Although some universities have begun to adopt innovative teaching approaches in courses like pathophysiology, the demonstrative impact and scalability of these reforms remain limited.3,4,8 Therefore, effectively integrating innovative methods into medical curricula requires not only identifying appropriate pedagogical pathways but also addressing the optimal allocation of limited instructional time between traditional and modern modalities. Building a well-structured and efficiently operated integrated curriculum system is critical to enhancing the impact and scalability of these innovations.
Among the many innovative teaching methods, problem-based learning (PBL) and case-based learning (CBL) have been widely demonstrated to enhance students’ depth of knowledge acquisition and application skills in medical education.9–11 These methods are particularly effective in cultivating clinical decision-making, differential diagnostic thinking, and interdisciplinary knowledge integration.11,12 PBL uses open-ended questions to promote self-directed learning, critical thinking, and deeper conceptual understanding. In contrast, CBL employs structured clinical cases to create contextualized learning environments that emphasize clinical reasoning and practical skills. Both approaches have shown promising outcomes in teaching complex diseases and are increasingly applied in international medical education settings.13,14 Their integration provides a more balanced and comprehensive learning experience. 11 Notably, their application in teaching specific diseases such as hepatocellular carcinoma in China has yielded encouraging results.15–17 Considering the central role of clinical cases in understanding pathophysiological mechanisms, the combined use of PBL and CBL holds significant potential to improve teaching efficacy in pathophysiology. 18
Implementation of PBL and CBL often requires students to engage in collaborative discussions and teamwork. 12 Therefore, combining team-based learning (TBL) and seminar with PBL and CBL to form a comprehensive instructional model is a promising direction. TBL is a student-centered pedagogical strategy that promotes active learning through a sequence of individual work, group collaboration, and immediate feedback. 19 Studies have shown that TBL enhances clinical reasoning skills, academic performance, classroom engagement, and learning satisfaction among medical students.20–22 Its core strength lies in fostering a strong sense of individual accountability and responsibility toward collective team goals, which is essential for students’ future clinical and research careers. 23 Meanwhile, seminar-based learning, characterized by in-depth academic discussions, is widely recognized for improving students’ scholarly capacity and communication skills. 24 The integration of TBL and seminars has already demonstrated educational value in foundational medical courses such as anatomy.25,26
This study proposes an innovative comprehensive instructional model that integrates PBL, CBL, TBL, and seminars into the teaching of pathophysiology. Under this model, the instructor's role shifts from a unidirectional knowledge transmitter to a facilitator and guide of learning. Through carefully designed PBL problems to stimulate inquiry, CBL cases to establish clinical context, TBL structures to ensure team efficiency and accountability, and seminar platforms to support deep academic discussion and reflection, this model aims to build a multidimensional, highly interactive, and competency-focused learning environment. It is anticipated that this integrated approach will better align pathophysiology education with modern medical education's emphasis on competency development, lifelong learning, and team collaboration. Ultimately, it may contribute to cultivating medical professionals with strong theoretical foundations, clinical capabilities, and well-rounded competencies—supporting the achievement of the “Healthy China 2030” strategic goals.
Methods
Research Participants
This study adopted a prospective randomized controlled design and recruited senior undergraduate students majoring in Clinical Medicine at the School of Medicine, Sun Yat-sen University. All participants were third-year undergraduate students majoring in clinical medicine. Only students who had completed and passed the core foundational preclinical courses biochemistry and molecular biology, physiology, histology and embryology, and systemic anatomy were eligible for inclusion. Students who had not successfully passed these prerequisite courses were excluded from the study. The study was conducted over a 3-month period from November 2024 to January 2025. During November and December 2024, students in both groups completed 6 class hours of instruction covering hepatic insufficiency, renal insufficiency, and pulmonary insufficiency. In January 2025, a 1-h quiz was administered to evaluate instructional effectiveness. A total of 60 students were enrolled and randomly assigned into 2 groups, with 30 students in each. Prior to the instructional intervention, all participants completed a preclass examination to assess their baseline understanding of pathophysiology (Figure 1). The 2 groups were subsequently taught using different instructional methods: 1 group received traditional lecture-based instruction, while the other underwent the Combi-Method, which integrated PBL, CBL, TBL, and seminar discussions. To enhance the comparability between groups, students in the traditional group also engaged in self-directed study of the same problems and cases used in the Combi-Method. Participation in this study was entirely voluntary and anonymous. All participants were informed of their right to withdraw at any stage without penalty.

Sixty students who voluntarily participated in the study were randomly divided into 2 groups (30 students in each group) after completing standardized preclass tests. Students respectively received traditional teaching and combined method teaching. The relative effectiveness of the comprehensive method compared with traditional teaching was evaluated through after-class tests, and the test process was anonymized.
Question Development and Assessment Procedure
Question Development
Basic discipline experts: 2 pathophysiology lecturers (associate senior or above, with at least 8 years of teaching experience).
Clinical team: 3 senior physicians (1 each in nephrology, respiratory medicine, and hepatology), all with ≥ 5 years of clinical experience and resident training.
Educational assessment consultant: 1 member of the Medical Education Evaluation Center (Master of Medical Education, proficient in Bloom's Taxonomy and multiple choice question [MCQ] development standards). To ensure that the pretest and posttest forms were psychometrically equivalent in difficulty, reliability and score scale, we implemented a parallel-form design with a priori equating:
① Common-item blueprint (20% anchor)
Both forms were built from an identical 20-item bidirectional matrix (renal 5, pulmonary 5, hepatic 5, integration 5). Three items per organ system (total 9, 45%) were kept intact as common anchor items with identical stems, options and scoring rubrics; the remaining 11 items were isomorphs (same cognitive level, same key concept, new surface context). Anchors were randomly dispersed across positions 3, 8, 13, 18 to minimize memory bias.
② A priori difficulty calibration
Before the RCT, both forms were administered to an independent sample (n = 42, 2023-cohort volunteers) under timed conditions. Classical difficulty index (P) and point-biserial (rpb) were computed. Items whose |Ppre – Ppost| > 0.10 or |rpb| < 0.20 were rewritten or replaced. After 2 iterations, the 2 forms showed:
− mean P 0.62 ± 0.08 versus 0.61 ± 0.09 (P = .83, paired t); − Cronbach's α 0.78 versus 0.80; − Fisher's z-transformed α difference 0.02 (95% CI [−0.11, 0.15]), ie, α equivalence. ③ Post-hoc equating check
Following the RCT, anchor-item scores were used for Mantel-Haenszel delta-plot equating. The equating shift was negligible (Δ = 0.6 raw-score points, SEM = 0.4). After equating, the experimental versus control group effect size changed by < 0.02 Cohen's d units, confirming that any observed difference is attributable to the intervention rather than form difficulty.
④ Reliability generalization
Separate α coefficients for each form in the RCT sample (n = 60) were 0.79 (pre) and 0.81 (post), with Feldt's test showing no significant difference (P = .62).
Thus, the pretest and posttest can be treated as statistically parallel and fair indicators of learning gain.
Finally, all items underwent 2 rounds of c until the content validity index (CVI) reached ≥0.83,27,28 at which point the items were officially included in the test.
Assessment Implementation and Evaluators
The examination was fully supervised by 2 administrative staff members from the Teaching Office, with instructors absent from the venue. The scoring process implemented 3 separate evaluations: MCQs were automatically graded using machine-readable cards without teacher involvement; short answer questions (SAQs) and case study answer questions (CSQs) underwent anonymous dual evaluation by 2 independent assessors (A and B), both being young pathophysiology instructors (PhD holders with ≥3 years of teaching experience) who did not participate in teaching. If the score difference exceeded 10%, a third-party chief physician-level arbitrator (uninvolved in teaching) would mediate. All questions were scored using a preestablished 0-5-point quantitative rubric (including key scoring criteria). Posttraining interrater Kappa = 0.82 ensured consistent and reliable scoring standards.
Conflict of Interest Control
The instructor is solely responsible for providing teaching materials and does not participate in the final review or grading of exam questions. The entire question-setting and grading process is conducted anonymously, with students’ names and group information being removed. Grades are entered by independent staff from the teaching office and only disclosed to the instructor after being locked in the database, ensuring an objective and fair evaluation process.
Instrument Validation
Validity Types and Validation Methods
Since this test gauges the relative impact of 2 teaching methods on knowledge acquisition and clinical reasoning, we center on content and response-process validity—the 2 sources that most directly protect the causal inference that any posttest difference is attributable to the intervention rather than to construct-irrelevant variance.29–31
① Content validity Complete in 3 steps:
“Bidirectional Detailed List” mapping: Developed by 2 pathophysiology lecturers and 3 attending physicians from nephrology, respiratory medicine, and hepatology departments, this system ensures each question corresponds to specific knowledge points in the syllabus (5 core concepts for renal, pulmonary, and hepatic failure respectively). Item-importance scoring: Using Lynn's (1986) 4-point scale, 6 experts from the university and affiliated hospitals (1:1 ratio of basic to clinical) were invited to rate 18 items as “representative.” Items with an Item-level CVI (I-CVI) ≥ 0.83 were deemed acceptable, while others were revised or removed. The final overall S-CVI/Average = 0.91. Pretest: A pretest was administered to 20 students from the 2023 cohort who were not included in the formal trial. As evidence of internal structure, items whose correlation with the total score was r ≥ 0.40 were retained; 2 multiple-choice items falling below this threshold were removed. Two low-correlation multiple-choice questions were replaced. ② Validity of the reaction process
The think-aloud method was employed: 8 randomly selected students orally articulated their reasoning while answering questions. Two researchers independently coded the responses, confirming 88% consistency between students’ actual thought processes and the expected cognitive hierarchy (memory → understanding → application), indicating the questions were unambiguous and nonmisleading.
Problems and Cases for Discussion
The problems and clinical cases used in the pathophysiology instruction were derived from real-world clinical scenarios, aiming to bridge theoretical knowledge with practical application and to enhance classroom engagement and relevance. These materials were collected from clinical departments by frontline physicians affiliated with the Department of Pathophysiology and were selected as representative and typical cases. Patient-identifiable information and final diagnoses were removed to ensure privacy; however, all contextual elements—such as patient history, physical examination findings, and laboratory test results—were preserved. Based on these cases, instructors designed targeted problems aligned with the course syllabus, with the goal of covering key concepts and fostering the integration of systematic knowledge. This approach was intended to deepen students’ comprehension of pathophysiological mechanisms and their clinical applications.
Instructional Implementation
The instructional sessions were jointly conducted by faculty members specializing in basic medical sciences and clinicians from frontline departments. Prior to engaging in problem and case discussions, all students were required to complete a 30-min structured review of relevant fundamental knowledge in pathophysiology. Students in the Combi-Method group proceeded to in-depth discussions under the dual guidance of basic science instructors and clinical physicians, facilitating the integration of theoretical and clinical perspectives.
Instructional Effectiveness Assessment
To evaluate knowledge acquisition under both instructional models, a postdiscussion quiz was administered following the case-based sessions (Figure 1). The assessment included:
MCQs: Five items each focusing on renal, pulmonary, and hepatic dysfunction. SAQ: One item specifically targeting renal failure. Case study questions (CSQs): One case each addressing pulmonary and hepatic dysfunction.
The content areas assessed included respiratory failure, acute respiratory distress syndrome, chronic obstructive pulmonary disease, hepatic encephalopathy, hepatorenal syndrome, and both acute and chronic renal failure. The test scores of students in the Combi-Method group were compared with those in the traditional lecture group to evaluate the differential effectiveness of the 2 teaching strategies.
Analysis of MCQs
Distractor Analysis
All 20 MCQ options were scrutinized with the 60 examinees. For every distractor we computed the “endorsement rate” in the lower-scoring 27% group; a good distractor should be selected by ≥ 5% of these candidates (Haladyna, 2021). Two options in Q-4 (renal) were chosen by only 1% and 2% respectively → ineffective. Both were rewritten and repiloted (n = 20); revised options now achieve 9% and 11% endorsement without altering difficulty (P moved from 0.64 → 0.62). No other distractor fell below the 5% cutoff.
Problem-Item Flagging and Action
Postrevision, all items meet: 0.30 ≤ P ≤ 0.80, rpb ≥ 0.36, D ≥ 0.30.
No negative discrimination or “all-correct” patterns remained; consequently no item was deleted from the final test form.
Baseline Equivalence of Groups
Pretest comparison (Traditional vs Combi-Method): mean 42.1 ± 6.3 versus 41.8 ± 6.5%, t(58) = 0.19, P = .85, d = 0.05.χ² on gender, prior GPA band, and repeat-exam history: all P > .40.
Thus the 2 groups were statistically equivalent before the intervention, satisfying the assumption of baseline comparability.
Analysis Method Difficulty Index (P)
Measures the percentage of correct answers per question,31–33 with P-values ranging from 0 to 1. A range of 0.3 to 0.8 is generally considered appropriate. Discrimination Index (D): Using the “upper versus lower 27%” method, it calculates the difference in correct answer rates between high and low score groups for the item. A D-value ≥0.3 indicates good discrimination. Point-biserial correlation (rpb): Measures the relationship between correct answers per item and total score, with rpb ≥ 0.2 considered acceptable.
Analysis Results (N = 60)
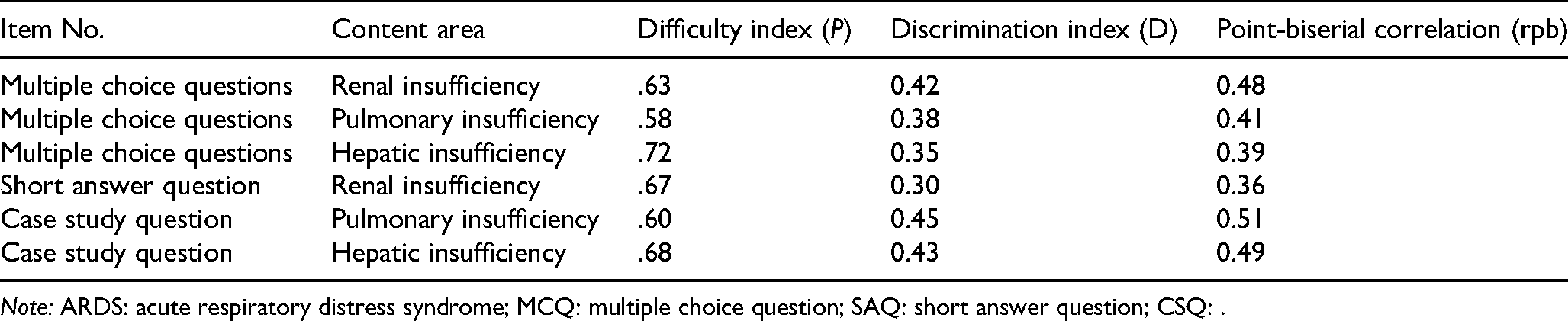
Note: ARDS: acute respiratory distress syndrome; MCQ: multiple choice question; SAQ: short answer question; CSQ: .
All questions demonstrated moderate difficulty (P = .58-.72) and good discrimination (D ≥ 0.30, rpb ≥ 0.36), with no items excluded due to excessive difficulty, excessive simplicity, or negative discrimination.
Fairness Test Intergroup Comparison
The chi-square test revealed significant differences between the Traditional and Combi-Method groups in only 1 item (MCQ1: Renal Failure Mechanism, χ² = 4.32, P = .038), while no significant differences were found in other items (P > .05). This suggests the test demonstrates good overall fairness. Preliminary DIF analysis: Due to sample size limitations, we conducted only the Mantel-Haenszel test (combining male and female groups). No significant DIF effect was found (OR ≈ 1.0, P > .05), indicating no systematic bias in the item design toward either gender.
Cognitive Level Assessed
The assessment totaled 47 points, with memory comprising just 5 points and comprehension accounting for 10 points. The remaining 68% of the score (14 points for Application and 18 points for Analysis) was concentrated in the Application and Analysis tiers, fully aligning with the core objectives of research to enhance clinical reasoning and knowledge integration.
Statistical Analysis
Statistical comparisons between the 2 groups were performed using an unpaired t-test or chi-square test. GraphPad Prism 10.4.1 software was used for data analysis. A 2-sided P-value of less than .05 was considered statistically significant. Significance levels were defined as P < .05 (*), P < .01 (**), P < .001 (***).
Results
Baseline Characteristics of the Participants
A total of 60 medical students participated in this study, who were divided into 2 groups based on the type of instructional intervention they received. The Traditional group consisted of 30 students (14 male, 16 female) with a mean age of 20.17 ± 0.46 years. The Combi-Method group also included 30 students (13 male, 17 female), with a mean age of 21.23 ± 0.50 years (Table 1). Age is expressed as “mean ± SD.” Before the course officially began, all participants underwent the same precourse instructional arrangement, including identical self-directed learning materials, study time, and a preclass examination. This was to ensure that the 2 groups had comparable levels of knowledge preparation before the instructional intervention. A further comparison of the preclass exam scores between the 2 groups revealed no statistically significant differences (P > .05) (Table 1). This indicates that the 2 groups had good baseline comparability, making them suitable for comparative evaluation of teaching effectiveness.
Bloom's Cognitive Level and Question Type Distribution Across Topics.

Postclass Quiz Results
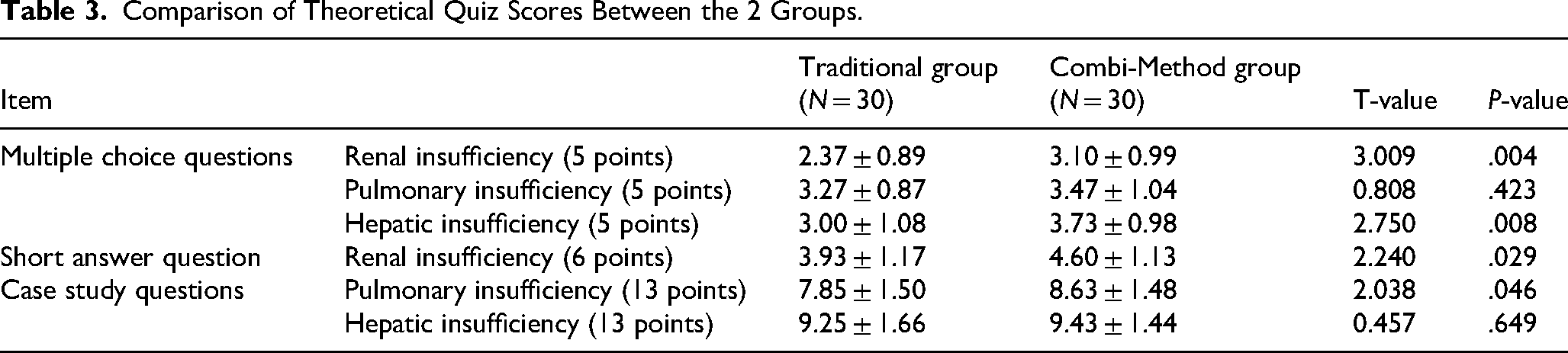
The results of the postcourse assessment (Tables 2, 3 and Figure 2) demonstrated that, for the MCQs related to pulmonary insufficiency, there was no significant difference in scores between the Traditional and Combi-Method groups, indicating comparable levels of knowledge acquisition for this specific topic. Similarly, no statistically significant difference was observed in the Case Study Questions focusing on hepatic insufficiency. However, the Combi-Method group exhibited significantly better performance in several other assessment components. In the MCQs covering renal insufficiency and hepatic insufficiency, students in the Combi-Method group achieved notably higher scores than those in the Traditional group. Additionally, for the open-ended Short Answer Question on renal insufficiency, the Combi-Method group demonstrated greater accuracy and logical organization in their responses, reflecting stronger clinical reasoning skills. In the Case Study Questions related to pulmonary insufficiency, the Combi-Method group also outperformed their counterparts in terms of case analysis, key point identification, diagnostic inference, and formulation of treatment strategies. Although the difference in scores for the hepatic insufficiency Case Study Question did not reach statistical significance, the overall trend suggested a potential advantage of the Combi-Method approach in facilitating students’ comprehension and application of complex pathophysiological concepts.

Comparison of theoretical quiz scores in traditional group (N = 30) and combi-method group (N = 30). (A) the scores of multiple choice questions related to renal, pulmonary, and hepatic insufficiency. (B) the scores of short answer question related to renal insufficiency. (C) the scores of case study questions related to pulmonary and hepatic insufficiency.
Comparison of the Baseline Characteristics.

Comparison of Theoretical Quiz Scores Between the 2 Groups.
Discussion
As a pivotal discipline bridging basic medical sciences and clinical medicine, pathophysiology plays a crucial role in guiding students toward both medical research and clinical practice. 1 In the context of international medical education, an increasing number of educators advocate for the early exposure of medical students to clinical and research experiences. However, such integration should not be limited to extracurricular activities but rather be systematically embedded within theoretical curricula to prevent the disconnection between theory and practice.34–36 To address this, we initiated educational reforms in pathophysiology as an entry point, promoting the concept of “earlier clinical exposure.” Specifically, the reform measures included allocating a portion of class hours within the theoretical courses to implement the Combi-Method approach. This restructuring of the curriculum aims to ensure that students systematically master the subject's knowledge framework while simultaneously reinforcing their understanding of the contextual application of that knowledge through practical experience. An analysis of the performance of students participating in case-based discussions on renal insufficiency, pulmonary insufficiency, and hepatic insufficiency revealed that the Combi-Method group significantly outperformed the Traditional control group in related test items. This integrative instructional model effectively enhanced students’ understanding of the relationship between disease mechanisms and clinical manifestations, confirming its positive impact on knowledge internalization and its application. These findings align with previous reports advocating for the integration of clinical cases into pathophysiology teaching, further supporting the effectiveness of this teaching model in enhancing educational outcome.18,37,38
In terms of instructional methodology, this study innovatively applied a Combi-Method integrating PBL, CBL, TBL, and seminar to pathophysiology education. This multimodal approach, to a certain extent, draws on Keller's ARCS motivational model—comprising Attention, Relevance, Confidence, and Satisfaction. 39 The element of Attention was addressed by utilizing real clinical cases to engage learners; Relevance was reinforced by connecting theoretical content with current research and clinical practice; Confidence was fostered through the design of appropriately challenging tasks that allowed students to build mastery incrementally; and Satisfaction was enhanced through the incorporation of student feedback and responsiveness to their learning needs. The ARCS model has shown great promise in the study of various diseases. 40
Although PBL, CBL, TBL, and seminar-based methods have been individually or jointly applied in various disciplines and instructional contexts, their comprehensive integration remains relatively novel. Prior studies have demonstrated, for example, the combined use of PBL and CBL in teaching hepatocellular carcinoma, and the integration of TBL and seminars in anatomy instruction.15,25 These educational practices highlight that the fusion of multiple teaching strategies is becoming an increasingly effective avenue for educational innovation, particularly in addressing the complexities of modern medical learning. In this study, we constructed a multilevel, interactive, and competency-centered instructional framework by integrating all 4 approaches. This composite model transcends the limitations of traditional single-method instruction and represents a pedagogical strategy more aligned with contemporary education's emphasis on integration and student-centeredness.
Based on the comparative analysis of theoretical quiz results, students receiving the Combi-Method consistently demonstrated superior performance across most assessment items, particularly in knowledge areas related to renal and hepatic insufficiency. These findings suggest that the Combi-Method enhances students’ comprehension of fundamental mechanisms and improves their ability to integrate and apply knowledge in clinical contexts. However, no significant difference was observed in the multiple-choice items on pulmonary insufficiency or the case analysis question on hepatic insufficiency. These findings may indicate areas for further optimization in instructional design or content structure for these specific topics. Overall, the combinatorial instructional model demonstrated strong educational efficacy, especially in conveying complex concepts and cultivating higher-order cognitive skills. We recommend its broader implementation in future pathophysiology education and suggest that areas showing nonsignificant differences be subject to further instructional refinement and targeted design improvements.
Looking ahead, as the concepts in medical education continue to evolve, pathophysiology, as a bridging discipline between basic and clinical sciences, is gradually moving toward a model that deeply integrates basic medical education with clinical practice. Future pathophysiology education will not only focus on disease mechanisms but will also emphasize their practical applications in clinical diagnosis, treatment, and decision-making. Therefore, the integration of CBL with mechanism analysis becomes a critical component of educational reform. In terms of teaching methods, interactive models such as PBL, CBL, TBL, and seminar will be more widely applied in the classroom. By constructing real or simulated clinical scenarios, these methods aim to guide students toward active inquiry and collaborative learning, thereby enhancing their ability to perform comprehensive analysis and foster clinical reasoning. This pedagogical transformation not only deepens students’ understanding of pathophysiological knowledge but also significantly strengthens their ability to link theory to practice, laying a solid foundation for their future competence in clinical practice.
Inevitably, there are some limitations in our reform. Given that the students are still beginners, the cases we used mainly focused on single-organ dysfunction, whereas real clinical cases are often more complex. Constructing a structured framework for teaching multiple disease comorbidities at the undergraduate level may be beneficial for further understanding pathophysiology. 41 Second, the evaluation of instructional effectiveness relied on a single postsession test. This design primarily reflects short-term knowledge retention and does not capture whether learning can be sustained, transferred, or generalized to more complex clinical decision-making contexts. Future studies may incorporate longitudinal assessment designs and competency-based evaluation frameworks to more accurately characterize learning trajectories and performance growth over time. Furthermore, the study was conducted with a relatively small cohort within a single institution and lacked longer-term follow-up, which constrains the external validity of the findings. Given the fixed class size and limited available sample, no formal sample size calculation was performed. Instructor-related variability may also have introduced uncontrolled instructional influences. Additional research is needed to determine the feasibility and contextual adaptability of this integrated approach across institutions with different curricular structures and sociocultural environments. Large-scale, multisite HPE studies are therefore warranted to further establish generalizability and to examine whether such curriculum reform contributes to downstream development of core competencies, including collaboration and communication, rather than merely improving conceptual understanding. Continuous iterative refinement will remain necessary as undergraduate pathophysiology progressively transitions toward more integrated instructional designs that foster professional confidence through repeated practice and better prepare learners for future clinical roles.42,43
Conclusions
The combined application of PBL, CBL, TBL, and seminar-based strategies proves to be a viable and effective pedagogical model for pathophysiology instruction. It facilitates the integration of foundational and clinical knowledge, contributing to the enhancement of students’ overall competency in accordance with the objectives of competency-based medical education.
Footnotes
Acknowledgments
We extend our sincere appreciation to the instructors and students whose invaluable participation in this study.
Ethical Considerations
This study did not require approval from the institutional review board.
Consent to Participate
This study has received formal ethical approval from the Medical Ethics Committee of the Seventh Affiliated Hospital of Sun Yat-sen University (Approval No. KY-2025-525-01). A copy of the approval document has been uploaded as supplemental material. Written informed consent was obtained from all participants prior to the initiation of the study.
Author Contribution
All authors have met the ICMJE criteria for authorship, have read and approved the final manuscript, and have made the following contributions: conceptualization: Jiancheng Wang and Xiaofeng Cen; methodology: Jiayu Huang and Yuqing Yao; formal analysis and investigation: Peng Wu, Kongyang Ma, and Nan Wang; writing—original draft preparation: Peng Wu and Xiaofeng Cen; writing—review and editing: Xiaofeng Cen, Shuo Fang, and Jiancheng Wang; funding acquisition: Jiancheng Wang; resources: Jiancheng Wang, Shuo Fang, and Kongyang Ma; supervision: Jiancheng Wang.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Guangdong University Quality Assurance Project (Grant No. 78000-12253001); Research Start-up Fund of the Seventh Affiliated Hospital, Sun Yat-sen University: ZSQYRSSFAR0003.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All data supporting the conclusions of this research are available upon reasonable request from the corresponding author.