
Abstract
This study used administrative data to compare the socio-demographics, health conditions, and health service use of autistic adults with adults with and without other developmental disabilities, after matching for age and sex. Autistic women and men were more likely to have a wide range of physical and mental health conditions compared to adults without developmental disabilities. Rates of co-occurring health conditions were similar or lower among autistic adults compared to adults with other developmental disabilities, except for a higher prevalence of psychiatric conditions among autistic adults. Notably increased psychiatric service use was evident among autistic women and men compared to the other groups. Among age-matched autistic women and men, significant differences were found for physical (i.e. Crohn’s disease/colitis, rheumatoid arthritis) and psychiatric conditions (i.e. psychotic disorders, non-psychotic disorders), as well as service use (i.e. emergency department visits, hospitalizations, family doctor and neurologist visits). These findings suggest autistic adults have high health care needs, as do adults with other developmental disabilities. Mental health support is especially critical for autistic adults and research examining sex and gender effects will assist in tailoring health promotion and intervention efforts.
Lay abstract
This study used administrative data from Ontario, Canada to compare the health conditions and service use of autistic women and men with adults with other developmental disabilities and with adults without developmental disabilities. Autistic women and men were more likely to have physical and mental health conditions compared to adults without developmental disabilities. Rates of health conditions were similar or lower among autistic adults compared to adults with other developmental disabilities, except more autistic adults had psychiatric conditions. Autistic women and men used higher rates of psychiatric services compared to all other groups. When comparing autistic women with same aged autistic men, sex differences were found for specific physical (Crohn’s disease/colitis, rheumatoid arthritis) and psychiatric conditions (psychotic disorders, non-psychotic disorders), as well differences in service use (emergency department visits, hospitalizations, family doctor and neurologist visits). These results further highlight the high health needs and service use of autistic women and men, as well as adults with other developmental disabilities. It is critical for future research to focus on mental health support for autistic adults and to better understand how to tailor supports to best serve autistic women.
A small but steadily increasing number of studies using administrative data demonstrate that autistic adults have elevated physical health and psychiatric conditions (Cawthorpe, 2017; Chiang et al., 2015; Croen et al., 2015; Davignon et al., 2018; Hand et al., 2019; Kohane et al., 2012; Schott et al., 2022a, 2022b; Smith DaWalt et al., 2021; Tint et al., 2021; Tyler et al., 2011; Vohra et al., 2017; Weiss et al., 2018) and higher health service use rates (Ames et al., 2021; Hand et al., 2018; Smith DaWalt et al., 2021; Vohra et al., 2016, 2017; Weiss et al., 2018; Zerbo et al., 2019) compared to the general population. The majority of these studies, however, are comprised predominantly of young adult males (Cawthorpe, 2017; Chiang et al., 2015; Davignon et al., 2018; Kohane et al., 2012; Tyler et al., 2011; Weiss et al., 2018) and many do not include sex-stratified analyses to allow for an understanding of autistic women’s patterns of need. This is particularly concerning as autistic adults are at higher risk of premature mortality than non-autistic adults (Lunsky, Lai, et al., 2022), with some evidence of increased risk for autistic women compared to men (Akobirshoev et al., 2020). To improve health outcomes and inform appropriate service provision across adulthood, we need a more comprehensive understanding of the health needs and service use patterns of autistic women and men at the population level.
The handful of population-based studies to date comparing health outcomes of autistic women with those of autistic men point to elevated health risks for the female sex (Croen et al., 2015; Davignon et al., 2018; Smith DaWalt et al., 2021). For instance, in a US-based study, Croen et al. (2015) did not compare sex differences statistically, though they found autistic women were diagnosed more frequently than autistic men with immune conditions, cancer, cardiovascular diseases, metabolic diseases, endocrine disorders, neurologic diseases, gastrointestinal diseases, sleep conditions, nutrition conditions, genetic and other medical disorders, with the exception of lower gastrointestinal, hepatic, and genitourinary diseases. In terms of psychiatric conditions, a higher percentage of autistic women were diagnosed with anxiety, bipolar disorder, dementia, depression, schizophrenic disorders, other psychoses, and suicide attempts compared to autistic men (Croen et al., 2015). When comparing autistic adults’ health outcomes with sex-specific general population comparison groups, autistic men are at increased risk for a range of co-occurring conditions, and the emerging research suggests that when compared to women in the general population, autistic women’s increased risk for co-occurring conditions is especially pronounced for certain physical health (e.g. epilepsy, diabetes, stroke, endocrinological conditions) and psychiatric conditions (e.g. psychotic disorders, obsessive-compulsive disorder, depressive disorders; Kassee et al., 2020; Simantov et al., 2021; Smith DaWalt et al., 2021; Tint et al., 2021).
High rates of health conditions among autistic women and men may necessitate intensive service use; however, research on adult service use is scarce and findings to date are inconsistent. In one of the few administrative data studies to date with sex-specific health service use findings, Zerbo et al. (2019) found autistic women and men had significantly higher use of outpatient primary care, mental health, and neurology services compared to women and men in the general population. However, gynecology visits and same-day hospitalizations were less common among autistic women compared to women in the general population. Among men, laboratory services and hospitalizations for ambulatory care sensitive diagnoses (conditions for which hospital admission could be prevented or delayed through primary care access and chronic disease management) were significantly more common among autistic men than those in the general population. Health service use was not directly compared between autistic women and men; however, survey-based and qualitative research has demonstrated higher service use, greater barriers to care, and less satisfaction with services received among autistic women compared to autistic men (Baldwin & Costley, 2016; Koffer Miller et al., 2022; Tint et al., 2017).
Recognizing the intersectionality of autistic adults with other social categories, inclusive of autistic and sex/gender-based roles and identities, the choice of comparison groups is key when studying profiles of health outcomes and service use. Of the relatively small number of studies that use sex-stratified analyses to examine health outcomes of autistic women, many studies either compare autistic women with women in the general population or with autistic men. However, Taylor and DaWalt (2020) highlight the need to understand sex/gender health and service need differences in the context of social determinants of health and associated vulnerabilities and marginalization associated with being autistic, being a woman or man, and/or being an autistic woman or man. This necessitates the need for comparing autistic women with autistic men, in addition to sex-stratified comparisons with the general population.
Extending this rationale, a further limitation of the research to date concerns the disentanglement of the unique patterns of service use of autistic women and men from those of adults with developmental disabilities (DD) other than autism (e.g. Down syndrome, fetal alcohol syndrome). This is important because if greater health concerns and higher service use rates are unique to autistic adults, this would speak to the need for tailored services for this population. Whereas, if health care needs and service rates are comparable across individuals with different types of DD, this would highlight a need for health care policies for a broader array of adults with developmental concerns.
There is growing evidence that both autistic adults and adults with other DD have higher levels of co-occurring physical health and psychiatric conditions and associated service use compared to the general population (Cooper et al., 2007; Havercamp et al., 2004; Jansen et al., 2004; Lunsky et al., 2013). Results are less clear, however, when comparing autistic adults to those with other types of DD. A Canadian study (Weiss et al., 2018) showed increased rates of co-occurring psychiatric conditions among young autistic adults (18–24 years old) compared to young adults with other DD, though young autistic adults were less likely to have physical health conditions such as asthma and hypertension. With respect to service use, young autistic adults were more likely to have at least one visit to the family physician and psychiatrist and were more likely to visit the emergency department (ED) for psychiatric reasons compared to young adults with other DD. However, they were less likely to have seen a respirologist or surgeon and to visit the ED overall; they were just as likely to be hospitalized and to visit the neurologist or the gastroenterologist, compared to young adults with other DD. Sex-stratified analyses of health conditions and service use, however, were not conducted.
We need more research to clarify specific as well as common patterns of health conditions and service use of autistic women and men in contrast with those with other DD, and those without DD. A better understanding of the unique health needs for which autistic women and men require improved service access and tailored care will enable health care systems to plan and implement effective service provision. In the current study, we used population-based data from Ontario, Canada to (1) characterize and compare common health conditions and health service use of autistic adults stratified by sex and (2) compare these characteristics to those of women and men with other DD and to those in the general population (without DD).
Methods
We conducted a population-based study in Ontario, which is Canada’s most populous province and has a publicly funded health care system. All residents of Ontario are eligible for universal coverage for basic and emergency health services, including physician, in-patient and ED care through the provincial health insurance plan. This project was completed as part of the Health Care Access Research and Developmental Disabilities (H-CARDD) program. The overall goal of the H-CARDD program is to monitor and improve the health and health care of Ontarians with DD through engagement with researchers, policymakers, health care planners, clinicians, adults with DD, and caregivers. The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act and does not require review by a Research Ethics Board.
Data sources
We analyzed administrative health and social service databases stored at ICES, an independent, non-profit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. Demographic data were obtained from the Registered Persons Database (RPDB), a registry of Ontario residents eligible for health insurance. Of note, this database provided information on sex assigned at birth, as defined by Ontario health records, but no information on gender. The Ontario Health Insurance Plan (OHIP) database was used to identify claims for physician services. ED visit data were obtained from the Canadian Institute for Health Information National Ambulatory Care Reporting System Database (NACRS). Hospital admission data were obtained from the Canadian Institute for Health Information Discharge Abstract Database (CIHI-DAD) and the Ontario Mental Health Reporting System (OMHRS), which includes detailed information regarding inpatient psychiatric care. Diagnostic data in the ED and hospital databases were recorded using the Canadian Coding Standards for the International Classification of Diseases and Related Health Problems (10th revision after 2002; ICD-10) or the Diagnostic and Statistical Manual of Mental Disorders, 4th edition. Physician visit data were recorded using billing claim and diagnostic codes. It is important to note that Ontario outpatient billing only permits a single billing code per visit. These datasets were linked using unique, encoded identifiers (e.g. name, address, birth date, sex, which are accessible only by the ICES data covenanter for the sole purpose of data linkage; Lin et al., 2014) and were analyzed at ICES in Toronto, Ontario, Canada.
Sample
We examined an existing cohort, henceforth referred to as the “primary cohort,” consisting of 66,484 Ontarians with DD aged 19–65 years as of 1 April 2010. In this primary cohort, individuals were considered to have DD if they had a documented diagnosis of intellectual disability, fetal alcohol syndrome, autism, and/or chromosomal and autosomal conditions (e.g. Down syndrome, Fragile X syndrome; see Supplemental Table S2 for full list). These diagnoses were identified in health administrative databases based on either ⩾ 2 physician visits or ⩾ 1 ED visit or hospitalization since birth or inception of each database (whichever occurred later) or based on disability income support program documentation (see Supplemental Tables S1 and S2). This definition of DD is based on the Ontario government’s definition used to determine eligibility for disability support services and is consistent with provincial legislation (Government of Ontario, 2010). DD conditions consistent with this definition within the above-mentioned databases were identified in consultation with clinicians and policymakers. Further information on methods for identifying the primary cohort of individuals with DD are described in detail in prior publications (Lin et al., 2014; Lunsky et al., 2013).
From this large primary cohort of adults with DD, autistic individuals were identified if they met one of the following criteria: (a) ⩾2 physician visits with an autism diagnosis code recorded since OHIP database inception (1991); (b) ⩾ 1 more hospital claim or ED admission with an autism diagnosis code since CIHI-DAD or NACRS database inception (1988 and 2002, respectively); or (c) autism was recorded as a diagnosis leading to eligibility for disability benefits from the Ontario Disability Support Program (Weiss et al., 2018). Prior research indicates using two physician visit codes for autism (Burke et al., 2014) and/or one from another source (e.g. hospitalization) has good specificity and moderate sensitivity when examining the validity of administrative health data relative to gold standard autism assessment methods (Dodds et al., 2009) and has been used in past research (Lunsky, Lai, et al., 2022; Weiss et al., 2018). Those not identified as autistic within the primary cohort were placed in the “other DD” group. The “without DD” group was comprised of a random sample of 20% of Ontario adults aged 18–64 years in fiscal year 2009 who were not identified in the primary cohort; no further exclusion criteria were used. Autistic adults were matched on sex and 5-year age group with adults with other DD (ratio 1 autistic adult:1 adult with other DD) and with adults without DD from the general population (ratio 1 autistic adult:4 adults without DD to increase the size of the comparison group). Autistic women were also matched 1:1 by age with autistic men.
Measures
Demographics
Age, sex assigned at birth (female, male), and postal codes of the residences of the study population on 1 April 2010 (index date) were identified from the RPDB. Information concerning gender identity, race, and ethnicity is not collected in Ontario health records and was, therefore, unavailable for this study. Neighborhood income quintiles were derived by linking 2006 Canadian Census data on area-level median income to residential postal codes. We classified neighborhoods as either rural or urban using the Rurality Index of Ontario, which uses 10 indicators to classify neighborhoods as urban (scores of 0–44) or rural (scores of ⩾ 45; Kralj, 2000).
Physical health conditions
We used validated algorithms using physician billing claim codes and ICD-9 and ICD-10 diagnostic codes to identify, as of 1 April 2010, epilepsy (Tu et al., 2014), diabetes (Hux et al., 2002), hypertension (Tu et al., 2007), chronic obstructive pulmonary disease (Gershon et al., 2009a), asthma (Gershon et al., 2009b), congestive heart failure (Schultz et al., 2013), Crohn’s disease and colitis (Benchimol et al., 2014), rheumatoid arthritis (Widdifield et al., 2014), and stroke (Tu et al., 2013) with a look-back period of 2 years (Lin et al., 2016; Weiss et al., 2018). We also identified a history of malignant conditions using the validated Ontario Cancer Registry (Hall et al., 2006). These physical health conditions were chosen as they are among those that past research has demonstrated to be common among autistic people (e.g. Weiss et al., 2018) and previously validated algorithms exist for their identification with the administrative health data, including recent studies with autistic and DD populations (Brown et al., 2016; Durbin et al., 2019; Lunsky, Durbin, et al., 2022; Tint et al., 2021; Weiss et al., 2018; Whittingham et al., 2020).
Psychiatric conditions
We identified individuals with psychotic and non-psychotic disorders and individuals with substance use disorders from physician billing claim codes and ICD-10-CA diagnostic codes (see Supplemental Table S2) in CIHI-DAD, OMHRS, NACRS and OHIP databases from 1 April 2008 to 31 March 2010. As in previous research (Lin et al., 2016; Weiss et al., 2018), psychiatric condition was defined as any ICD-10 F-code or equivalent codes from the ICD-9 or DSM (ICD-9/OHIP: 290–298, 300–316; ICD-10: F00–F69, F99), excluding codes for DD (see Supplemental Table S2).
Health service use
Service outcomes included any all-cause visit to primary care physicians, psychiatrists, respirologists, gastroenterologists, neurologists, obstetrician and gynecologists (OB/GYN for women only), and the ED, and any all-cause hospital admissions. We also examined ED visits and hospital admissions specifically for psychiatric concerns. Service outcome variables were identified from OHIP, NACRS, CIHI-DAD and OMHRS from 1 April 2010 to 31 March 2011.
Analyses
Standardized differences were used to examine the differences in socio-demographic characteristics between groups as they are not influenced by sample sizes as are p-values, and are therefore more appropriate for large population-based studies (Mamdani et al., 2005). A standardized difference ⩾ 0.10 is viewed as clinically meaningful (Austin, 2009). In addition, we calculated prevalence and risk ratios (RR) and neighborhood income quintile adjusted prevalence and risk-ratios (aRR) with 95% confidence intervals (CI) using log-binomial regression and accounted for matching. We calculated adjusted risk ratios rather than odds ratios because odds ratios can be a biased measure of risk when outcomes are common (greater than 10%) (Mcnutt et al., 2003). All analyses excluded those with missing neighborhood income quintile information (approximately 0.46% of autistic adults, 0.75% of adults with other DD, and 0.40% of adults without DD). Finally, to better understand similarities and differences in patterns of health concerns and service use among autistic women and men, analyses were conducted to directly compare a subsample of 3240 autistic women with age-matched autistic men. All analyses excluded those with missing neighborhood income quintile information. Analyses were conducted at ICES using SAS version 9.4.
Community involvement
Members of the autistic and autism communities were not directly involved in this project.
Results
A total of 10,646 autistic adults (of which 3220 were women) were identified. Descriptively, autistic women (Table 1) and men (Table 2) differed in age. We presented sex-stratified results below.
Demographic characteristics across groups with autism, other DD, and without DD: Women.
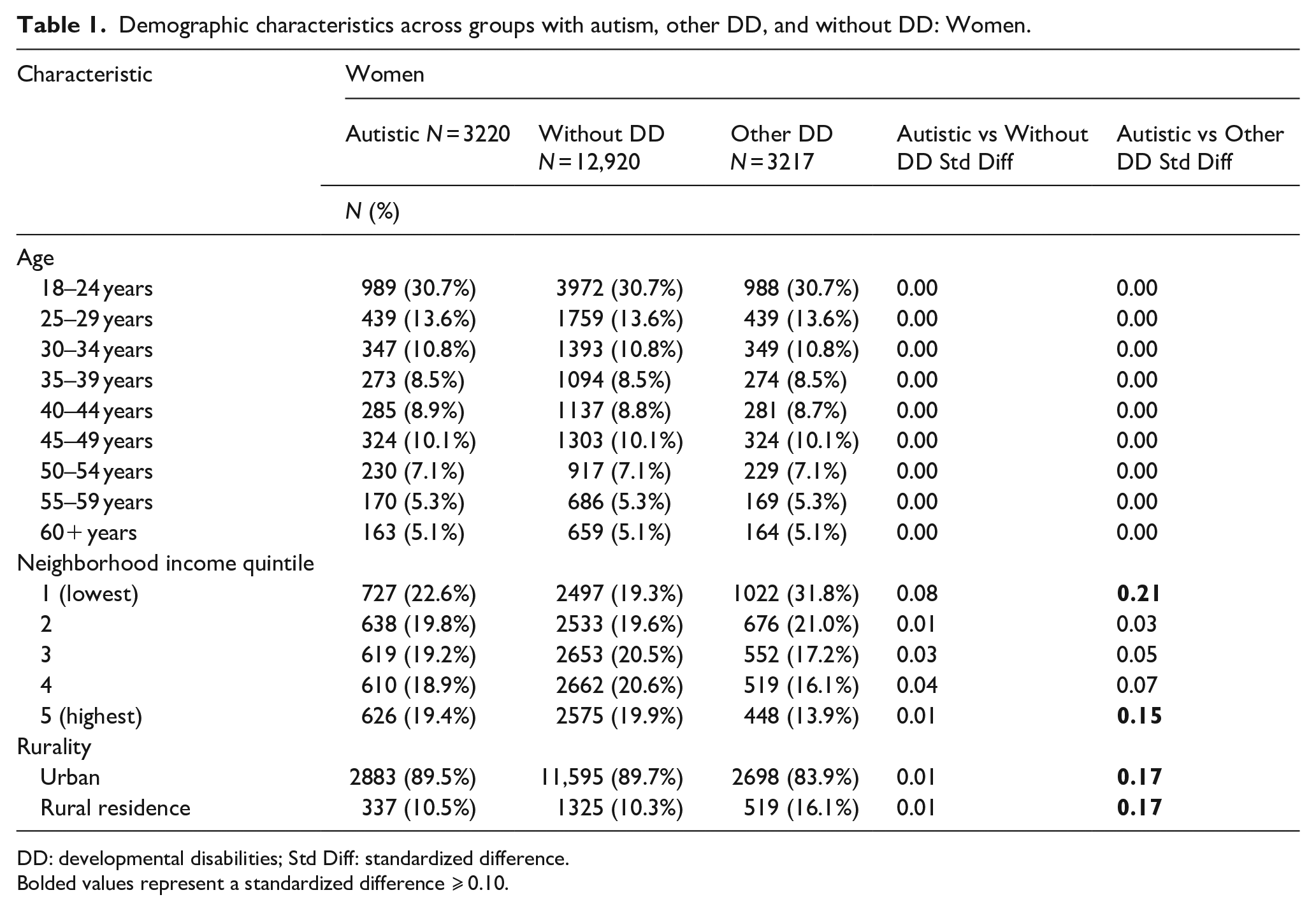
DD: developmental disabilities; Std Diff: standardized difference.
Bolded values represent a standardized difference ⩾ 0.10.
Demographic characteristics across groups with autism, other DD, and without DD: Men.
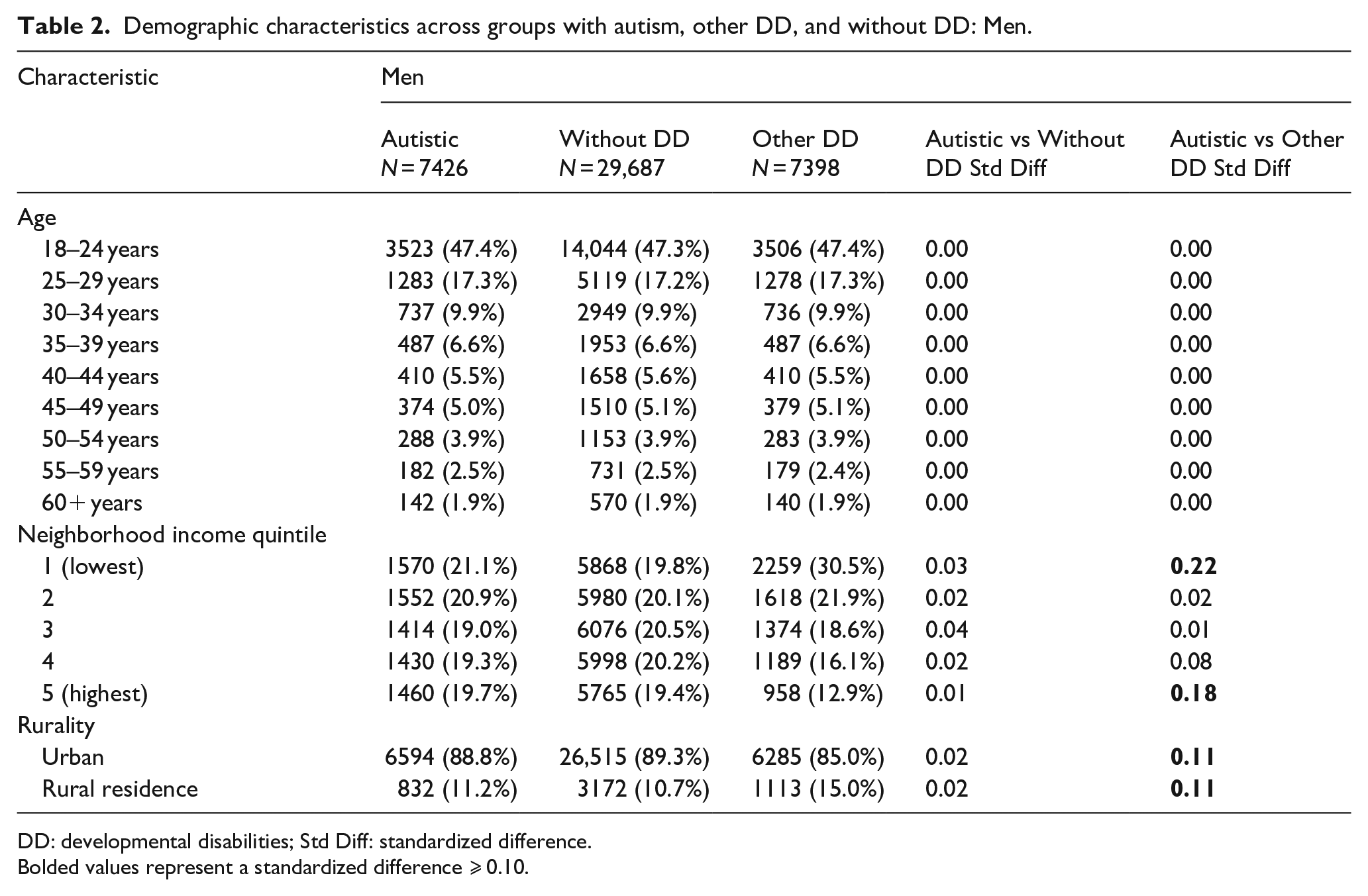
DD: developmental disabilities; Std Diff: standardized difference.
Bolded values represent a standardized difference ⩾ 0.10.
Socio-demographics
Socio-demographic characteristics for each sex are shown in Tables 1 and 2. Autistic women showed an equivalent pattern of distribution related to neighborhood income as women without DD. Compared to women with other DD, autistic women were less likely to come from the lowest quintile (22.6% vs 31.8%) and were more likely to be from the highest quintile (19.4% vs 13.9%). Autistic women were equally as likely to reside in rural regions compared to women without DD (10.5% vs 10.3%), yet less likely to reside in rural regions compared to women with other DD (10.5% vs 16.1%). Results about autistic men followed the same pattern (Table 2).
Physical health conditions
Compared to women without DD, autistic women were more likely to have epilepsy, diabetes, hypertension, chronic obstructive pulmonary disease, asthma, cancer, and stroke (Table 3). The greatest differences were for epilepsy (aRR = 17.10, 95% CI = 13.66–21.40), stroke (aRR = 2.25, 95% CI = 1.28–3.97), and diabetes (aRR = 2.00, 95% CI = 1.74–2.30). However, when compared to women with other DD, autistic women were less likely to have epilepsy (aRR = 0.75, 95% CI = 0.66–0.85) and diabetes (aRR = 0.84, 95% CI = 0.72–0.98). No differences were found for the prevalence of Crohn’s disease and colitis, congestive heart failure, or arthritis when comparing autistic women to women with other DD or women without DD.
Health and service use characteristics: Women.
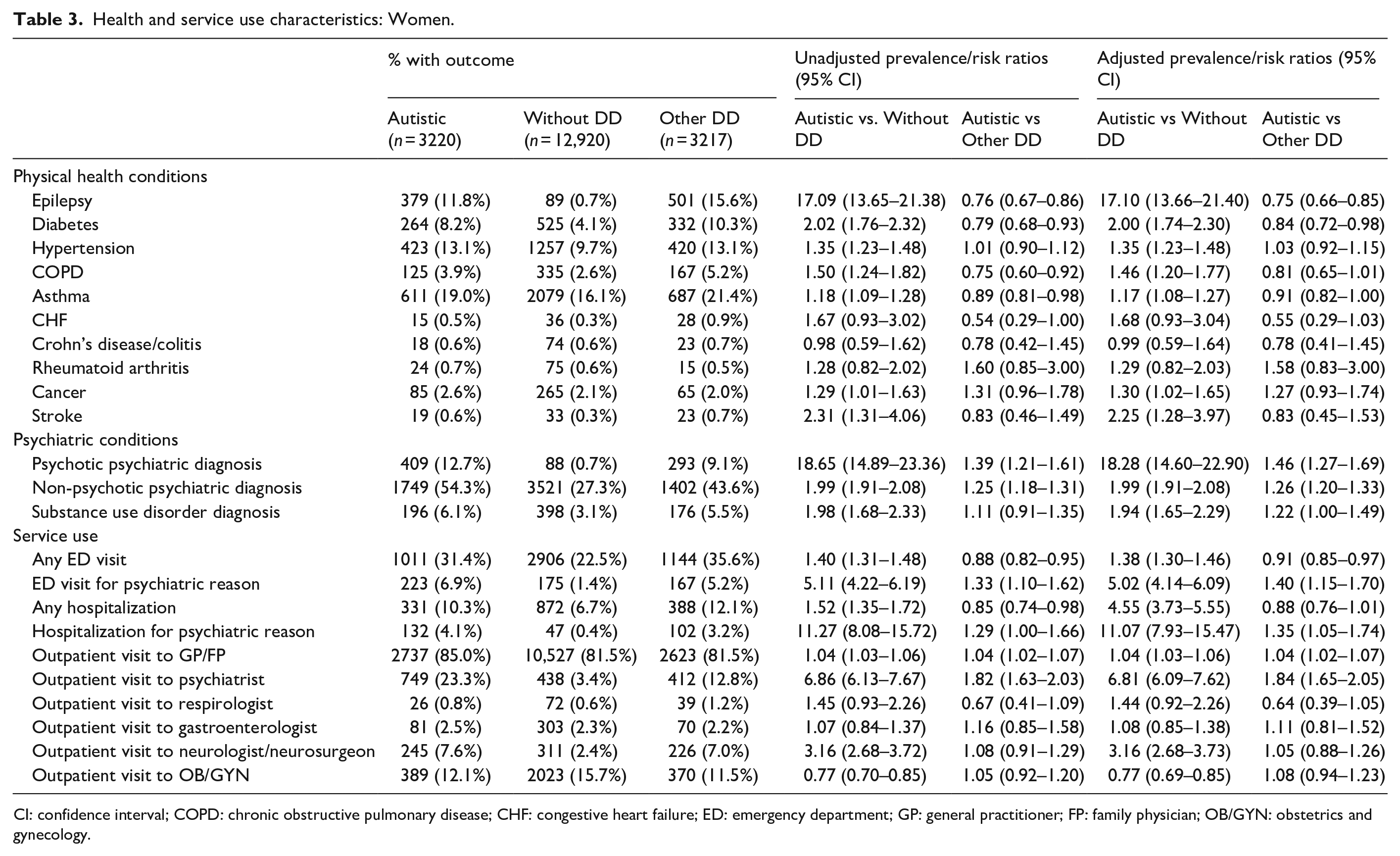
CI: confidence interval; COPD: chronic obstructive pulmonary disease; CHF: congestive heart failure; ED: emergency department; GP: general practitioner; FP: family physician; OB/GYN: obstetrics and gynecology.
Compared to men without DD, autistic men were similarly more likely to have physical health conditions, including epilepsy, diabetes, hypertension, chronic obstructive pulmonary disease, congestive heart failure, asthma, and cancer (Table 4). The most marked differences were for epilepsy (aRR = 13.72, 95% CI = 11.97–15.72), congestive heart failure (aRR = 2.82, 95% CI = 1.74–4.55), and diabetes (aRR = 1.69, 95% CI = 1.50–1.89). When compared to men with other DD, autistic men were less likely to have chronic obstructive pulmonary disease (aRR = 0.72, 95% CI = 0.58–0.89), asthma (aRR = 0.90, 95% CI = 0.85–0.96), and stroke (aRR = 0.52, 95% CI = 0.29–0.91). Prevalence of Crohn’s disease and colitis or arthritis did not differ among autistic men and the two comparison groups.
Health and service use characteristics: Men.
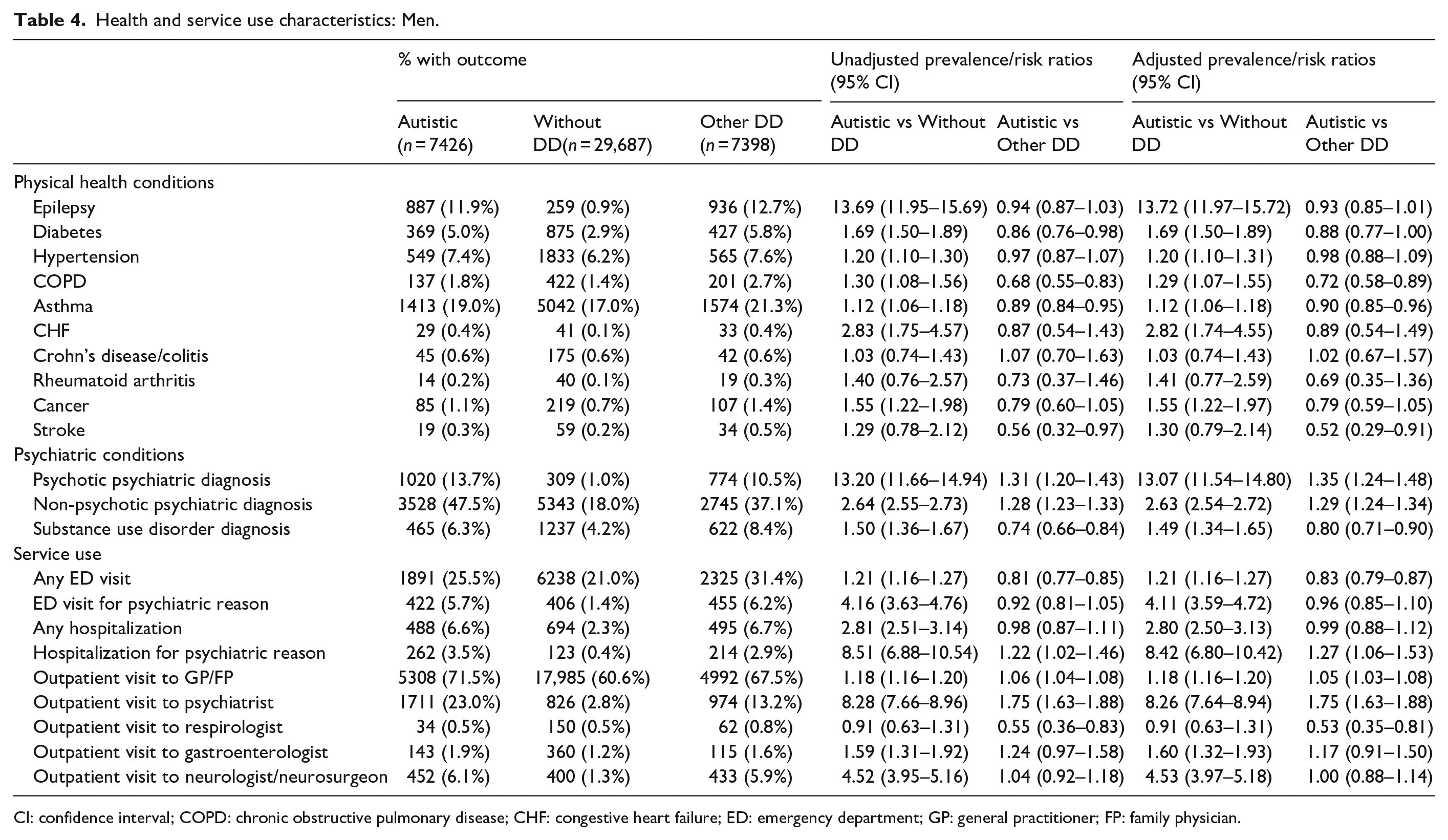
CI: confidence interval; COPD: chronic obstructive pulmonary disease; CHF: congestive heart failure; ED: emergency department; GP: general practitioner; FP: family physician.
Psychiatric conditions
Compared to women without DD, autistic women were more likely to have all psychiatric and substance use conditions (Table 3). Compared to women with other DD, autistic women were also more likely to have psychotic (aRR = 1.46, 95% CI = 1.27–1.69) and non-psychotic conditions (aRR = 1.26, 95% CI = 1.20–1.33), but the prevalence of substance use disorders did not differ.
Compared to men without DD, autistic men were more likely to have non-psychotic conditions and substance use disorders (Table 4). Compared to men with other DD, autistic men were more likely to have all psychiatric conditions except for substance use disorders, which were more prevalent in men with other DD.
Health service use
Compared to women without DD, autistic women were more likely to use all health services examined except for respirologist, gastroenterologist, and OB/GYN visits (Table 3). The greatest differences were for psychiatric hospitalizations (aRR = 11.07, 95% CI = 7.93–15.47), psychiatrist visits (aRR = 6.81, 95% CI = 6.09–7.62), and psychiatric ED visits (aRR = 5.02, 95% CI = 4.14–6.09). Compared to women with other DD, autistic women were more likely to visit a family doctor (aRR = 1.04, 95% CI = 1.02–1.07), psychiatrist (aRR = 1.84, 95% CI = 1.65–2.05), psychiatric ED (aRR = 1.40, 95% CI = 1.15–1.70), and to be hospitalized for a psychiatric reason (aRR = 1.35, 95% CI = 1.05–1.74). Autistic women were less likely to visit the ED overall compared to women with other DD (aRR = 0.91, 95% CI = 0.85–0.97), though hospitalizations for any reason did not differ significantly between the two groups.
In comparison to men without DD, autistic men were more likely to use all health services examined except for respirologists (Table 4). Marked differences were seen in psychiatric hospitalizations (aRR = 8.42, 95% CI = 6.80–10.42), psychiatrist visits (aRR =8.26, 95% CI = 7.64–8.94), and neurologist visits (aRR = 4.53, 95% CI = 3.97–5.18). Compared to men with other DD, autistic men were more likely to visit a family doctor (aRR = 1.05, 95% CI = 1.03–1.08), psychiatrist (aRR = 1.75, 95% CI = 1.63–1.88), and to be hospitalized for a psychiatric reason (aRR = 1.27, 95% CI = 1.06–1.53). Autistic men, compared to men with other DD, were less likely to visit a respirologist (aRR = 0.53, 95% CI = 0.35–0.81) and to visit the ED for any reason (aRR = 0.83, 95% CI = 0.79–0.87). Hospitalizations for any reason did not differ between autistic men and men with other DD.
Direct comparison between autistic women and men
A total of 3240 autistic women and age-matched autistic men were initially identified. Analyses excluded those with missing neighborhood quintile information, which resulted in a final sample comprised of 3220 autistic women and 3222 males. Autistic women and men did not differ in socio-demographics (Table 5). The prevalence of physical health conditions was largely similar between the sexes (Table 6) but with two exceptions: (1) autistic women were less likely to have Crohn’s disease or colitis (aRR = 0.55, 95% CI = 0.31–0.97) and; (2) autistic women were more likely to have rheumatoid arthritis (aRR = 3.02, 95% CI = 1.36–6.70).
Demographic characteristics across autistic women and autistic men.
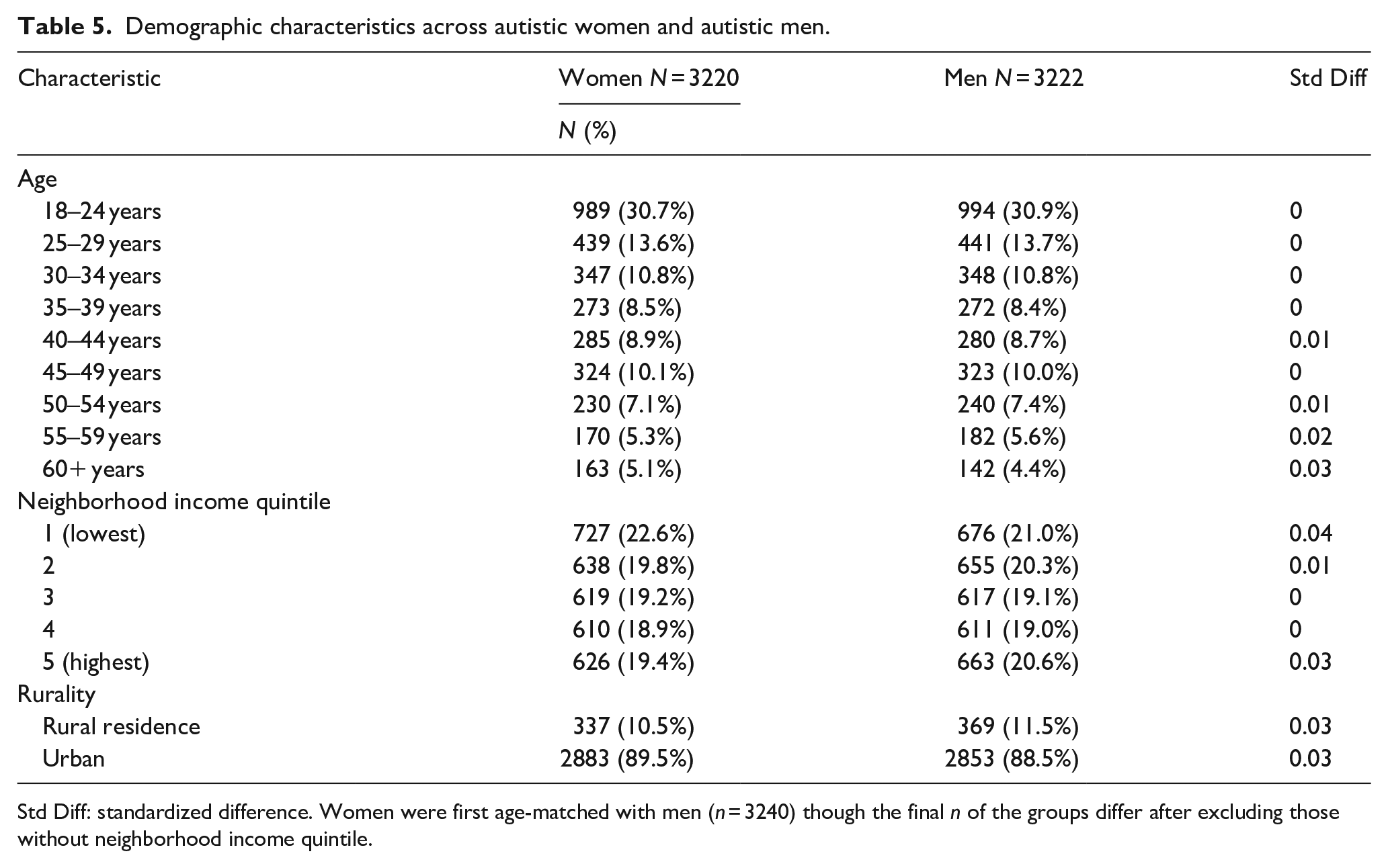
Std Diff: standardized difference. Women were first age-matched with men (n = 3240) though the final n of the groups differ after excluding those without neighborhood income quintile.
Health and service use characteristics between autistic women and men.
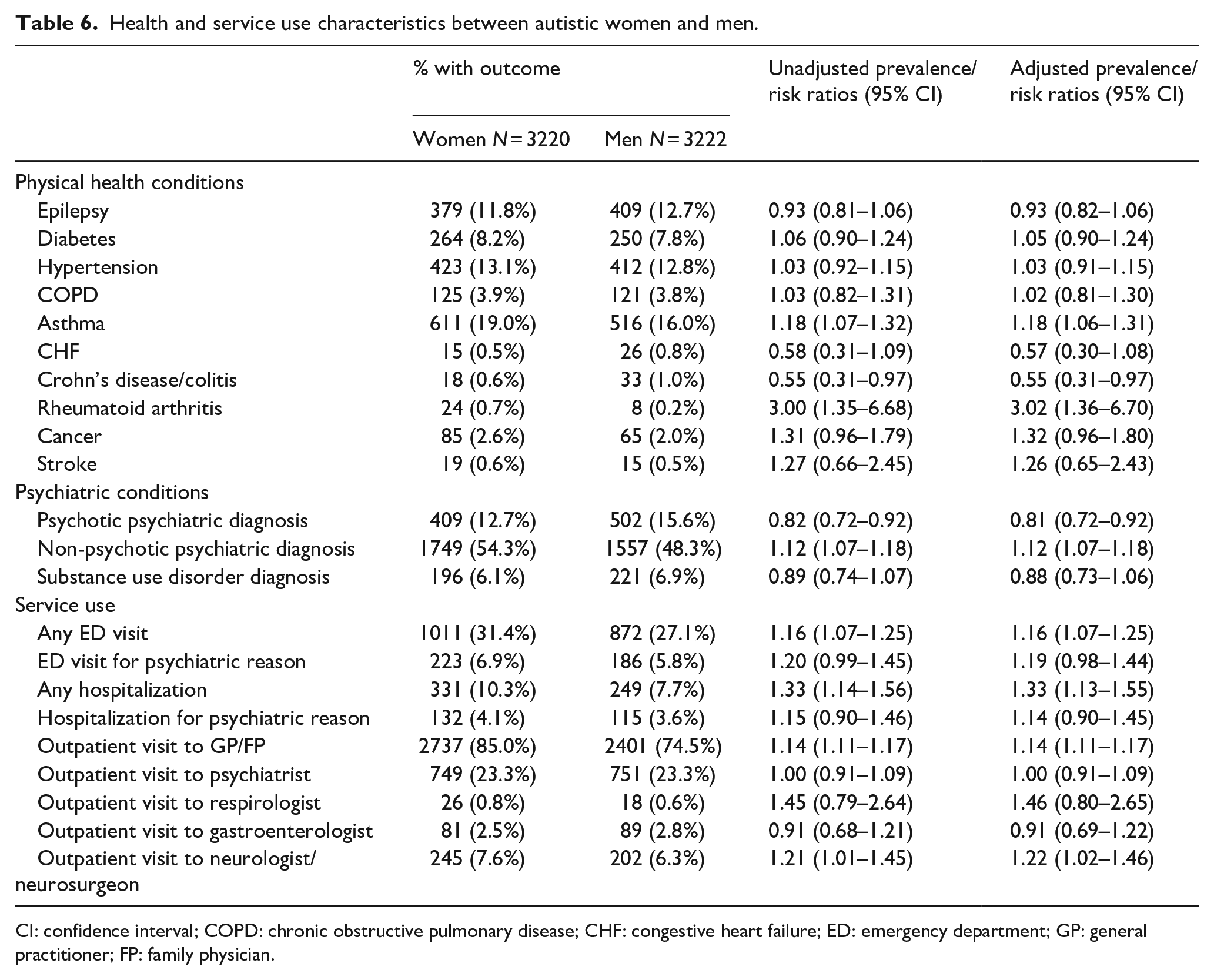
CI: confidence interval; COPD: chronic obstructive pulmonary disease; CHF: congestive heart failure; ED: emergency department; GP: general practitioner; FP: family physician.
Autistic women were less likely to have psychotic conditions (aRR = 0.81, 95% CI = 0.72–0.92). However, autistic women were more likely to have non-psychotic psychiatric conditions compared to autistic men (aRR = 1.12, 95% CI = 1.07–1.18). The prevalence of substance use disorders did not significantly differ between the sexes (Table 6).
Compared to autistic men, autistic women were more likely to visit the ED for any reason (aRR = 1.16, 95% CI = 1.07–1.25), to be hospitalized for any reason (aRR = 1.33, 95% CI = 1.13–1.55), and to visit a family doctor (aRR = 1.14, 95% CI = 1.11–1.17) and neurologist (aRR = 1.22, 95% CI = 1.02–1.46). Psychiatric ED visits and hospitalizations did not significantly differ between the sexes (Table 6).
Discussion
The present study fills current knowledge gaps as the findings are derived from a large, population-based sample of autistic women and men matched by age with adults with other DD and those without DD. Echoing a growing number of administrative data studies from other jurisdictions (Cawthorpe, 2017; Croen et al., 2015; Davignon et al., 2018; Hand et al., 2019; Smith DaWalt et al., 2021; Tint et al., 2021), we found that autistic women and men were more likely to have a wide variety of physical and mental health conditions and to use health services more compared to women and men without DD. There were some significant sex differences for specific physical (i.e. Crohn’s disease/colitis, rheumatoid arthritis) and psychiatric conditions (i.e. psychotic disorders, non-psychotic disorders) among age-matched autistic women and men. Rates of co-occurring health conditions were similar or lower among autistic women and men compared to women and men with other DD, except for higher prevalence of psychiatric conditions in the autistic groups. Health service use among autistic adults was generally similar to or greater than that of adults with other DD, with markedly increased psychiatric service use evident among autistic adults. There were some sex differences in health care use between autistic women and men (i.e. ED visit for any reason, hospitalization for any reason, visit to a family doctor and neurologist).
While we evaluated a wider age range than Weiss et al.’s (2018) study of young autistic adults, we found consistent results in that autistic adults had similar or fewer physical health conditions than age-matched adults with other DD. This discrepancy may be related to some of the underlying causes of intellectual disability (e.g. Down syndrome) among adults with other DD, which are commonly associated with physical health complications. Regardless of these differences, the high prevalence of co-occurring health conditions among autistic adults and those with other DD speaks to the importance of broad medical training of health care professionals regarding the complex health care needs of individuals with DD, including autism, across the lifespan (Adirim et al., 2021; Havercamp et al., 2021). Focused efforts on DD informed chronic disease management, continuity of care, and coordinated mental and physical care are areas of particular importance to improve health outcomes.
Our findings highlight significant disparities in the mental health of autistic adults compared to adults without DD and those with other DD, adding to the growing literature that indicates psychiatric conditions are significantly more common in autistic individuals of all ages (Lai et al., 2019). Interestingly, while autistic women and men alike had high prevalence rates of psychiatric conditions, there were differences in patterns of conditions in an age-matched sample of women and men. Autistic men had higher prevalence of psychotic conditions compared to autistic women, and autistic women had higher prevalence of non-psychotic psychiatric conditions compared to autistic men. Similar patterns of sex differences are seen in the general population (Boyd et al., 2015; Green & Pope, 1999; Rhodes et al., 2002; Seedat et al., 2009; Wittchen et al., 2011). Of particular concern is the high prevalence of psychotic disorders among autistic women and men alike in the present study. There is evidence to suggest both an overlap in clinical presentation and a significant degree of co-occurrence between autism and psychotic disorders (De Giorgi et al., 2019; Fitzgerald, 2012; Lai et al., 2019), which creates substantial challenges in psychiatric assessments (Kildahl et al., 2017; Van Schalkwyk et al., 2015). Further work in this area is needed given the complex ascertainment and pharmacological and psychosocial treatment challenges among autistic people (Downs et al., 2017; Lai et al., 2020).
Both autistic women and men in the current study had higher rates of substance use compared to women and men without DD. In population-based studies in Sweden and Norway (Butwicka et al., 2017; Solberg et al., 2019), autistic adults were twice as likely to have substance use problems than non-autistic adults and increased risks were found in non-autistic family members, which may suggest that environmental or genetic factors are at play. Qualitative results have also suggested that autistic adults are more likely to report using substances to manage behavior and/or mental health difficulties (Weir et al., 2021) than non-autistic adults, which is particularly problematic given the high rates of co-occurring psychiatric conditions among autistic adults. When compared to women and men with other DD, autistic women in the current study were no more likely to be diagnosed with substance use disorder though autistic men were less likely to be diagnosed with substance use disorders. Similarly, in Weiss et al.’s (2018) younger and predominantly male-based sample, autistic adults were less likely to be diagnosed with substance use disorders compared to adults with other DD. Similar to a recent U.S.-based study (Roux et al., 2022), patterns of substance use did not differ among our age-matched sample of autistic women and men. In the general population, men are more likely to have substance use disorders than women (McHugh et al., 2018), while mixed patterns have been found in previous samples of autistic women and men (Croen et al., 2015; Roux et al., 2022; Solberg et al., 2019; Weir et al., 2021). Overall, research on substance use among autistic adults is limited and recent research has shown concerningly low rates of substance use education among autistic girls and boys alike (Graham Holmes et al., 2022). It will be important to continue to consider sex/gender differences while studying patterns of substance use, education, and treatment planning.
Aligned with previous research (Hand et al., 2018; Vohra et al., 2016; Zerbo et al., 2019), we found that autistic adults had increased use of most health services compared to adults without DD. In addition, despite lower rates of many physical health conditions compared to adults with other DD, autistic adults largely had similar or increased use of health services compared to adults with other DD. High use of outpatient services and hospitalizations may reflect autistic adults’ difficulties accessing effective care due to service navigation concerns, challenges with sensory differences, and/or patient-provider communication problems (Mason et al., 2019; Walsh et al., 2020). Alternatively, it may be representative of appropriate service use among autistic adults and reflective of the significant challenges adults with other DD experience accessing health care. Reduced ED use among autistic adults compared to adults with other DD in the current study corroborates previous findings (Hand et al., 2018; Weiss et al., 2018) and may be indicative of a higher threshold for going to the ED, given how stressful that environment can be for autistic adults. Educational supports for clinicians providing care for autistic people in the hospital environment (Carter et al., 2017) as well as ways to assist autistic adults prepare for primary care and acute care procedures (Nicolaidis et al., 2016; Venkat et al., 2016) may be helpful; further work to this effect across a range of health care providers and settings may help autistic adults to receive effective care, and ultimately reduce high hospitalization rates.
Autistic women in the current study were less likely to use OB/GYN services compared to women without DD. Past population-based research has shown similar decreased rates of OB/GYN use among autistic women compared to the general population (Ames et al., 2021; Zerbo et al., 2019). While no significant difference in OB/GYN service rates between autistic women and women with other DD were noted in the current study, Ames et al. (2021) found lower rates of OB/GYN service among young autistic women (ages 14–25 years old) compared to young women with other special healthcare needs (i.e. attention-deficit/hyperactivity disorder and diabetes mellitus). However, among women with disabilities, women with DD, including autistic women, have been shown to encounter pronounced barriers to accessing health care (Tarasoff et al., 2020) which are likely attributable to compound experiences of marginalization (e.g. stigma, social determinants of health; Khan et al., 2021).
We found that autistic women and men demonstrated elevated use of outpatient psychiatric visits and psychiatric hospitalizations compared to women and men without DD and those with other DD. This finding aligns with their increased rates of psychiatric conditions. The same service use pattern has been seen in young autistic adults (Weiss et al., 2018) as well as autistic adolescents and children (Croen et al., 2006; Leslie & Martin, 2007; Mandell et al., 2006). Intensive outpatient services have been shown to reduce psychiatric hospitalizations for adults with a range of psychiatric conditions (Andrews & Sunderland, 2009; Preston & Fazio, 2000; Scott et al., 2009) and among autistic children with co-occurring psychiatric concerns (Mandell et al., 2012). In addition to autistic adults in the current study demonstrating high use of outpatient psychiatrist visits, the rates of psychiatric hospitalizations were high as well. It is important to better understand the effectiveness of current psychiatric care and how the interplay of other psychosocial supports and environmental adjustment (e.g. employment and residential supports) may reduce psychiatric hospitalizations.
Contrary to previous studies (Smith DaWalt et al., 2021; Tint et al., 2017), psychiatric service use did not differ among autistic women and men in the current study. However, autistic women were more likely to visit the ED for any reason, to be hospitalized for any reason, and to visit a family doctor compared to autistic men. Recently, Smith DaWalt et al. (2021) suggested that autistic women may experience “double jeopardy” with respect to multiplicative risk (e.g. above what would be expected based on autism diagnosis or sex alone) of service use. Concerns related to late autism diagnoses (Bargiela et al., 2016), increased rates of victimization (Brown-Lavoie et al., 2014), a greater burden of caregiving responsibilities (Offer & Schneider, 2011), gender-based compensation inequities (Chapman & Benis, 2017), differences in living arrangements and community participation (Song et al., 2022), and service providers’ disbelief of their health concerns (Tint & Weiss, 2018) may all play a role in precipitating and/or perpetuating autistic women’s increased risk of service use.
Limitations
There are important limitations to note when interpreting our results. Similar to previous administrative data studies, we were only able to identify the sex assigned at birth as designated within health records (and not based on karyotyping) and we were unable to analyze data by gender owing to a lack of data. Furthermore, binary sex as recorded in Ontario health records does not capture individuals who identify as transgender or nonbinary, which is recognized to occur more frequently among autistic individuals (Dewinter et al., 2017). Similarly, information concerning race and ethnicity is not collected in Ontario health records. These remain important areas for future research and further learning from the lived experiences of racially diverse and nonmale autistic individuals about their health care needs is needed.
Although our cohorts were created by merging health and disability support information (an advantage over using health data alone), we recognize that our data do not completely capture the autistic or DD population, and that information from other sources, such as educational or other clinical records, may contribute cases not identified by administrative data and/or mitigate potential misclassification errors (Bickford et al., 2020; Lin et al., 2014). This is a concern of particular importance for autistic women as they are known to be underdiagnosed (Loomes et al., 2017) and may have been misidentified if they did not have a health care encounter associated with a relevant diagnostic code or receive disability support. It is noteworthy that outpatient billing in Ontario only allows for a single diagnostic code per healthcare visit. As such, observable differences between groups may be related to factors not measured in this study. For example, we were not able to reliably stratify results of autistic adults based on the presence or absence of an intellectual disability, which has been shown to impact health and service use outcomes (Bishop-Fitzpatrick & Rubenstein, 2019; Hand et al., 2018). In addition, our data are based on diagnostic information prior to 2010 and include different look back periods for different outcomes. This lends itself to concerns with respect to potential missing data and variability in data quality. Moreover, as an increasing number of autistic women are being identified in adulthood (Lai & Baron-Cohen, 2015), it will be important for future research to study autistic women’s profiles based on more current data sources. We also acknowledge that a limited set of health conditions were included in the current study due to availability of validated algorithms and it will be important for future research to include other co-occurring conditions commonly associated with autism (e.g. obesity, sleep difficulties). We cannot comment on the frequency or quality of care received in any of the groups studied. We also did not study care received outside of formal medical services (e.g. social or educational supports), and it remains unknown how the current patterns of results would vary within other health care delivery models (e.g. privatized health care systems).
Conclusion
This study provides a comprehensive, sex-stratified characterization of the co-occurring physical and psychiatric conditions and associated service use in a large population-based sample of autistic adults. Overall, autistic women and men alike have high health care needs, as do adults with other DD. Further mental health support is especially critical for autistic adults and research examining sex and gender effects will assist in tailoring health promotion and intervention efforts. Future service planning will benefit from a combination of autism-specific as well as comprehensive DD-informed health care strategies.
Supplemental Material
sj-docx-1-aut-10.1177_13623613221144353 – Supplemental material for Health conditions and service use of autistic women and men: A retrospective population-based case–control study
Supplemental material, sj-docx-1-aut-10.1177_13623613221144353 for Health conditions and service use of autistic women and men: A retrospective population-based case–control study by Ami Tint, Hannah Chung, Meng-Chuan Lai, Robert Balogh, Elizabeth Lin, Anna Durbin and Yona Lunsky in Autism
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of the Health Care Access Research and Developmental Disabilities Program (![]() ). This study received funding from the Canadian Institutes of Health Research (CIHR) Partnerships for Health Systems Improvement Grant (PHE 103973) and a CIHR postdoctoral fellowship award. This study was also supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). Parts of this material are based on data and information compiled and provided by MOH and MLTC, and the Ontario Ministry of Children, Community and Social Services (MCCSS). This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from ©Canada Post Corporation and Statistics Canada. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources. No endorsement is intended or should be inferred. Parts of this material are based on data and/or information compiled and provided by CIHI. However, the analyses, conclusions, opinions, and statements expressed in the material are those of the authors, and not necessarily those of CIHI.
). This study received funding from the Canadian Institutes of Health Research (CIHR) Partnerships for Health Systems Improvement Grant (PHE 103973) and a CIHR postdoctoral fellowship award. This study was also supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). Parts of this material are based on data and information compiled and provided by MOH and MLTC, and the Ontario Ministry of Children, Community and Social Services (MCCSS). This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from ©Canada Post Corporation and Statistics Canada. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources. No endorsement is intended or should be inferred. Parts of this material are based on data and/or information compiled and provided by CIHI. However, the analyses, conclusions, opinions, and statements expressed in the material are those of the authors, and not necessarily those of CIHI.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.