
Abstract
Introduction
Clinical leadership is an essential skill for physicians, empowering them to lead and coordinate teams, communicate clearly under various conditions, model positive behaviors, display emotional intelligence, and ultimately improve patient care outcomes. However, there are currently no standardized residency curricula or competency-based assessments for clinical leadership, as residents often assimilate leadership skills through trial-and-error or observation of their clinical faculty. By utilizing a comprehensive needs assessment and synthesizing evidence-based practices, we developed and implemented a longitudinal and skills-based clinical leadership curriculum for pediatric residents.
Methods
We modeled our clinical leadership curriculum after Kern's 6-step approach to curricular development and the Accreditation Council for Graduate Medical Education competency requirements for professionalism. We identified topics based on a resident needs assessment and synthesized evidence from published practices. The curriculum was implemented through both monthly facilitated group sessions and independent learning modules.
Results
44 postgraduate year-2 (PGY-2) and PGY-3 pediatric residents participated in at least one monthly session of the clinical leadership curriculum. 27 (61%) completed the survey to evaluate the efficacy of the curriculum. Of the respondents, 23 (85%) residents found the leadership sessions useful, 4 (15%) were neutral, and none (0%) rated the sessions as not useful. 26 (96%) residents reported that the sessions should be continued.
Conclusion
The clinical leadership curriculum has been received favorably by senior pediatric residents at our institution. Our next steps are to pilot the curriculum within residency programs of different specialties at our own institution as well as with pediatric residencies at other institutions.
Keywords
Introduction
Clinical leadership encompasses essential skills for physicians. It is broadly defined as the ability to lead and coordinate teams, communicate effectively in various settings, role model positive behaviors, and exhibit emotional intelligence.1,2 This skill is associated with high quality, cost-effective patient care, 3 patient safety and outcomes, 3–7 physician engagement, wellbeing, and resilience.4,8 The need for clinical leadership training has been established,7,9,10 however there are no standardized residency curricula or competency-based assessments for clinical leadership skills.7–10 Residents report learning these critical skills through trial-and-error or observation of faculty. 9 Recently graduated physicians feel inadequately prepared to assume basic clinical leadership responsibilities.7,11 Clinical leadership training in graduate medical education is critical to ensure that future physicians have the necessary skills to successfully navigate in a dynamic healthcare environment. 7
We previously performed a comprehensive needs assessment with the pediatric residents at our institution to better understand their leadership training needs. 12 Our findings are consistent with, and build upon, previously published quantitative11,13 and qualitative14–16 leadership training needs assessments. Some residency programs have conducted leadership workshops but have faced challenges evaluating their efficacy without fully assessing learners needs beforehand or following up with learner progress.8,17–19 In addition, most programs are focused on improving knowledge on leadership topics rather than building and reinforcing practical, applied skills.14,20–24
Our objective was to develop a comprehensive, longitudinal, and skills-based clinical leadership curriculum based on our needs assessment 12 and evidence-based practices for senior trainees within graduate medical education.
Methods
The project was approved by the Eastern Virginia Medical School Institutional Review Board (IRB# 16-09-NH-0174). We used Kern's Six Step Approach to Curriculum Development as our conceptual framework, which has been summarized in Table 1.25,26
Application of Kern's 6 steps to curricular development.

Step 1 and Step 2
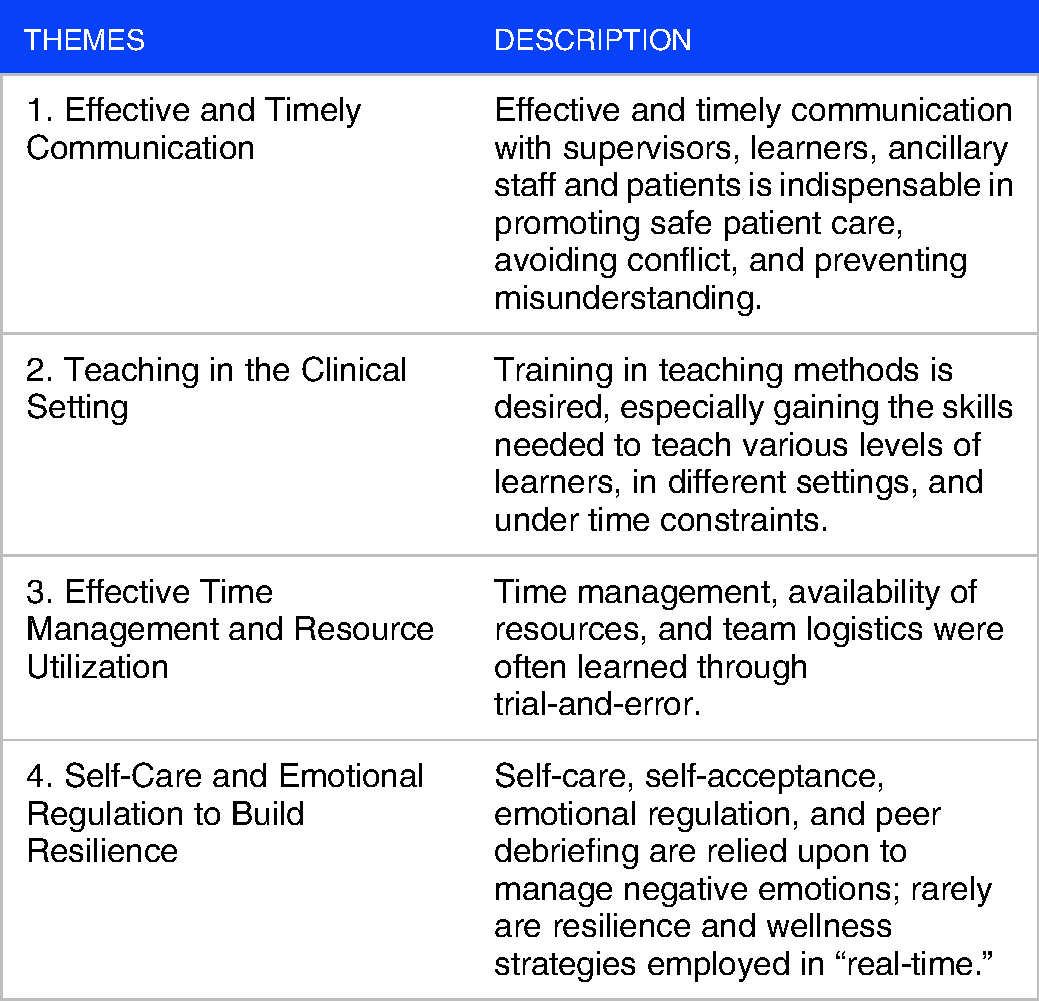
During academic years 2016 to 2018, we conducted the problem identification and general needs assessment (ie Step 1) and targeted needs assessment (ie Step 2). The results are summarized in Table 2.
Themes identified from a general needs assessment. 12
Step 3: Curriculum Goals and Objectives
Based on the results from the needs assessment, we developed goals and objectives for the clinical leadership curriculum and aligned them with competencies established by the Accreditation Council for Graduate Medical Education (ACGME), which has been summarized in Table 3. 27
Goals, objectives, and alignment to ACGME Competencies. 27

Step 4: Educational Strategies
Based on our goals and objectives, we searched PubMED and MedEdPORTAL for articles and curricula from 1990 to present with the following terms: “Professionalism,” “leadership curriculum,” “clinical leadership,” “leadership development,” “leadership training,” “professional development,” “resident leadership,” “setting expectations,” “feedback,” “time management,” “reframing thoughts,” “resident as teacher,” “team development,” “team building,” “emotional regulation,” “resiliency,” “conflict resolution,” “limitations,” “professional identity,” and “self-reflection” in order to identify evidence-based strategies for each respective topic. Our research team, consisting of a medical student, director of graduate medical education, and several faculty members with professional interests in academic medicine, then reviewed the articles specifically for teachable skills or actions that had evidence to support their use and then reached consensus on which skills should be included for each topic.
We used two different but complementary formats to deliver the curriculum as group sessions and independent learning modules. First, we held facilitated group sessions to debrief teams, encourage open discussions, build community, foster resilience, and relieve stress. 28 This allowed participants to engage in open peer-to-peer discussions to share their personal experiences, ask questions, and discuss personal strategies. The faculty facilitator would introduce evidence-based strategies throughout the session where appropriate. As a second format, due to time and scheduling challenges in residency, we also developed interactive, self-paced learning modules on each topic.
Our target audience included pediatric residents who had completed at least one year of residency. As a yearly curriculum open to both postgraduate year 2 (PGY-2) and PGY-3 residents, we acknowledged that residents would attend similar sessions the following year. We believed that the open format would benefit the residents by reinforcing leadership skills with a different perspective after accruing more training experience. Additionally, we hoped that PGY-2 residents would ask questions and request help from PGY-3s, who could then assume a mentorship role.
Step 5: Implementation
We implemented the clinical leadership curriculum during the 2018 – 2019 academic year. Each monthly group session and independent learning module focused on one leadership topic:
Session #1: Introduction to Leadership and Setting Expectations (Appendix A) Session #2: Receiving Feedback (Appendix B) Session #3: Giving Feedback (Appendix C) Session #4: Time Management Skills (Appendix D) Session #5: Teaching Mixed Groups of Learners (Appendix E) Session #6: Reframing Thoughts (Appendix F) Session #7: Team Building (Appendix G) Session #8: Managing Emotions (Appendix H) Session #9: Conflict Resolution (Appendix I) Session #10: Overcoming Limitations (Appendix J) Session #11: Finding your Professional Identity (Appendix K) Session #12: Personal Reflection (Appendix L) and Passing the Torch
Recruiting Faculty Facilitators
At our program, our facilitator team included a Residency Associate Program Director and the Director of Graduate Medical Education. Both had academic interests in professional development. Both facilitators had training in focus group facilitation.
Planning the Group Sessions
We scheduled the sessions approximately 4 weeks apart and during protected time such as morning report, noon conference, or as part of an academic half-day.
Resident Recruitment
We invited all pediatric residents at our institution who had completed at least one year of training. We informed residents that attendance would be optional.
Room and Table Setup
We tracked attendance for the purpose of providing the anonymous evaluation survey (Appendix M) to those who participated at the end of the academic year.
Using the resident conference room, we arranged tables in a circle formation facing inward, allowing room for all residents to visualize every other participant. We allowed residents to select their own seats, but we asked them to move around if necessary to ensure a fair distribution of residents from each class and to allow for a diversity of perspectives.
Facilitating the Group Sessions
Ground Rules: 1 Minute
The faculty facilitators set expectations for confidentiality with the residents at the beginning of each session to create a psychologically safe space for open discussion. These ground rules have been effective in that no one has breached this confidentiality agreement, to our knowledge, over the last four years since the program has started. The faculty facilitators also provided their contact information (email and cell phone) to all participants and emphasized that they were available for questions or follow-up.
Introduction of Topic: 5 Minutes
Following these ground rules, the facilitators then took five minutes to introduce the topic of discussion and then shared a personal experience or challenge related to the topic to initiate discussion. By doing so, the facilitators established an environment of trust and psychological safety by sharing an example related to the specific clinical leadership topic in which they themselves learned to grow professionally from the experience. 29
Peer-to-Peer Discussion: 35 to 40 Minutes
The faculty facilitated the discussion, interjecting only to pose another question if there was an extended period of silence or if directly addressed to clarify or answer questions. We have provided examples of broad questions to ask for each respective topic within each respective module (Appendices A-L) in the section “Before You Begin: Questions to Consider.” Additionally, the facilitators introduced evidence-based strategies where applicable during discussion. (eg: “That's excellent –That technique is actually called ‘reframing’ and the evidence….”). Given the sensitive nature of several leadership topics, residents were encouraged, but not required, to participate. To encourage participation, the faculty facilitators first broadly asked the most senior group of residents (eg PGY-3s in a mixed group of PGY-2s and PGY-3s) to lead the discussion by sharing their experiences of what has been effective or ineffective throughout their training. Occasionally, they opened it up to PGY-2s to ask questions or air concerns and give PGY–3s a chance to share their processes or techniques.
Debrief: 10 to 15 Minutes
Following the peer-to-peer discussion, the faculty facilitators summarized key points from the discussion, identified and compiled personal solutions from participants, and then reviewed evidence-based strategies with the entire group. To close each session, the faculty facilitators invited residents to complete the associated interactive, self-paced module (Appendices A-L).
Implementation Guide for Independent Learning Modules
We designed clinical leadership modules (Appendices A-L) to be completed independently as an adjunct to group sessions for residents interested in deeper study or that were unable to attend an in-person session. All modules were available with a recommended order that matched the order of the group sessions. There was no suggested time limit or spacing, as we designed the modules for self-paced learning to accommodate individual schedules and professional obligations. We estimated that each module would require approximately 60 minutes to complete. The only material necessary to participate included a personal computer or tablet if independent learning modules were implemented electronically. No prerequisite knowledge or training was required to participate.
Step 6: Evaluation and Feedback
Distributing the Survey
At the end of each academic year, following the final group session, we distributed an evaluation survey to all residents who had participated in at least one session to provide anonymous feedback. We designed it to evaluate resident perception and satisfaction with the group session.
Incorporating Survey Feedback
We reviewed the survey responses annually for two years and made iterative updates to the curriculum. We have since updated the survey to reflect a 5-point Likert scale and to include additional items that evaluate the efficacy of individual sessions and modules related to specific leadership topics (Appendix M).
Results
We implemented the clinical leadership curriculum during the 2018-2019 academic year. 44 (100%) PGY-2 and PGY-3 pediatric residents participated in at least one group session, with an average attendance of 5 sessions attended per resident. At the end of the academic year in June 2019, 27 (61%) completed the anonymous survey that evaluated resident perception and satisfaction. The June 2019 survey did not quantify the efficacy of individual sessions and the curriculum overall, but the survey has since been updated to include a 5-point Likert scale and such items (Appendix M). From the June 2019 survey, 23 (85%) residents found the leadership sessions useful, 4 (15%) were neutral, and none (0%) rated the sessions as not useful. 26 (96%) residents reported that the sessions should be continued. Additionally, the open-ended survey responses indicated an overall favorable perception of the group sessions and formalized clinical leadership curriculum.
Conclusion
The benefits of clinical leadership skills for physicians3,4,6 and others within the medical system 3,5,7,8 are well described in the literature. The need for a clinical leadership curriculum for medical trainees has also been defined,7,11 and the needs assessment at our own institution 12 matches the breadth and the depth of the content deemed essential across other specialties and institutions.9,11,13 We developed and implemented a longitudinal, skills based clinical leadership curriculum that utilizes evidence-based strategies targeting interpersonal communication, professional relationships, time management, resource utilization, and emotional resilience for senior pediatric residents. The curriculum directly addresses the professionalism requirements outlined by the ACGME by providing explicit instruction on clinical leadership topics to foster resident resilience and cultivate an open culture that is conducive to professional development. 27 The results from the anonymous evaluation survey indicate an overwhelmingly positive reception to the curriculum.
The initial curriculum addresses the needs and content deficits described in the literature but still face a number of limitations. First, because the sessions were optional, there may be self-selection bias reflected in our surveys, if residents who value professional development were more likely to attend and respond favorably. However, given that 100% of residents attended one or more sessions, it is likely that this self-selection bias is minimal. Additionally, our original survey did not evaluate the efficacy of individual sessions or modules. The survey has since been updated to include such items rated on a 5-point Likert scale (Appendix M). We have also included survey items to address utilization of skills in the clinical environment. Ideally, we would measure the impact of the curriculum on patient care outcomes, but such a metric may be difficult to measure and associate directly with the implementation of this educational intervention. Although our findings are consistent with the literature across different specialties and institutions, we acknowledge that this curriculum was developed based on a needs assessment within the specialty of pediatrics and at our institution.
Next steps include piloting the curriculum within residency programs of different specialties at our own institution as well as with pediatric residencies at other institutions. Given the identified need for this type of training in the literature at all levels of education,1,10 the curriculum could be modified to fit the needs of trainees in other specialties or at earlier stages of training, such as interns or medical students. Additionally, placing the curriculum on a web-based platform may allow for greater access, increase our ability to measure its favorability and impact, and help develop connection and community. This longitudinal and skills-based clinical leadership curriculum may serve as a model or template for future work and collaborations.
Supplemental Material
sj-docx-1-mde-10.1177_23821205221096354 - Supplemental material for Implementation of a Clinical Leadership Curriculum for Pediatric Residents
Supplemental material, sj-docx-1-mde-10.1177_23821205221096354 for Implementation of a Clinical Leadership Curriculum for Pediatric Residents by Daniel H. Mai, Heather Newton, Peter R. Farrell, Paul Mullan and Rupa Kapoor in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205221096354 - Supplemental material for Implementation of a Clinical Leadership Curriculum for Pediatric Residents
Supplemental material, sj-docx-2-mde-10.1177_23821205221096354 for Implementation of a Clinical Leadership Curriculum for Pediatric Residents by Daniel H. Mai, Heather Newton, Peter R. Farrell, Paul Mullan and Rupa Kapoor in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205221096354 - Supplemental material for Implementation of a Clinical Leadership Curriculum for Pediatric Residents
Supplemental material, sj-docx-3-mde-10.1177_23821205221096354 for Implementation of a Clinical Leadership Curriculum for Pediatric Residents by Daniel H. Mai, Heather Newton, Peter R. Farrell, Paul Mullan and Rupa Kapoor in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-4-mde-10.1177_23821205221096354 - Supplemental material for Implementation of a Clinical Leadership Curriculum for Pediatric Residents
Supplemental material, sj-docx-4-mde-10.1177_23821205221096354 for Implementation of a Clinical Leadership Curriculum for Pediatric Residents by Daniel H. Mai, Heather Newton, Peter R. Farrell, Paul Mullan and Rupa Kapoor in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-5-mde-10.1177_23821205221096354 - Supplemental material for Implementation of a Clinical Leadership Curriculum for Pediatric Residents
Supplemental material, sj-docx-5-mde-10.1177_23821205221096354 for Implementation of a Clinical Leadership Curriculum for Pediatric Residents by Daniel H. Mai, Heather Newton, Peter R. Farrell, Paul Mullan and Rupa Kapoor in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-6-mde-10.1177_23821205221096354 - Supplemental material for Implementation of a Clinical Leadership Curriculum for Pediatric Residents
Supplemental material, sj-docx-6-mde-10.1177_23821205221096354 for Implementation of a Clinical Leadership Curriculum for Pediatric Residents by Daniel H. Mai, Heather Newton, Peter R. Farrell, Paul Mullan and Rupa Kapoor in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-7-mde-10.1177_23821205221096354 - Supplemental material for Implementation of a Clinical Leadership Curriculum for Pediatric Residents
Supplemental material, sj-docx-7-mde-10.1177_23821205221096354 for Implementation of a Clinical Leadership Curriculum for Pediatric Residents by Daniel H. Mai, Heather Newton, Peter R. Farrell, Paul Mullan and Rupa Kapoor in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-8-mde-10.1177_23821205221096354 - Supplemental material for Implementation of a Clinical Leadership Curriculum for Pediatric Residents
Supplemental material, sj-docx-8-mde-10.1177_23821205221096354 for Implementation of a Clinical Leadership Curriculum for Pediatric Residents by Daniel H. Mai, Heather Newton, Peter R. Farrell, Paul Mullan and Rupa Kapoor in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-9-mde-10.1177_23821205221096354 - Supplemental material for Implementation of a Clinical Leadership Curriculum for Pediatric Residents
Supplemental material, sj-docx-9-mde-10.1177_23821205221096354 for Implementation of a Clinical Leadership Curriculum for Pediatric Residents by Daniel H. Mai, Heather Newton, Peter R. Farrell, Paul Mullan and Rupa Kapoor in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-10-mde-10.1177_23821205221096354 - Supplemental material for Implementation of a Clinical Leadership Curriculum for Pediatric Residents
Supplemental material, sj-docx-10-mde-10.1177_23821205221096354 for Implementation of a Clinical Leadership Curriculum for Pediatric Residents by Daniel H. Mai, Heather Newton, Peter R. Farrell, Paul Mullan and Rupa Kapoor in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-11-mde-10.1177_23821205221096354 - Supplemental material for Implementation of a Clinical Leadership Curriculum for Pediatric Residents
Supplemental material, sj-docx-11-mde-10.1177_23821205221096354 for Implementation of a Clinical Leadership Curriculum for Pediatric Residents by Daniel H. Mai, Heather Newton, Peter R. Farrell, Paul Mullan and Rupa Kapoor in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-12-mde-10.1177_23821205221096354 - Supplemental material for Implementation of a Clinical Leadership Curriculum for Pediatric Residents
Supplemental material, sj-docx-12-mde-10.1177_23821205221096354 for Implementation of a Clinical Leadership Curriculum for Pediatric Residents by Daniel H. Mai, Heather Newton, Peter R. Farrell, Paul Mullan and Rupa Kapoor in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-13-mde-10.1177_23821205221096354 - Supplemental material for Implementation of a Clinical Leadership Curriculum for Pediatric Residents
Supplemental material, sj-docx-13-mde-10.1177_23821205221096354 for Implementation of a Clinical Leadership Curriculum for Pediatric Residents by Daniel H. Mai, Heather Newton, Peter R. Farrell, Paul Mullan and Rupa Kapoor in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
We thank Dana Ramirez, MD, former Program Director of the CHKD/EVMS Pediatrics Residency Program, for assistance with recognizing and protecting the time to study clinical leadership and implement the curriculum within the residency structure, and Clarence W. Gowen, MD, Department Chair of Pediatrics at CHKD/EVMS for assistance with his vision for physician leadership and support in the development of clinical leadership training for residents.
Author Contributions
RK, HN, PF, and PM designed the study and implementation plan. PF, RK, HN facilitated the sessions. DM, RK, and HN complied and edited all appendices. RK and DM analyzed survey responses. All authors reviewed and discussed the results and contributed to the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.