
Abstract
Introduction:
Although clinical leadership in physicians is associated with improved healthcare, leadership training is rarely integrated into residency training. Our objective was to perform a comprehensive needs assessment of our pediatric residents’ existing leadership experiences and knowledge and to identify training gaps within our program.
Methods:
First, we held focus groups with senior pediatric residents to understand their clinical leadership experiences and identify training needs. Notes were transcribed and independently coded by 2 researchers, with thematic saturation achieved. Next, we focused each session on 1 leadership content area identified from the aforementioned themes to better understand the specific training needs for each topic.
Results:
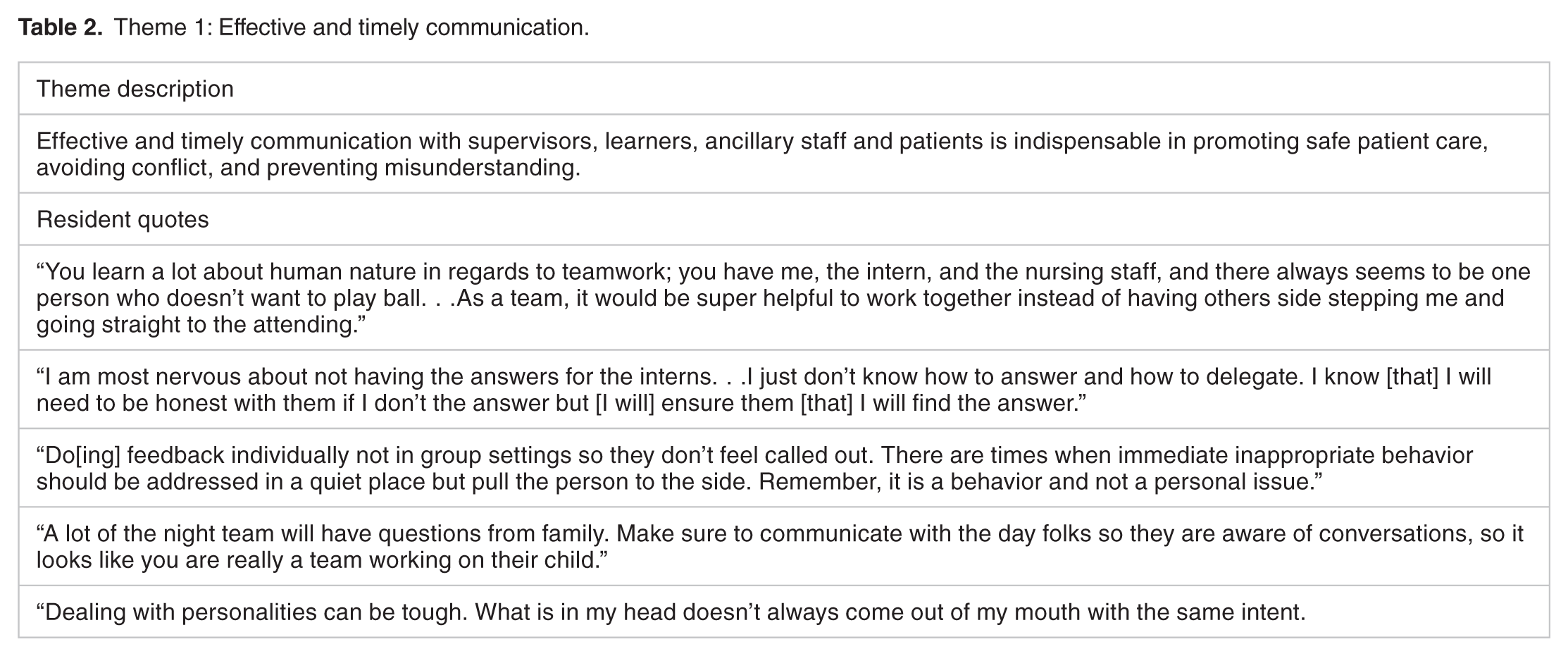
Four major themes were identified: (1) Effective and timely communication with supervisors, learners, ancillary staff, and patients is indispensable in promoting safe patient care, avoiding conflict, and preventing misunderstanding. (2) Training in teaching methods is desired, especially gaining the skills needed to teach various levels of learners, in different settings and under time constraints. (3) Time management, availability of resources, and team logistics were often learned through trial-and-error. (4) Self-care, self-acceptance, emotional regulation, and peer debriefing are relied upon to manage negative emotions; rarely are resilience and wellness strategies employed in “real-time.”
Conclusion:
Senior residents currently face gaps in clinical leadership training and may benefit from additional instruction in content areas related to these 4 themes. Our next steps are to utilize the identified themes to develop a longitudinal and skills-based clinical leadership curriculum to address the gap in graduate medical education.
Keywords
Introduction
Clinical leadership, broadly defined as the ability to effectively lead and coordinate teams, communicate clearly in various settings, role model positive behaviors, and display emotional intelligence, is considered an essential skill for physicians. 1 On an individual level, physicians who demonstrate clinical leadership can collaborate effectively in team-based settings and minimize miscommunication to deliver high quality, cost-effective care to patients. 2 On a systems level, clinical leadership increases physician engagement and results in advances in healthcare reform, regulation, and patient safety policies. 3 Although there is literature that suggests that clinical leadership empowers physicians and improves patient care,2-6 the process by which clinical leadership is learned is less clear, as there have been no standardized residency curricula or competency-based assessments for leadership development in physicians.6-9 While physicians invest the majority of time during their residency to the acquisition and application of clinical knowledge, their exposure to leadership training is generally lacking; they primarily report learning these critical skills through trial-and-error or observation of faculty in higher positions of power. 10 As a result, recently graduated physicians report feeling inadequately prepared to assume basic leadership responsibilities, such as leading multidisciplinary teams and resolving professional conflicts.6,11 Furthermore, physicians who lack leadership training are more prone to burnout and depression, which impacts quality of care and patient safety as well as contributing to high physician turnover and a workforce shortage. 12 Effective clinical leadership training is critical in graduate medical education to ensure a holistic education that will provide the necessary skills that future generations of physicians need in the dynamic healthcare environment. 6
While the need for leadership training has been established,6,10,11 and there is ample evidence that it affects patient outcomes,2-6 as well as physician wellbeing and resilience, 12 robust needs assessments for the content of such a training are lacking. Several programs have attempted to survey leadership training needs, such as at a large Northeastern academic medical center, where respondents reported needs in “leading a team,” “confronting problem employees,” “coaching and developing others,” and “resolving interpersonal conflicts.”13,14 However, surveys may not be an optimal methodology in evaluating training needs as they provide standardized representations of groups as a whole, lack insight into individual needs, and may fail to identify needs that were not pre-conceived during the survey design process.15,16 Few programs have conducted focus groups to expand upon these leadership needs through in-depth discussions.17,18 Additionally, most programs are geared toward improving knowledge as opposed to developing practical, applied skills.17,19-23 Other programs have instituted brief leadership workshops to try and address leadership training needs,7,24,25 but find it difficult to evaluate the efficacy of their program without fully assessing training needs. 26
In order to develop a longitudinal and skills-based clinical leadership curriculum based on best practices both within and outside of medicine, 6 we performed a comprehensive needs assessment with the residents at our own institution through focus groups with in-depth peer-to-peer discussions.
Methods
We utilized the 21 Standards of Reporting Qualitative Research (Table 1) as our reporting guidelines. 27 We modeled our comprehensive needs assessment after Steps 1 and 2 of Kern’s 6 steps of curricular development, which include problem identification and general needs assessment, and targeted needs assessment, respectively. 28
Standards for reporting qualitative research (SRQR).

This accounts for the overlap of 22 residents transitioning into resident positions over a 2-year period.
After requests by residents and faculty members for additional training of residents in the “senior role,” we obtained approval from the local institution review board for an educational intervention (IRB#16-09-NH-0174) to perform a needs assessment for the purpose of developing a clinical leadership curriculum for residents.
Conducting focus groups was the optimal methodology because it allowed us to perform a comprehensive needs assessment to gather qualitative data on both the breadth and depth of training needs. 16 Asking open-ended questions allowed us to better understand residents’ thought processes and follow-up with responses, if necessary. 16 As social familiarity establishes a more comfortable environment to elicit honest answers, we sought to recruit a group facilitator that had been well received by the residents. 29 Furthermore, we considered alternative methods, such as a standardized survey, but opted instead to conduct focus groups, as it encouraged peer-to-peer discussion and allowed observations of participant behaviors to re-direct tangential conversation. Lastly, we hoped that interpersonal discussions between residents, sharing personal experiences, would trigger memories or examples from other residents to add value to the discussion.
Focus group team and preparation
We assembled a team including clinical faculty, a graduate medical education (GME) specialist, and chief residents. To ensure consistency, we designated 1 faculty member to facilitate every session and another to transcribe every session. At our program, the faculty facilitator was an attending physician with focus group facilitation training and experience. Each resident had previously worked with the physician during their emergency medicine rotation, so the participants and the facilitator were familiar with each other. The faculty facilitator and the transcriber also had previous training in focus group coding and qualitative research. We created and used a script (Figure 1) that was reviewed by chief residents, faculty, and an expert in focus groups for use by the faculty facilitator during the sessions. During each focus group, the transcriber used a laptop to transcribe resident responses electronically.

Focus group script.
Participants and setting
Participants in the focus groups included post-graduate year-2 (PGY-2) and PGY-3 pediatric residents who assumed a “senior role” in the residency program. We excluded interns because we were interested in the unique challenges of “leading from the middle,” where senior residents lead junior learners, such as interns and medical students, but still report upwards to an attending physician. 30 No other prerequisite knowledge or training was required of participants. This study was conducted at an urban, stand-alone children’s hospital with a medium-sized three-year pediatric residency program that has approximately 22 residents per year. Of note, there are no subspecialty fellows outside of the Emergency Department.
Focus group design and implementation
From August 2016 to May 2017, senior pediatric residents at CHKD/EVMS participated in monthly focus groups to better understand their clinical leadership training needs. We informed residents that participation was voluntary, that all responses would be transcribed but not associated with identifying information, that their participation in the focus group implied consent, and that the information would be used to better understand resident training needs in clinical leadership.
The focus groups took place in the morning conference room with tables arranged in a circle formation facing inward to allow each participant to visualize each other. Upon entering the room, residents could select their own seats, but were asked to move where possible to ensure a fair distribution of residents. Each focus group had a convenience sample of available residents, usually consisting of 8 to 12 participants, but no more than 15.
Each month, residents participated in peer-to-peer discussion during 1-hour focus groups with open-ended questions from the prepared script related to their challenges in a senior role, experiences related to witnessing unprofessional behavior, and “what they wished they had known prior to starting as a senior.” At the end of each focus group, the facilitator summarized the key points of discussion and invited clarifying comments. By the end of the academic year, we had conducted a total of 9 focus group sessions as we had achieved thematic saturation from the resident responses. We did not conduct a focus group during December due to resident obligations during the holiday schedule.
Thematic analysis
Resident responses were directly transcribed. The faculty facilitator and the transcriber performed content analysis by independently coding the transcriptions from each session using an iterative coding process to identify patterns of responses, ensure reliability, and examine discrepancies. 31 The faculty facilitator and the transcriber kept rigorous memos of coding decisions to ensure consistency in coding. The codes were then categorized, and emerging themes were identified. Both coders then met to achieve consensus and resolve discrepancies. Thematic saturation was achieved and used as a basis for a targeted assessment.
Targeted needs assessment
In the second year of the program, from August 2017 to May 2018, we conducted monthly facilitated discussions with the succeeding group of PGY-2 and PGY-3 residents. We used the same format as previously described, but we focused each monthly session on 1 content area related to the themes that emerged from the qualitative analysis of the sessions from the prior year. The purpose of the 2017 to 2018 focus groups was to better understand resident experiences and training needs within each content area. The same prepared script was used and residents were asked to focus their responses and discussion on the selected content area (eg, feedback). Responses were again transcribed.
Results
During the initial 9 focus groups from 2016 to 2017, all 44 (100%) PGY-2 and PGY-3 residents participated in at least 1 focus group session. From 2017 to 2018, the succeeding group of 44 (100%) PGY-2 and PGY-3 residents participated in at least 1 focus group for the targeted needs assessment. A total of 66 senior pediatric residents participated in the focus groups, which accounts for the overlap of 22 residents who transitioned from a PGY-2 to a PGY-3 position over this 2-year period. Based on the resident responses that were transcribed and coded, we identified 4 major themes (Tables 2–5):
Theme 1: Effective and timely communication.
Theme 2: Teaching in the clinical setting.

Theme 3: Effective time management and resource utilization.

Theme 4: Self-care and emotional regulation to build resilience.

Lack of effective communication is currently a barrier to optimal patient care and is prevalent when interacting with colleagues, attending physicians, medical students, ancillary staff members, and even patients themselves. Miscommunication may consequently contribute to frustration and negative emotions that compound dissatisfaction with their training and the program. To minimize miscommunication, medical trainees would benefit strongly from instruction on how to resolve conflicts and avoid misunderstanding in a professional manner.
Although PGY-2 and PGY-3 residents assume more teaching responsibilities, they currently lack training in teaching methods, especially with learners at different levels of education, in various clinical settings, and under time-limited circumstances. Formalized instruction on how to set expectations, provide feedback, and delegate roles would establish a foundation to facilitate learning and assume teaching roles.
In addition, residents struggle to develop efficient techniques in time management and resource utilization, which are currently learned through trial-and-error. A lack of dedicated instruction may compound the high stress environment of residency training, as residents practice unhealthy behaviors, such as avoiding meals or having poor sleep hygiene. Identifying personalized solutions on how to prioritize tasks appropriately, for example, would be greatly appreciated.
Finally, many stressors within the clinical learning environment can contribute to the myriad of negative feelings experienced among residents, including anxiety, apprehension, and Imposter Syndrome. These feelings contribute to the prevalent rates of burnout and depression among residents. Therefore, instruction on strategies for self-care, self-acceptance, and emotional regulation may reduce burnout and depression and foster resilience.
Discussion
Here we presented the results of our assessment, which identified clinical leadership training needs in 4 major areas for senior pediatric residents at our institution. They would benefit from training in: (1) effective and timely communication, (2) teaching strategies in the clinical setting, (3) effective time management and resource utilization, and (4) self-care and emotional regulation techniques to build resilience.
The identified themes collectively align with the current literature on what is necessary for effective clinical leadership and would benefit resident trainees.1-7 Resident responses also indicate an overall desire for applied leadership skills training in the content areas covered by the 4 themes. Additionally, the high prevalence of depression and burnout within graduate medical education32-36 is often attributed to the “hidden curriculum,”37,38 which involves implicit standards of conduct that govern behaviors, beliefs, and attitudes that have been deemed inappropriate yet perpetuated.38-41 Clinical leadership skills training would address the hidden curriculum by explicitly redefining appropriate standards of conduct and actively engaging physicians, ultimately leading to improved clinical outcomes.2,3,42
Although we have successfully identified clinical leadership training needs, we understand that our focus groups face several limitations. The needs assessment was performed with pediatric residents, so they may not apply universally across other specialties; however, our findings align with those in the current literature, which are not exclusive to the field of pediatrics. In addition, the generalizability of the findings to other settings might be limited for several reasons. First, these needs were identified by residents at a single institution; however, the high level of resident participation and the variety of different clinical settings of our residency program (eg, outpatient clinic, emergency department, inpatient team, intensive care units, etc.) are likely similar to other institutions and implementation at other programs can assess for the consistency of these needs. Additionally, our institution is a tertiary care center without inpatient subspecialty fellows, where the senior resident is truly the learner that is leading the team. Although this may limit generalizability, it likely adds to the breadth and depth of the themes. Furthermore, we have employed qualitative methods to assess training needs, as opposed to more robust methods that utilize both qualitative and quantitative data, which may have been beneficial in comparing and stratifying the relevance of specific needs.
Ultimately, the responses from our comprehensive needs assessment indicate that residents currently face gaps in clinical leadership skills and would benefit from additional training. Our next steps are to utilize the identified themes to develop a longitudinal and skills-based clinical leadership curriculum to address the gap in graduate medical education. We further plan to evaluate the impact of the curriculum utilizing skills-based domains, in addition to focusing on resident behavior, resilience, and wellbeing. Our goal is to ultimately empower residents, reduce the prevalence of depression and burnout within graduate medical education, and improve patient care outcomes.
Footnotes
Acknowledgements
We thank Dana Ramirez, MD, former Program Director at CHKD/EVMS Pediatric Residency, for assistance with recognizing and protecting the time to study clinical leadership within the residency structure, and Clarence W. Gowen, MD, Department Chair of Pediatrics at CHKD/EVMS for assistance with his vision for physician leadership and support in the development of clinical leadership training for residents.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
HN, PF, PM, and RK designed the study and reviewed the script prior to conducting the focus groups. PF and RK facilitated the focus groups as HN transcribed resident responses. RK and HN analyzed responses for thematic coding. All authors reviewed and discussed the results and contributed to the final manuscript.