
Abstract
Surveys were sent to deans and curriculum leaders of American medical schools regarding the teaching of disclosure and apology in the curriculum. One-hundred six medical schools responded (n = 106; 60% response rate) and results showed that disclosure and apology (also known as communication and resolution programs or CANDOR) is being taught in American medical schools but more work remains to develop consistent curriculum across all medical schools. The same survey (with slightly different wording) was sent to a commercial list of fourth year medical students; two hundred thirty students (n = 230, 17% response rate) representing 67 medical schools completed the survey. The students’ data – though not statistically significant – provides a glimpse into students’ feeling about this topic, including the desire to learn what happens after “sorry” and how cases can be resolved with disclosure, including the insurance, legal, and compensation aspects. Further avenues of research on this topic are suggested.
Keywords
Introduction
The concept of sharing adverse medical events and medical errors with families has many names, from the long-time moniker “disclosure and apology” or simply “disclosure” to more recent marketing terms such as communication and resolution programs (CRP), CANDOR, and others. Nonetheless, disclosure/CRP is becoming more prevalent in American acute and long-term care healthcare organizations.1–4 Once controversial, disclosure/CRP is now ethically expected and promoted in healthcare, insurance, and legal circles. However, practicing physicians often quip or complain -- sometimes in writing5,6 – that medical schools typically do not teach how to communicate following adverse medical events, how to apologize to angry patients and families, and other forms of crisis communication along with the legal and insurance considerations. To foster greater understanding, acceptance, and practice of disclosure/CRP, some suggest this topic must be taught in medical schools7,8, including formal lecture material, simulations and other realistic training, coaching, and presentations and seminars with practicing physicians as well as attorneys, risk managers, and claims professionals. Indeed, learning how to have difficult conversations in general with consumers is an important skill set for medical students, but what specifically are American medical schools teaching about disclosure/CRP? Are schools including this topic in the curriculum, and, if so, how much is disclosure/CRP emphasized and how exactly are they teaching this content to tomorrow's physicians? There has been no measurement or survey about what is being taught about disclosure/CRP in American medical schools. 1 To learn what is being taught about disclosure/CRP in the medical school curriculum, this first-of-a-kind study surveyed deans and curriculum leaders of America's 178 medical schools (Medical Doctor & Doctor of Osteopathic Medicine) on this topic. A survey was also sent to a commercial list of fourth year American medical students.
Methods
A cross-sectional survey with an introductory page and 16 questions was developed, pilot tested among a dozen colleagues with medical, nursing, and risk management backgrounds, and approved by the Institutional Review Board (IRB) at The Ohio State University. The introductory page contained definitions for adverse event and medical error 9 and defined disclosure and apology “as a communication process with a patient and family following an unexpected outcome, typically starting with empathy (“sorry” and remorse but not accepting responsibility) and possibly followed by apology if a medical error is proven, with apology defined as accepting responsibility and expressing a desire to make amends, financial and otherwise.” Respondents were also instructed in the following manner: “Disclosure and apology is becoming the ethically preferred choice for addressing adverse events. However, disclosure is still controversial in some quarters. Moreover, not all medical schools have incorporated disclosure into their curriculum. There are no ‘right’ or ‘preferred’ answers to our survey questions. We only want your honest answers. You may always choose to refuse to answer a question but please be assured that your responses will be kept strictly confidential.” The survey was administered with the help of CHRR, or the Center for Human Resource Research, at The Ohio State University, with CHRR's in-house proprietary web survey software which is programmed with Java, Javascript, and html.
The questionnaire was constructed to mirror how disclosure and apology is typically discussed and taught to healthcare professionals, 1 beginning with a real case (names redacted) concerning a routine medical procedure that resulted in a tragic death. Deans/curriculum leaders were asked six questions to gauge if their students were taught how to handle such scenarios. The survey then asked five questions if and how disclosure and apology is incorporated in their curriculum. Responses were measured with a five-point Likert scale (strongly agree, agree, neither agree/disagree, disagree, strongly disagree). “Strongly agree” and “agree” were scored one (1) and two (2) respectfully and considered a “positive” response, while “Neither Agree/Disagree” was tabulated as a three (3) and considered a “neutral” response, and “Disagree” and “Strongly Disagree” were scored as a four (4) and a five (5) and considered a “negative” response. The survey continued with two open-ended narrative questions asking respondents to provide additional insights into how they address disclosure and apology and what they would like to see included (or added) to the curriculum at their school and nationally. The survey concluded with demographics questions.
The surveys for deans/curriculum leaders and medical students were basically identical except for changes in phrases for their intended audiences (“Does your medical school prepare students for…” vs. “Did your medical school prepare you for…”). The deans’ survey can be found in Appendix A.
The public websites of America's 178 medical schools (including 38 Osteopathic medical schools) were visited to obtain e-mail addresses and phone numbers for deans and curriculum leaders (all of which were publicly available on medical school websites). Between March 2020 and March 2021, surveys were sent via e-mail to the medical school deans and curriculum leaders and followed up with phone calls. One response was requested per school from the dean or any curriculum leader. There was no incentive given for completing the survey.
A commercial list of fourth year medical students with 1367 email addresses was rented (the company which owned list e-mailed the survey for a fee; the company-maintained control of the e-mail list). A five-dollar gift card was offered as an incentive for completion of the survey.
The patchwork of so-called “apology laws” in American states was not taken into consideration in the design of this experiment, as many disclosure experts and advocates agree apology laws can offer some encouragement with the development of disclosure programs but said laws are not necessary for successful administration of disclosure programs. 1
Analysis
Coded qualitative data was converted to themes by two researchers to create quantifiable information for the purposes of data analysis (via Nvivo) and inter-rater reliability. The narrative/open-ended questions were analyzed with a process involving a close reading of open ended and narrative native data and then manually coding text fragments into a framework of themes or topics. Text fragments may be comprised of several words (phrases) or complete sentences. They may also be coded to more than one theme if overlapping concepts are present. The textual data informs the shape and growth of the theme framework. The framework grows as more themes are added from the qualitative data.
Means and frequencies of data were also tabulated.
Results – Deans & Curriculum Leaders
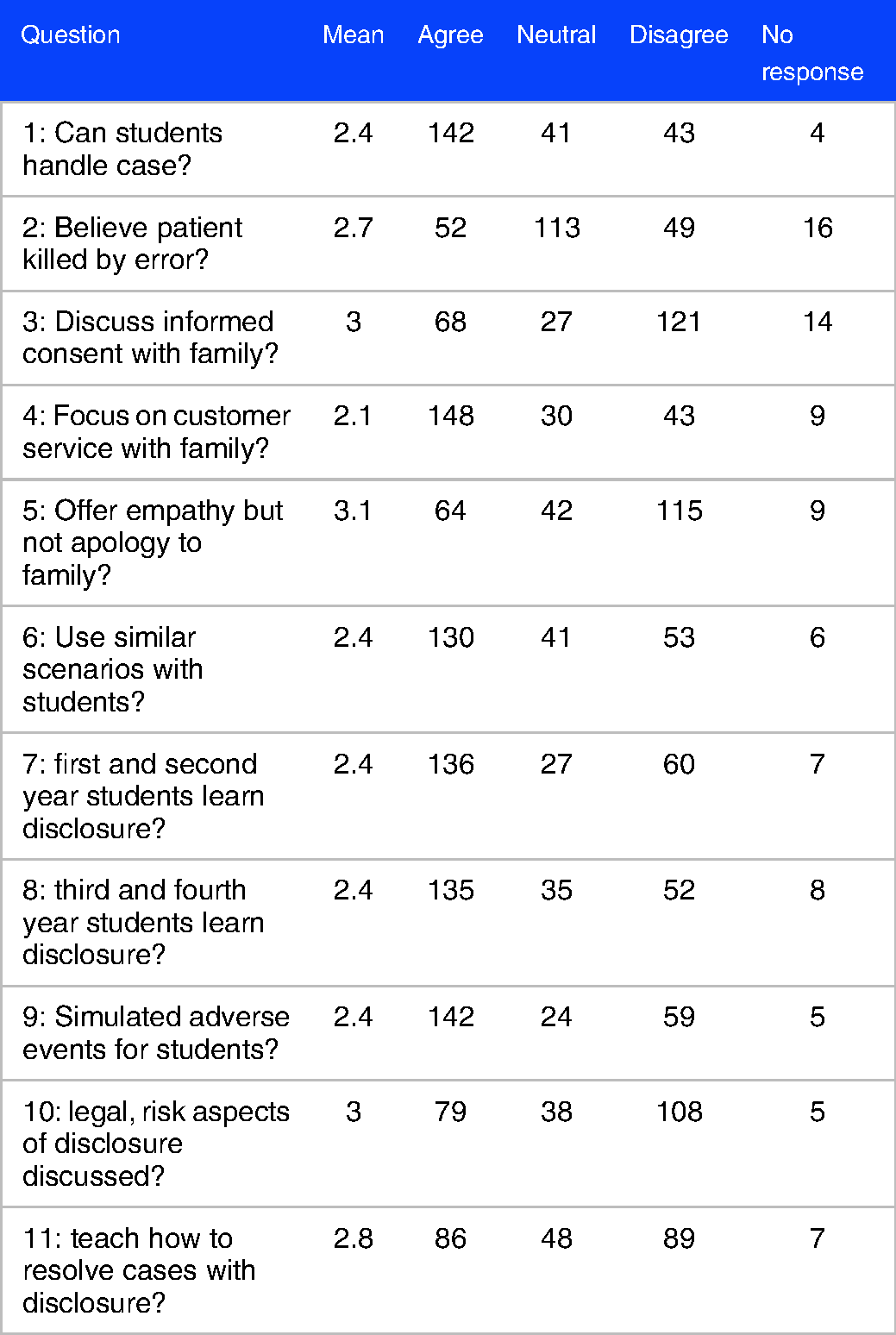
One hundred six (n = 106) American medical schools completed the survey (60% response rate). The results for questions 1-11 from the medical schools are shown in Table 1.
Responses from deans/curriculum leaders.

Ninety-six (n = 96) of the 106 schools provided responses to the narrative questions. For question 12 -- “Please provide any additional insights into how your school teaches young physicians how to discuss adverse events with patients/families, including strategies and stories/cases as well as challenges and hurdles.” --- there were a wide variety of responses. Answers ranged from “no organized, institutionally established approach” and “we lack the experience and curriculum for this at this time” to “it is extensively taught within our mandatory ethics and patient safety course” and “one of our most effective sessions we do is a panel discussion of our clinical faculty discussing their own errors, what they learned, and the experience of apology.” Fifty-four (n = 54) deans/curriculum leaders mentioned coursework --- including electives (such as an ethics and patient safety electives) (n = 7), group discussions (n = 6), case reviews and scenarios (n = 6) and lectures (n = 3) --- as the primary method for engaging students on this topic. Some leaders indicated that their respective schools offer medical malpractice sessions (n = 2), professors sharing personal experiences with students (n = 2), close readings (n = 2), and even a required international patient safety credential (n = 1). Deans also mentioned several types of formal training and interactions (n = 17); with simulations (n = 8) as the most common formal training followed by clerkships (n = 3), coaching (n = 1), skills workshops (n = 1) and SPIKES (Acronym for providing distressing information to patient and families. S stands for setting, P for perception, I for invitation or information, K for knowledge, E for empathy, and S for summarize or strategize) protocol (n = 1).
There were 39 other responses, including seven deans (n = 7) stating students shouldn't be involved in disclosure discussions while four deans (n = 4) explicitly supported increasing awareness and education for their students around this topic. Ten deans (n = 10) said they offer no content on this topic, while two deans (n = 2) expressed they have content in development.
Question 13 asked deans and curriculum leaders the following question: “What would you like to see included in the medical school curriculum (both at your school and nationally) to help future physicians be better equipped to discuss adverse medical events with patients and families?” At the local level (within individual schools) deans and curriculum recommended improving students’ knowledge about adverse events and disclosure (n = 53), skills (n = 25) and publicly available curriculum (n = 1). Simulation was the most frequent mention (n = 21) to increase knowledge of disclosure with discussion coming in second (n = 12). Some deans would like to see more faculty sharing real life stories with students (n = 9).
At the national level, deans and curriculum leaders would like to see more information and awareness around this topic (n = 39), more practice (n = 9), and more assessment (n = 5).
Results – fourth Year Medical Students
Two hundred thirty students (n = 230, 17% response rate) representing 67 medical schools completed the survey; data from students is tabulated and reported in Table 2. The results from the students are not being statistically compared to the deans due to the low response rate from students.
Responses from fourth year medical students.
One hundred eight students (n = 108) provided narrative responses to questions 12 and 13. For question 12, some comments included, “We have not addressed this in our medical school curriculum, but I think it would be useful” and “We had one online module about medical errors but that was it” to “I have never received any formal training on what happens legally after an apology” and “Had good training about how to deliver bad news including the power of apology. Would have been nice to have had some more insight about the legal ramifications of these events.”
Many students commented that some aspects of delivering bad news to patients/families were covered in their curriculum but also indicated there was no deeper explanation how to resolve medical errors, legally or otherwise. In fact, twenty-one students (n = 21) stated they received little to no instruction regarding what happens after “sorry,” including legal and insurance aspects and potential compensation for medical errors. In the positive, students said schools provided formal coursework (n = 39), simulation (n = 28), and information on apologies (n = 27). In the negative, students shared that their schools provided little to no information on the topic of disclosure and apology (n = 62).
For question 13, students stated they would like schools to provide simulations (n = 72), more information on the topic (n = 56), curriculum additions or changes (n = 44), and more training (n = 21). Under more information on the topic, students indicated they wanted to learn the consequences of medical error (n = 41) and legal and financial aspects (n = 34). Eight students (n = 8) stated they did not learn about disclosure and apology through formal curriculum but instead through observations or mentorships during clinical rotations.
Discussion/Conclusion
The process by which medical schools train future physicians is constantly evolving10,11 and professionals associations such as the American Medical Associations are soliciting new ideas for improving medical school curriculum. 12 Disclosure & apology, or CRP or CANDOR, is an idea that has become the ethically expected response to adverse medical events, including medical errors. Future physicians are well-served by learning how to disclose adverse events and medical errors to patients and families, and medical schools can provide this needed training by incorporating appropriate content in their curriculum. This survey provided an initial glimpse into what is being taught about disclosure in America's medical schools (the literature shows no similar studies), and like all newer ideas the study showed that the adoption of disclosure and apology concepts in the medical school curriculum is a work in process. Many schools have been begun to adopt and teach this concept in earnest, yet much more work remains. Moreover, this research project suggests some current gaps as well as avenues for future research.
Many deans and curriculum leaders shared that disclosure principles are taught throughout their medical school curriculum, including use of scenarios similar to the case posed in the survey. Moreover, deans and curriculum leaders strongly believe that students would know to focus on customer service elements following an adverse event. However, more than half of the deans and curriculum leaders were less sure if students could handle the case presented in the survey. The rest of the answers in the survey were mixed or somewhat neutral which likely indicates unease or uncertainty about this topic. Moreover, narrative responses to question 13 – “What would you like to see in the medical school curriculum” – indicated more enhancements are needed in the curriculum, including improving students’ knowledge about disclosure along with skills through simulation and discussion. In fact, some schools indicated they have done little to nothing on this topic. Indeed, the teaching of disclosure and apology in American medical schools is a work in progress.
Student data cannot be leaned on strongly given the low response rate (17%). The survey was conducted with a commercial list in which the company-maintained control (they sent e-mails) and there was no ability to make follow up phone calls to encourage completion of the survey. Nonetheless, the data from the students representing 67 different American medical schools provides an initial view into how fourth year medical students feel they have been prepared on the topic of disclosure and apology. Like the deans, students generally believe that disclosure principles are being taught to some degree in the medical school curriculum. Moreover, students indicated a strong tendency to focus on customer service in the aftermath of an adverse event and expressed confidence (even if naïve confidence) in handling the hypothetical case in the beginning of the survey. However, students expressed concern that the legal, insurance, and compensation aspects of disclosure are not being adequately covered by American medical schools. In their narrative responses, students gave the impression disclosure is not covered in an adequate or complete fashion, if at all in some medical schools. Students expressed a desire to know how cases play out beyond “sorry” or empathy, including how the legal and insurance issues are handled and how patients can be compensated for legitimate medical errors. Ultimately, although statistically based comparisons cannot concerns the deans and student data sets, possible trends can be gleamed that suggest some disparity between the perceptions of students and deans exists on this topic. Did deans paint a rosier picture due to social desirability bias while students provided a truer picture? These issues and questions are fodder for future research on this topic.
Study Limitations
This study did not dive deeply into the specifics of how disclosure is taught in American medical schools, most especially those schools that do a good or excellent job covering this topic. Furthermore, this study was not designed to explore conceptual frameworks or pedagogy strategies 13 but future projects could certainly venture down this path. The profiles of curriculum leaders as far as gender, race, age, etc was not accounted for and may be a subject for future study. Also, the high prevalence of neutral responses to survey questions potentially indicated a central tendency bias.
Further research is needed to adequately assess the opinions and perspective of medical students on this topic, including responses of medical students by profile (gender, race, age, etc). Moreover, schools that indicated strong curriculum on this topic should be studied further, and, perhaps “a national curriculum endorsed by the AMA and AAMC” can be developed as suggested by one dean responding to the narrative questions. Finally, future studies should also measure the acquisition of competencies from disclosure and apology curriculum.
Footnotes
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Appendix A: Survey Format
Scenario: “Mrs. Woods is a 53-year-old woman who visits the hospital for a CT-guided biopsy of her liver. Mrs. Woods believes the test shouldn't be a big deal because the staff told her the test is routine, so she tells her husband to go to the mall across the street and do some shopping. The technician assures Mr Woods she will call him when the test is complete.
Mr Woods is standing in the mall when his cell phone rings. He answers to hear a nurse frantically screaming, “Come quickly!”
When Mr Woods gets to the hospital, he learns his wife is dead.”
D1. How much do you agree or disagree with the following statements: Your medical students have been adequately prepared by your curriculum to lead the discussion with Mr Woods. D2. Your students would believe that Mrs. Woods had been killed by medical errors D3. Your students would start the conversation with Mr Woods by reviewing informed consent D4. Your students would focus on customer service elements in the conversation with Mr Woods, including phone calls, finding clergy or social work, food, transportation, grief support, etc. D5. Your students would know the fact pattern presented in the case would only initially warrant empathy and a promise to review the care and stay connected with the family – but not apology. D6. Your medical school curriculum teaches similar-type scenarios to your students involving disclosure & apology. D7. What follows are broad questions about your curriculum and disclosure & apology. How much do you agree or disagree with the following: Disclosure and apology concepts are incorporated into your first and second year courses. D8. Disclosure and apology concepts are incorporated into the clinical rotations of third and fourth year medical students in your program. D9. Your medical school provides to your students simulated patient experiences that include adverse medical events. D10. Your curriculum fully discusses the legal, insurance, business, and public relations aspects of disclosure & apology? D11. Your medical school teaches student how cases can be handled through to resolution (including cases of medical error where monetary compensation is justified) with disclosure and apology. D12. Please provide any additional insights into how your school teaches young physicians how to discuss adverse medical events with patients/families, including strategies and stories/cases as well as challenges and hurdles. D13. What would you like to see included in the medical school curriculum (both at your school and nationally) to help future physicians be better equipped to discuss adverse medical events with patients and families? At my school: Nationally: D14 What is your gender? D15 Are you Hispanic or Latino origin? D16 What is your race?