
Abstract
Background:
Medical schools are required to have formal advising structures; however, there are limited data on how to optimally meet that mandate. Learning communities (LC), with their emphasis on longitudinal relationships, offer a unique scaffold for advising.
Program description:
The Johns Hopkins School of Medicine (JHSOM) LC focuses on curricular and extracurricular longitudinal connections between students and advisors. A core component of the LC is a relationship-centered advising (RCA) model drawing from best practices in physician–patient relationships, life coaching, and social contract theories. The key elements of the model include dyadic and small group advising, while the LC structure allows for faculty development in these domains. Relationship-centered advising approaches the collaborative advising work between students and advisors through explicit valuing of personal experiences, mutual respect, and earned trust. Framing the advising relationship in this way allows it to grow with the student along their medical school journey.
Program evaluation & results:
Student and faculty satisfaction with this model is high. Data from annual, anonymous student evaluations consistently indicate high degree of trust in and satisfaction from these relationships.
Discussion:
Relationship-centered advising aims to create a relationally anchored platform on which students can develop their personal and professional identities. This LC-based advising model is adaptable across schools regardless of structure and resources.
Background
Medical student advising has long focused on career advising: finding a mentor, choosing electives, exploring specialty choice, and ultimately achieving success in the match. Many 4-year, US medical schools have used Offices of Medical Student Affairs for such advising tasks supplemented with specialty advisors once students differentiate. There has been a growing awareness of and literature about the prevalence of both burn-out and depression among medical students,1–3 and in response, a new emphasis has been placed on student wellness initiatives providing support to students across a wide range of situations and needs. A growing trend in US medical schools has been to pair students with a longitudinal advisor who follows them throughout their undergraduate medical training.
Medical schools’ advisors serve many diverse roles including but not limited to coaching around study skills, issues of professionalism and mistreatment, and student wellness including managing relationships, health issues, and screening and referral for mental health concerns. This broader concept of advising requires trained and interested faculty willing and able to deliver these expanded skills as well as protected time to do this more nuanced and complex job well. Some specific advising content has been developed by the AAMC Careers in Medicine. There are not, however, best practices for how to develop or deliver this kind of broad, humanistic, and developmentally sensitive advising. The authors propose that learning communities (LCs) provide an ideal foundation on which one might build such advising programs.
Learning communities share common values and strive to actively learn together and from each other. McMillan and Chavis cite 4 essential elements: (1) a sense of membership and belonging, (2) the belief that one can impact the group, (3) the ability to have individual needs fulfilled by the group, and (4) the opportunity to share events and sustain connections over time. Becoming a physician requires a shift in how students view themselves in the context of their new role. 4 Professional identity formation is a dynamic process leading to student expression of altruism and service to others across preclinical, clinical, and research settings. That shift occurs through a transformational learning process that includes critical reflection about one’s own beliefs and biases, followed by a consideration of alternative perspectives and priorities, leading to a reframing of those beliefs. This iterative model of learning and change occurs best in settings where trust, autonomy, relational engagement, role modeling, and active dialog are supported. Learning communities offer an excellent mechanism through which faculty can explicitly support and guide students through this learning process. This report shares the JHUSOM model of relationship-centered advising (RCA) as an example of using LC principles to directly impact student experience through advising.
Program Description
The Johns Hopkins University School of Medicine Colleges Advisory Program (JHUSOM CAP) utilizes dedicated faculty working with students one-on-one as well as in small groups throughout the medical school experience to support personal and professional growth, create a sense of belonging and connection, and foster feelings of safety and self-efficacy. The individual relationships that are built between students and their JHUSOM CAP advisor parallel the model of relationship-centered care commonly discussed for clinical services: (1) each member of the student–advisor dyad is a unique person with a narrative that contributes to the connection; (2) the relationship is considered a partnership, each member of which deserves respect; (3) the way in which a student can best be understood and advised requires thoughtful personalization of both the content and process of advising; and (4) each person in the dyad gains a sense of trust and connection that allows the value of the relationship to grow. 5
The JHUSOM CAP has 24 faculty members chosen through a competitive application process by faculty and students with an eye to familiarity with the medical school curriculum, a student-centered orientation, and diversity of person and practice. Each faculty member is supported at 20% effort to teach the clinical skills course in year 1 and provide longitudinal advising across all years of the curriculum. These faculties are organized into 4 groups or “Colleges” of 6, and the 120 students/year are similarly divided into 4 groups of 30. Those 6 faculty members then work with 5 students each year for the duration of the student’s time at the medical school. This creates a “molecule” in each cohort year, and stacking those molecules creates a “macromolecule” for each faculty member.
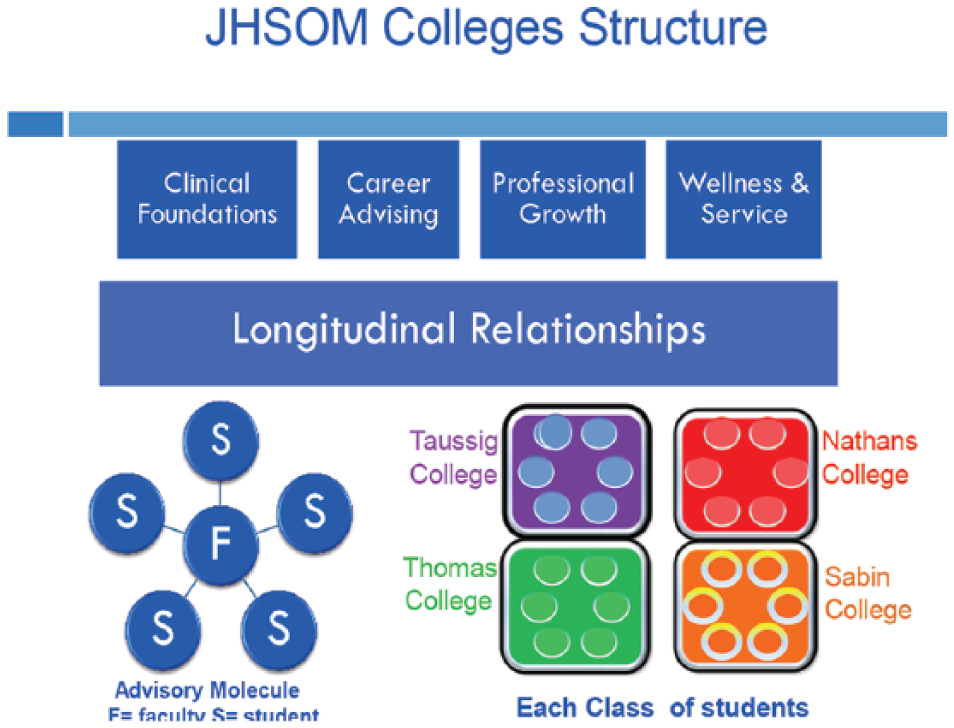
Longitudinal relationships serve as a platform for learning across various domains in medical school.
An advising contract is reviewed at the beginning of medical school that establishes clear expectations of communication, goals of the advising relationship, and confidentiality of discussed information. For many students, this is their first experience with such an intentional establishment of parameters of an advising relationship. Advising takes 2 primary forms: (1) individual advising meetings with a minimum of 3 meetings per year but often exceeding that based on an individual student’s needs and (2) mandatory group meetings that are embedded in the formal curriculum 4 times/year. In addition, college faculty connect with students through social events, extracurricular events, and community service. Colleges Advisory Program also sponsors a range of school activities to support students such as Choosing your Schedule, How to Prepare for Step 1, How to Apply to Residency, Mock Interview Night, and many others.
Colleges Advisory Program faculty meet with their advisee groups approximately every 3-4 months to facilitate reflective dialog aimed at making sense of various experiences in medical school and the impact that they have on individual students, teams, and patients. These sessions create intentional safe spaces for discussing those common experiences that define the student evolution into becoming a professional. The sessions target (1) transitions, eg, into medical school, onto the wards, and out into residency; (2) issues of identity formation and professionalism including understanding their role and managing tensions between their role and personal values; (3) debriefing of critical incidents on the clerkships; and (4) navigating the impact of clinical work, professional identity, and role acceptance on self concepts and practice of wellness and self-care. Explicit, facilitated dialogs can help normalize common developmental experiences embedded in this transformation, identify struggling students, and create moments for increased support, reflection, and guidance. These sessions are often powerful moments for students and are important pedagogical spaces in which faculty value, model, and support transformational learning across the 4 years of the curriculum with a consistency in the relationship. The LC structure offers a consistency of connection that can deepen over time as the relationships between students and with faculty are valued and trust grows.
Our model of relationship-centered advising is proactive and dynamic, moving with students along their paths through medical school. Colleges Advisory Program faculty are aware of the student curricular experience and check in with advisees around critical transitions. One-on-one advising encompasses a longitudinal dialog around academic topics such as effective studying and board preparation, as well as research, career counseling, personal wellness, and extracurricular opportunities. Students embrace the safety of the relationship and commonly bring traditional (eg timing of step exams, selection of electives) and nontraditional content (eg navigating family stress, mental health concerns) to the meetings. Each advising encounter employs a relationship-centered approach guiding the student to introspection and self-awareness using a developmentally sensitive framework. Each meeting typically results in a set of “next steps” and anticipatory guidance until the next advising encounter.
In addition to the individual student–faculty relationships that are formed, the stacked cohort structure of this advising model allows students to connect and journey together through the many ups and downs of life in medical school. The safe and confidential nature of the small group advising sessions not only allows for sharing of experiences—highs as well as lows—but also the opportunity to co-create wisdom about how to navigate medical school. This creates a vertical connection through which advice and support can flow.
Program Feedback
Each year, the students are asked to complete an anonymous survey asking a wide range of questions about their experiences with CAP. The questions include items on (1) frequency of formal and informal meetings; (2) relational connectedness including trust, safety, and overall value; (3) guidance around professional identity formation; (4) guidance around personal wellbeing; (5) guidance on academic success through discussions of study habits, performance progress, and preparation for next steps such as boards; (6) support around career planning and residency application process; and (7) the impact of the advisor–advisee relationship on other connections in medical school. All questions have a 5-point Likert-type response scale ranging from Strongly Agree to Strongly Disagree. In addition, there is a separate section that asks for comments about what the student appreciated most about their advisor, if they were not connecting well what barriers they faced, and what suggestions they have for the program as a whole.
Response rate for the survey is usually around 65% to 70%. The most recent collated data from 2016 to 2017 indicate high student satisfaction in the relational connectedness domain as evidenced by almost 75% of students rating the overall value to them of the advising relationship as “outstanding,” which is the highest possible score; 87% of students stated that their advisor is “is non-judgmental,” and 90% of students reported that their advisor “listens well.”
Faculty are required to track every individual and face-to-face meeting with their advisees in an excel spread sheet and submit these data to the CAP leadership every 6 months. This not only ensures that every student is being seen regularly but also gives an overview of CAP’s involvement with students. Although each faculty has 5 students per year of medical school, with students taking time off for PhD, MPH, research, and other opportunities, the average number of advisees/faculty is 25. In 2016-2017, the total number of 1:1 meetings between students and advisors was more than 2200 with an average of 3.8 meetings per student (expected minimum is 3 per year). The curricular-embedded small group sessions meet 4 times a year and students and faculty have contact through social and extracurricular programming at least 4 times a year as well. Taken together, there are thus typically at least a dozen points of contact throughout the year with each student.
The institution has been very receptive to and supportive of this program. The CAP budget represents 10% of the available monies for educational planning in the overall SOM budget. In addition, CAP leadership has been invited to sit on various student-focused committees in the medical school such as promotions and clerkship director meetings.
Discussion
Our 15-year experience at JHUSOM has demonstrated that developing a RCA model within a US medical school LC is both feasible and appears to be well received by students, faculty, the institution, and regulatory bodies alike. The CAP program is now so closely interwoven with the overall student experience that it is virtually inseparable from the curriculum and culture of the medical school. In addition, the importance of the dyadic relationship between student and advisor is well recognized beyond its confines. Faculty external to CAP but critical in the lives of students such as Deans of Curriculum and of Student Affairs work closely with the program with a growing appreciation for the student experience. This enhanced and expanded communication has in turn permeated the larger community on campus.
The LC structure enables students and faculty to be explicitly connected in a relational system purposefully focused on students’ professional development. In addition, it allows faculty advisors to form relationships with each other across a wide range of specialties while similarly facilitating student bonds within and across molecules. These connections are in turn embedded in a culture that promotes interdependence. Thus, just as the relationship-centered care model explicitly values connections and reciprocal influences, so does the RCA model.
Our experience with this model of advising has shown benefits to students, faculty, and the institution as a whole. Prior to this model, students felt that advising ranged from inconsistent to absent, with graduation feedback including comments such as “no one really knows who I am here.” With the implementation of this advising model within our LC, we see very different types of feedback. There is a deep sense of connection reflected not only in the percentage of students rating the program highly as noted above, but also in the anonymous comments, eg:
My advisor is always very interested in how I am progressing as a student and how I am doing as a person. He gives excellent advice that is geared toward helping me in school and in preparing myself to be a competitive applicant for residencies. He is also a great person to talk to about non-school topics.
XX is always there when I need her, and checks in throughout the year to see how I’m doing. She addresses any and all concerns or uncertainties that I have. She is a great listener and gives appropriate advice and reassurance. She has helped me think about the next steps in getting where I want to, in regards to residency and personal life goals.
Absolutely outstanding listener who consistently asks me important questions that no one else asks.
Faculty also value this model of advising, welcoming not only these strong connections with students but also cherishing the faculty LC. For many faculty whose primary role is as a clinician-educator, it can be challenging to find peers with similar priorities in clinical or research-focused departments. Often, university or hospital departments have just 1 or 2 faculty whose primary focus is education. This model of a medical school LC, however, brings together faculty from disparate departments and specialties who share a dedication to relationally framed, student-centered education and advising. That sense of belonging creates high job satisfaction. Colleges Advisory Program faculty participate in an annual review with CAP leadership, and a consistent theme that emerges in those meetings is that CAP is the highlight of their professional work. In addition, these new faculty connections lead to sharing research interests, educational scholarly work, and mentoring. In addition, results of the annual AAMC Graduation Questionnaire, known as the “GQ,” have improved notably in areas of advising. Colleges Advisory Program faculty have offloaded work from the Office of Medical Student Affairs and have created a method of early detection for student health and academic needs.
During the 15-year experience with this program, there have been challenges. Recruitment of the most talented faculty has been very successful, but with such a group, promotion to other leadership positions has been a common event. The faculty development needs for these positions are great and onboarding new faculty is labor and time intensive. The program strives for diversity in its faculty in all domains with a hope to mirror the student body. At times this is difficult to accomplish. As the institution has received the program so favorably, it is not uncommon for any new initiative or idea to quickly become something that CAP faculty might take on. This can create tension between CAP’s primary advising mission and other possible innovations. At times, CAP has had to pass up opportunities that have not been directly aligned with our primary goals.
In summary, while many students and faculty have historically developed strong partnerships, creating an inclusive model that ensures that all students have access to the same advising opportunities requires a background structure to ensure viability. Program success requires broad institutional and departmental support including faculty salary support. Consideration should be given to recruiting those faculty with knowledge of the student experience and the curriculum, who have strong relationship-centered skills, and who reflect the diversity of the student body. Advising activities should be intentionally embedded within the curriculum with attention paid to the overall curricular map, student transitions, and known areas of student distress. Such an undertaking requires a formal leadership structure to sustain and ensure faculty development as well as ongoing student satisfaction. Learning communities offer an ideal model for longitudinal, relationally focused advising that can support students’ development and learning throughout their medical school career and beyond.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
EF conceptualized, reviewed literature, wrote, and edited this paper. MG conceptualized, reviewed literature, wrote, and edited this paper.