
Abstract
Introduction:
Clinical performance varies due to academic, clinical, and behavioral factors. However, in many countries, selection of medical professionals tends to focus on exclusively academic ability and clinical acumen. Appropriate selection processes for medical professionals should consider behavioral factors, which may vary across contexts. This study was conducted to identify behavioral competencies considered relevant for effective medical practice in Nigeria, by medical students and doctors, and compared with other contexts.
Methods:
This mixed methods study draws on a scoping review and nominal group technique exercises. We undertook a scoping review to develop a list of behavioral attributes that may correlate with effective service provision in the empirical literature, across contexts. Drawing on nominal group technique exercises with 17 medical students and 11 physicians, this starting list was modified through scoring and ranking of selected competencies. We compared the list of competencies and rankings between medical students, doctors, and the scoping review.
Results:
The scoping review identified 9 articles for full-text review, resulting in a starting list of 21 behavioral competencies defined in studies, all of which had been conducted in non-African countries. The nominal group technique exercises conducted with medical students and doctors yielded a condensed list of 32 and 27 behavioral competencies respectively. For doctor-client interactions, effective communication and patient-centeredness were ranked highly, while for doctor-colleague interactions, teamwork, respectfulness, and management ability were ranked highly. There were also divergences in the condensed list of behavioral competencies and the scoping review, which may be explained by cultural and non-cultural factors.
Discussion:
This study is one of the few to examine the perspectives of medical students and physicians on behavioral competencies for effective medical practice in an African country. We found differences in the perspectives of medical physicians and students, and in the prioritized competencies across countries. Our study illustrates the need for careful consideration in identifying subject matter experts and in generalizing competencies across contexts. Future research in this field in Nigeria should examine effective ways of testing for key behavioral competencies among medical students and for residency programs. Also, investigating the perspectives of medical faculty and administrators on important competencies, and exploring the generalizability of these competencies across cultures in Nigeria should be considered.
Introduction
The Hippocratic Oath includes a pledge by the physician, “in purity and holiness, to guard [one’s] life and art.” 1 Since the classical period, appropriate behavior of the physician has been considered important for medical practice. The overall performance of a physician can be attributed to structural factors such as academic and clinical skills, as well as behavioral factors that influence relationships with colleagues and clients. These factors explain the performance of medical students and doctors. Academic and clinical performance have been shown to account for only 23% of performance in undergraduate medical training and 6% at the postgraduate level. 2 Hence, behavioral factors contribute considerably to the overall performance of physicians.
In many countries, the selection of medical professionals tends to focus exclusively on academic ability and clinical acumen.3,4 However, appropriate selection processes for medical professionals should also assess for behavioral attributes that are compatible with high-quality health care provision. 5 The renewed attention being given to strengthening the quality of health care globally to facilitate improved health outcomes, is further impetus to revisit this norm to ensure that medical professionals have the academic and behavioral competencies for effective care.6-8
There is a growing body of literature that focuses on defining, identifying, and measuring the values and behavioral competencies for medical practice, to inform selection processes. 4 Patterson and Zibarras, 4 in their seminal report on the selection and recruitment of medical professionals, addressed these pre-requisites. Values were defined in literature as enduring beliefs one holds about what is a preferable state of things and provide principles that guide one’s actions or behavior.4,9 Patterson and Zibarras, 4 clarified that to measure these values in medical professionals, an appropriate selection system must clearly identify the attributes or behaviors that reflect these values. This system should derive these key attributes from individuals who have direct experience in or have a good understanding of the role and are thus subject matter experts. 4 In line with these recommendations, studies in high-income countries have examined the perspectives of medical students and professionals, who can be considered subject matter experts on the qualities and behaviors of a high-performing physician.10,11
There have also been efforts in low and middle-income countries, particularly in Asia, to specify technical and non-technical competencies for medical students and graduates. 12 However, there is a relatively limited literature that investigates behavioral competencies among medical professionals in African countries. 13 Translating behavioral competency definitions and lists from one context to another may have unintended consequences, including the marginalization of priorities and values of one country relative to others.14,15 The context in which medical professional selection happens also matters because service delivery problems vary and require different attributes or behaviors for an appropriate response. 13 Thus, there are potentially cultural (differing priorities and values) and non-cultural (differing service delivery challenges) reasons why behavioral competencies should be context-specific. Hence, a scoping review of literature advocated for further research through qualitative studies. The review advocated for in-depth exploration of forces that shape the selection of health professionals across contexts. 13
Our study responds to this research gap, focusing on Nigeria. The objective of this study was to identify behavioral competencies considered relevant for effective clinical practice in Nigeria, by triangulating a scoping review and nominal group technique (NGT) exercises. We explored differences and similarities in the perspectives of different groups of subject matter experts and compared these with findings reported in global literature to enable a more nuanced description.
Methods
Scoping review
Scoping reviews are an ideal tool to determine the coverage of the body of evidence on a topic.16-18 These reviews can help to identify the types of evidence in a field, examine how research in a field is conducted, identify the key characteristics of a concept, inform a systematic review, and analyze knowledge gaps. 17 Through a scoping review, we identified behavioral attributes that correlate with effective service provision and which are not indicators of clinical acumen or academic performance. The behavioral attributes from the scoping review served as discussion prompts in the group exercise described later in this section.
We undertook steps in the scoping review in line with the guidance provided in a seminal paper by Arksey and Malley. 16 We identified the research objective of the scoping review as aiming to describe behavioral competencies required for medical practice. We then performed a search on Google Scholar and PubMed for relevant studies, including peer-reviewed articles and gray literature, published in English, between 1st January 2007 and 30th June 2019, regardless of methodology or country of focus. The search algorithm included the following terms: (((values) OR (behavior) OR (competence)) AND ((medical practitioner) OR (doctor) OR (medical professional) OR (health practitioner) OR (health professional) OR (auxiliary professional)) AND ((non-cognitive) OR (non-clinical) OR (non-academic)) AND ((selection criteria) OR (selection process) OR (situational judgment test) OR (review))).
Following the initial search, the title and abstract of each publication were reviewed by 2 independent reviewers to verify compliance with the inclusion criteria described above. Bibliographies of identified studies were also reviewed to identify other publications that could be eligible for inclusion. The review process was managed manually. Data were extracted using a Microsoft Word template designed by the researchers with the following headers: (i) document source (eg, PubMed, Google Scholar); (ii) full reference or citation of the article; (iii) website link; (iv) indicate whether full text or abstract is available; (v) country or sub-region and; (vi) methods (eg, survey). The full text of the final set of included studies was reviewed by 2 independent researchers to extract information on (i) the behavioral competencies required for medical practice and (ii) the definitions of the identified behavioral competencies (if any). Drawing on these definitions, duplications were removed, and a list of non-overlapping behavioral competencies was derived through deliberations and consensus by the team of reviewers. Discrepancies between reviewers were resolved by consensus or with the help of a third reviewer.
Nominal group technique (NGT) exercise
The NGT is a group consensus-building method that aggregates the opinions of individuals that have experienced a phenomenon using a structured format.19-21 Through anonymous voting, it promotes equal opportunity for participants to contribute, reduces the influence of dominant speakers in group interactions, and ensures that individual voices do not skew the debate. For this study, we used NGTs to elucidate the consensus of medical students and professionals on the behavioral competencies required for physicians to provide effective care.
The NGT exercises were conducted in May—June 2019 in the College of Medicine, University of Nigeria. The participants were physicians involved in clinical practice and training, including medical students and doctors in the affiliated teaching hospital. We believe that the input of this group will contribute to underlining more formal guidelines for intake into medical training. At the face-to-face recruitment, participants were informed that the aim of the study was to determine important behavioral competencies required for medical practice in Nigeria.
The study team purposively selected twenty medical students in the penultimate and final year of clinical training, and who had thus been exposed to rotations in internal medicine, surgery, pediatrics, obstetrics and gynecology, and community medicine, of whom 17 (11 males and 6 females) consented to participate. The study team also purposively selected 20 medical residents, equally distributed among the main clinical specialties: internal medicine, surgery, pediatrics, obstetrics and gynecology, and community medicine. Eleven residents (3 males and 8 females) consented to participate.
We held one NGT with medical students in May 2019 and another with medical residents in June 2019. Discussions were held in a quiet, secluded room situated in the University teaching hospital. All discussions were conducted in English and audio-recorded with the consent of the participants. Hand-written notes describing the group interactions were taken by a member of the research team.
Each NGT started with a review of the objective of the discussion and the process of conducting NGTs. The starting list for the discussion was derived from the results of the scoping review on the global evidence on behavioral competencies required for medical practice.10,11,22-28 These competencies were grouped by the participants based on their relevance for interactions with clients or colleagues. During the NGT exercise with resident doctors, this starting list had been modified to reflect the list of competencies generated from the first NGT exercise with the medical students.
The study question of identifying behavioral traits that are essential to effective practice among medical professionals was restated. In round-robin fashion, which is with 1 response per person per round, everyone in the group was given the opportunity to add to the starting list, with 3 rounds in total. The responses were recorded on a flip chart without criticism. Repetitions and overlaps between responses were noted, clarifying questions were asked when needed, and participants attempted to provide definitions for each competency.
Based on the updated list, participants were asked to anonymously select and then rank 5 most relevant competencies for interactions with clients and with colleagues. Each list of 5 competencies was then ranked in order of importance for effective practice, with “5” indicating the most important competency and “1” indicating the least important competency. The aggregate score for each competency was generated by summing the numerical scores. Results from the voting and ranking were discussed. Participants were then asked to re-rank their original top 5 ideas for each interaction. The aggregate score for each behavioral competency and changes from the first round of voting were calculated. The highest possible score a competency could have was dependent on the rank assigned by participants (rank 1-5) and the number of participants in the NGT exercise. In the first NGT exercise with 17 participants, the highest possible score a competency could have was 85, while in the second NGT exercise with 11 participants, the highest possible score was 55.
Drawing on the updated list and definitions, we triangulated our findings across the scoping review and NGTs. We compared the final list of competencies defined by medical students with medical doctors, and the respective rankings of each competency for doctor-client and doctor-colleague interactions using an arbitrarily-selected decision rule (aggregate ranking of greater than equal to 10) that reflected relative consensus on the importance of the competency. We then identified parallels between behavioral competencies common across both groups and the results of the scoping review of the global literature.
Three members of the research team are physicians, who have experience providing primary and specialist care. The other member of the research team has a graduate degree in health promotion and communication. One of the members of the research team with significant prior experience conducting NGT exercise provided training to the other team members involved in data collection. The guide for the NGT was also discussed with experts from other disciplines, to ensure that the guide and probes were free of pre-conceived opinions of the research team on the subject matter. The study findings have been reported in line with the consolidated criteria for reporting qualitative research (COREQ). 29
Results
In the scoping review, the initial search on Google Scholar and PubMed yielded 10 citations, of which 8 were peer-reviewed publications and 2 were gray literature. Following a review of the titles and abstracts of the citation, a total of 4 papers were excluded for not meeting the inclusion criteria, and the remaining 6 citations were given a bibliography review to identify other relevant articles. A total of 6 new citations were identified following the bibliography review, 3 were excluded and the total number of publications included in the full text review was 9.
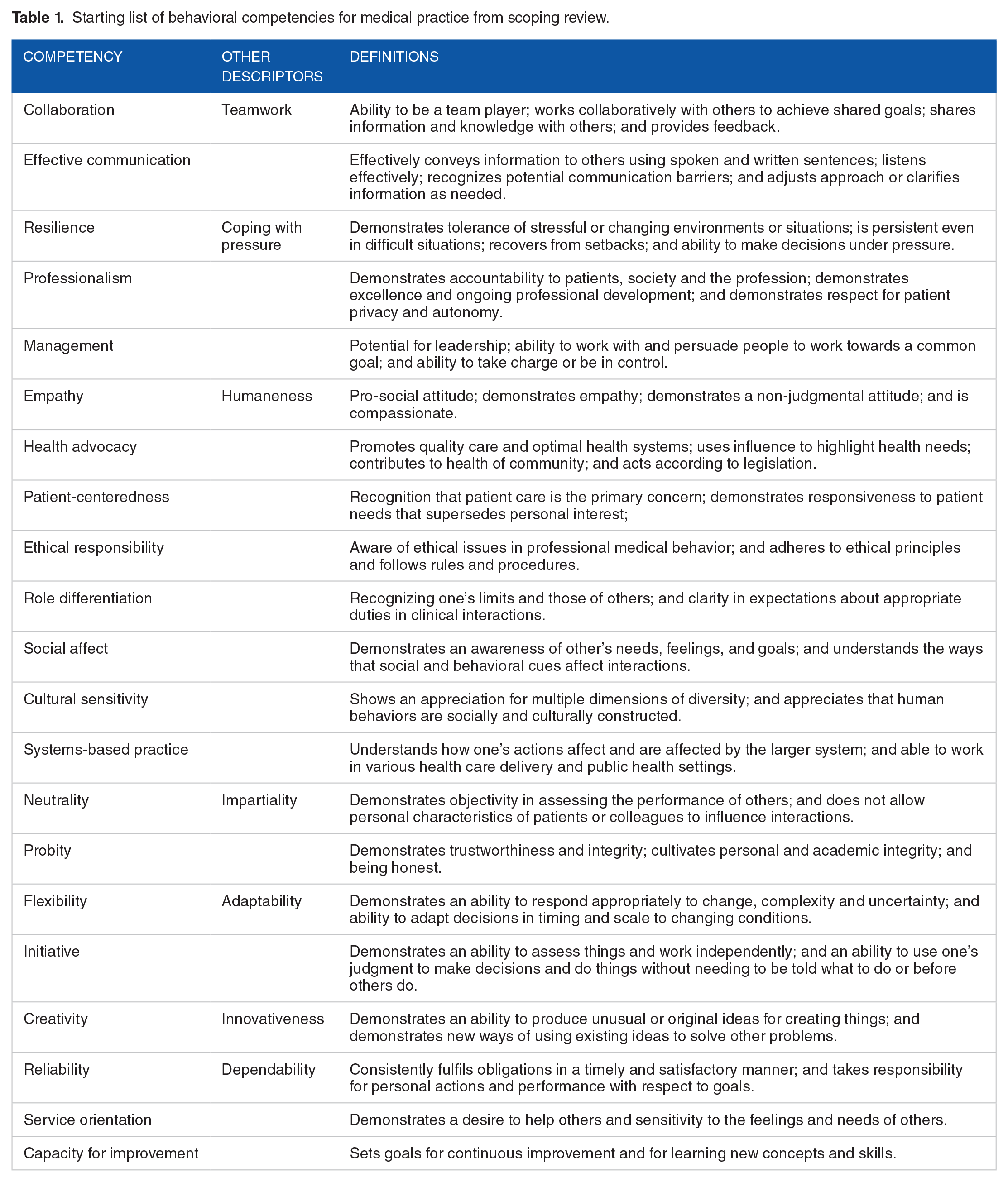
The scoping review resulted in a starting list of 21 behavioral competencies defined in Table 1: collaboration, effective communication, resilience, professionalism, management, empathy, health advocacy, patient-centeredness, ethical responsibility, role differentiation, social affect, cultural sensitivity, systems-based practice, neutrality, probity, flexibility, initiative, creativity, reliability, service orientation, and capacity for improvement.10,11,22-28
Starting list of behavioral competencies for medical practice from scoping review.
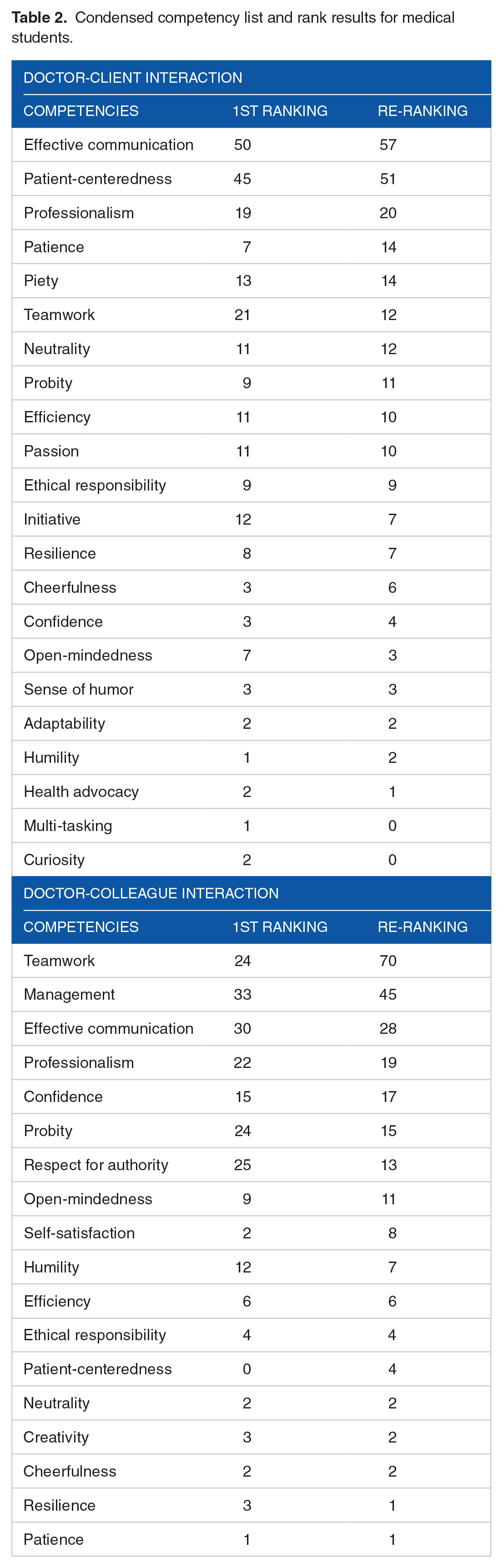
Following round robin contributions, the NGT with medical students and doctors yielded 63 and 42 competencies respectively. Elimination of overlapping concepts condensed the list of behavioral competencies to 32 for medical students and 27 for medical doctors. All the medical students and doctors were involved in the initial ranking exercise for the top 5 behavioral competencies, while 1 medical doctor opted out of the re-ranking exercise following a discussion of the aggregate rank results. The voting results for the condensed list of competencies for medical students and doctors are shown in Tables 2 and 3. Top ranked competencies for doctor-client interactions were effective communication, patient-centeredness, empathy, and professionalism. Top-ranked competencies for doctor-colleague interactions were teamwork, team leadership and management ability, effective communication, respectfulness, and professionalism.
Condensed competency list and rank results for medical students.
Condensed competency list and rank results for medical doctors.

A comparison of the voting results between medical students and doctors revealed commonalities and divergences in the competencies considered important for doctor-client and doctor-colleague interactions (Table 4). For doctor-client interactions, the behavioral competencies considered most important by both groups were teamwork and patient-centeredness while for doctor-colleague interactions, both groups ranked teamwork, respectfulness, and management ability highly. However, there were clear divergences between groups. For doctor-client interactions, medical students also ranked effective communication, professionalism, patience, piety, neutrality, probity, efficiency and passion as important, while medical doctors considered empathy and diligence to also be essential. With respect to doctor-colleague interactions, medical doctors specified the importance of conflict management as a sub-set of team leadership and management, while medical students voted other behavioral competencies highly, specifically effective communication, professionalism, confidence, probity, and open-mindedness.
Comparison of medical students’ and doctors’ behavioral rankings for competencies with aggregate ranking of ⩾10 (commonalities in italics).

We explored convergences in the opinions of medical students and doctors in our study, as well as findings from the scoping review, summarized in the starting list, regardless of behavioral competency ranking. These findings are summarized in Table 5. The condensed list for medical students and doctors had 13 behavioral competencies in common, which is equivalent to 48% of the total list for medical doctors and 41% of the total list for medical students. There was a similar level of overlap between the condensed lists for medical students and doctors, and findings from other contexts (starting list derived from scoping review), with 12 common behavioral competencies for medical students and 11 for doctors, which is equivalent to 41% of the total list for medical doctors and 38% for medical students.
Commonalities between condensed lists from NGT exercise and starting list from scoping review.

We conducted 2-way comparisons between our groups to identify competencies that were noted as important (regardless of ranking) in 1 group but omitted in the other. For medical students, these included effective communication, professionalism, piety, curiosity, and a sense of humor. Competencies identified by medical doctors only included accountability, responsibility, good judgment, empathy, diligence, reliability, self-care, and resourcefulness. In Table 6, we have summarized the differences between the condensed lists for medical students and doctors.
Examining divergence between the condensed lists for medical students and doctors.

Finally, we also examined divergence between the condensed lists for medical students, doctors, and the scoping review to highlight the generalizability of findings from other contexts to Nigerian students and physicians. Several behavioral competencies in the scoping review were removed from the condensed list for both medical students and doctors, particularly service orientation, systems-based practice, and social affect. Similarly, the condensed list for medical students and doctors included behavioral competencies in common that were not found in the scoping review, including humility, respect for authority, and multi-tasking (Tables 7 and 8).
Examining divergence between the condensed lists for medical students and the scoping review.

Examining divergence between the condensed lists for medical doctors and the scoping review.

Discussion
Our study of behavioral competencies for the Nigerian medical physician is one of first to have examined this question in an African country. Below, we reflect on the potential significance of the divergence between the perspectives of medical students and doctors, identified competencies, and generalizability across contexts.
The divergence of the elicited competencies between medical students and doctors in our study illustrates the need for careful consideration of who is nominated to be a subject matter expert in identifying qualities to be considered for medical student admissions or graduate residency programs. The differences between these groups may also signal the competencies that may be needed at different points in the training of a medical physician. Thus, while medical students, whose primary responsibilities involve learning and developing skills required for future practice prioritized curiosity, open-mindedness, passion, and a sense of humor; the medical doctors and graduate residents prioritized competencies that enabled them to undertake their duties of service provision within a hierarchical and multidisciplinary medical team including accountability, good judgment, diligence, conflict management, discipline, and accountability. A list of behavioral competencies developed by medical students for doctors may be relevant for navigating a medical residency. There may be value in considering the behavioral competencies enumerated by medical doctors in defining the qualities of students admitted into medical school and in designing the medical curriculum, given the eventual relevance of these values and attributes for medical practice.
The behavioral competencies elicited from the NGT with medical doctors are likely to more closely reflect the needs for actual medical practice than the view of medical students. In that respect, among doctors in our study, the top-ranked competencies for doctor-client interactions were ethical responsibility, empathy, patient-centeredness, diligence, and teamwork, while the top-ranked competencies for interactions with other medical colleagues were respectfulness, teamwork, and leadership ability including conflict management. These competencies overlap with factors identified in other contexts, including the United Kingdom and United States.10,22 In Nigeria, these factors are not explicitly considered in admitting medical students, in decisions on entry into medical or surgical residency programs, or in appointing doctors into permanent positions in hospitals.
Less than 50% of the behavioral competencies identified in the scoping review were retained in the condensed lists of medical students and doctors in Nigeria. The divergence in identified behavioral competencies between participants in our study and the scoping review highlight the difficulty in generalizing across contexts, which has also been identified in the theoretical literature.13-15 Both medical students and doctors in our study identified humility and respectfulness as behavioral competencies that are important for effective practice. This may reflect a cultural context in which respect for elders is a valued attribute, where undergraduate and graduate medical training is led by older physicians. 30 These characteristics were not identified in a scoping review that largely included studies conducted in Western countries. An extensive body of literature has explored the differences in attitudes toward older people in society in Western versus Eastern cultures, with more negative views held in the West, as exemplified by a 1975 study by Erdman Palmore. 31 This finding suggests that differences in culture may shape perspectives on important values and behaviors in professional practice.14,15
There were other divergences between the condensed lists from the NGTs and the scoping review that may reflect non-cultural differences in service delivery across countries. 13 For example, medical doctors in the Nigerian context identified the importance of multi-tasking and self-care while the scoping review highlighted the need for systems-based practice. On the one hand, a Nigerian medical doctor, who works in a resource-constrained environment, may find the need to perform multiple functions that may be ascribed to other members of the medical team in a more advanced economy, such as nurses and physician assistants. This may explain the need to multi-task and to pay attention to emotional well-being, as particularly important attributes of the effective physician in this context. As clinical practice may not have evolved to systematically consider the broader social determinants of health, including health systems, within clinical guidelines and training in Nigeria, physicians did not consider systems-based practice to be an important behavioral competency overall, and eliminated it from the starting list. Thus, non-cultural differences in medical practice across contexts introduce difficulty in generalizing from competencies developed in specific countries.
We have identified several limitations that our study faces. While we included the perspectives of medical students and graduate residents who are practicing physicians, our study may have benefitted from discussions with supervising or consultant medical physicians and medical administrators, who in practice may be involved in defining the required competencies for medical physicians. Regardless, medical students and physicians have been considered as subject matter experts in other studies in the literature given their direct involvement in training and service provision.10-12 Future studies may compare perspectives across these multiple groups to identify the appropriate group to define behavioral competencies in guidelines for medical student admissions, residency program selection decisions, and appointment of medical faculty.
While NGTs provide an objective means of consensus building on behavioral competencies that may be replicated in practice, these methods face important limitations. For example, the voting process may not lead to a convergence of opinions with multiple competencies given low ratings, dominant individuals may influence the re-ranking process during the discussion of initial rankings, ideas may be constrained by the initial list of ranked competencies, and the process may be mechanical relative to other qualitative methods such as focus group discussions. Having considered these limitations, NGTs through anonymous voting and when led by trained facilitators can mitigate some of these negative features, including reducing the influence of dominant individuals and facilitating a more fluid process of arriving at a consensus.
The literature exploring the consideration for behavioral competencies in Nigeria and more broadly, in low- and-middle-income countries is still nascent. There is a possibility that our focus on 2 databases (Google Scholar and PubMed) could have limited the studies we retrieved. However, there is an obvious need for future studies that examine and compare behavioral competencies for medical practice across groups defined by culture and geography. Furthermore, admissions procedures and training curricula that systematically incorporate these competencies need to be developed, pre-tested, and examined for their impact on the performance of medical students and physicians.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The findings, interpretations, and conclusions expressed in this paper are entirely those of the authors. They do not necessarily represent the views of the World Bank and its affiliated organizations or those of the Executive Directors of the World Bank or the governments they represent.
Author Contributions
AC and CM conceptualized the study; AC, CM, UO, and IA designed the study; CM, UO, and IA led the nominal group technique exercises; UO and IA conducted the scoping review; CM analyzed the data; AC, CM, UO, and IA interpreted the data, drafted the manuscript, and were involved in revising the intellectual content of the manuscript. All authors read and approved the final manuscript.
Ethical Approval
Approval for this study was obtained from the University of Nigeria Teaching Hospital Health Research Ethics Committee (NHREC/05/01/2008B-FWA00002458-1RB00002323). All participants provided written informed consent to participate in the study.