
Abstract
OBJECTIVES
Best practices for content selection, mode of delivery, and timing of pediatric clerkship readiness curricula for medical students have, by and large, not been established. Capitalizing on changes in structure of the clinical clerkships during the COVID-19 pandemic, we created an upfront clerkship readiness curriculum, termed Pediatric Intersession (PI), to replace the existing weekly lecture-based clerkship didactics.
METHODS
Our goal was to develop an interactive curriculum with innovative instructional design methodology intended to promote broad foundational pediatric knowledge and clerkship preparedness using case-based learning. We first conducted a needs assessment and crafted curriculum content using guiding principles from the 2019 Council on Medical Student Education in Pediatrics (COMSEP) curriculum. We then organized material into four daily modules prior to the start of the clerkship and employed flipped classroom (FC) methodology.
RESULTS
Sixty-six percent of students completed course evaluations, and >90% of the 100 respondents reported that the PI enhanced their clinical learning. Pre-/post-testing demonstrated some knowledge gain following the small-group sessions and there was no change on the National Board of Medical Examiners (NBME) Subject Exam mean scores compared to prior cohorts of students.
CONCLUSIONS
The global pandemic provided an opportunity to re-envision our pediatric clerkship didactics content, while also incorporating instructional design methodology preferred by students. Our curriculum promotes a small group-based, interactive approach to clerkship readiness that fosters learning in the clinical environment that can be adapted for various settings. Our evaluation suggests that the transition to a FC readiness curriculum can be done successfully while effectively preparing students for their pediatric clerkship.
Keywords
Introduction
As undergraduate medical education (UME) pre-clinical curricula tend to highlight adult-oriented pathophysiology and clinical skills, medical students receive comparatively less and more variable exposure to pediatric content.1-3 In fact, medical students are generally perceived as less prepared for the pediatric clerkship (PC), both by PC directors and by the students themselves.4-7 Students therefore rely on pediatric-specific didactics delivered during the clerkship in order to supplement and solidify wards-based learning.
Pediatric clerkship didactics have been previously described in the literature.1-3,6,8 Importantly, prior curricula have been generally designed as standalone modules addressing specific knowledge gaps and are not intended to be combined into a comprehensive curriculum for clerkship readiness (defined for the purposes of this study as student-reported sense of preparedness for the PC). 6 There is also uncertainty regarding the timing for delivery of clerkship content where some institutions have adopted longitudinal integrated clerkship curricula. 7 Overall, there remains a need for best practice recommendations on how and when to deliver pediatric core clerkship content that students will enjoy while simultaneously preparing them for clerkship success.4-7
Methods
Problem identification and needs assessment
The clinical clerkship year begins in January of second year and ends in December of third year. Previously, PC didactics occurred once per week with lecture-based instruction. However, when the COVID-19 pandemic forced all clinical clerkships to accommodate obligate quarantine periods, we were compelled to re-imagine PC-specific didactics overall, with respect to content, structure, and delivery.
Employing Kern's six-step framework for curriculum design, 9 we conducted a needs assessment including review of course evaluations, existing literature, national curricula; informal focus groups with medical students; and meetings with other specialty clerkship directors and external PC directors. Findings suggested that (1) students have a strong understanding of basic pathophysiology but limited pediatric fund of knowledge and minimal competency in most pediatrics-specific clinical skills; (2) students expect interactivity in sessions and often prefer self-directed learning; 10 and (3) students prefer to choose from a variety of media to prepare for teaching sessions, patient care, and the required National Board of Medical Examiners (NBME) Subject Exam. 11
We identified flipped classroom (FC) methodology as a potential instructional design strategy to address the above findings.10,12 An additional literature review suggested that core clerkship didactics utilizing FC methodology had been described in a small number of instances (including within obstetrics-gynecology, 13 radiology, 14 surgery, 15 and ophthalmology 16 clerkships). To our knowledge, there has been no description of FC application to pediatric clerkship readiness in existing literature.
Goals and objectives
We created a virtual pre-clerkship readiness curriculum, termed Pediatric Intersession (PI), using an FC 12 approach. Our goal was to provide foundational clinical knowledge needed for clerkship success while promoting student-driven, case-based learning. We sought to determine the acceptability and feasibility of our PI and to better understand how the transition of PC content to an FC format compares to prior lecture-based instruction.
Educational strategies
We selected PI instructional design and curricular content to reflect the results of the needs assessment. The FC 12 approach allowed us to encourage the acquisition of foundational knowledge through self-paced learning prior to class, with class time devoted to targeted application and integration of knowledge through case-based discussions. We blended asynchronous preparation and virtual synchronous case analysis and synthesis over four days, focusing on the following key topics: (1) nutrition, growth, and development; (2) respiratory illnesses; (3) febrile illnesses; and (4) the acutely ill child (Table 1). Topics were selected after synthesizing the 2019 Council on Medical Student Education in Pediatrics (COMSEP) curriculum and incorporating areas of student and educator-perceived weakness identified from the needs assessment. 17 Case-based instruction encompassed review of pertinent historical elements, physical exam findings, differential diagnosis, evaluation, initial management, and review of key concepts related to the case (ie, intravenous fluid calculations for pediatric patients presenting with dehydration).
Overview of Pediatric Intersession (PI) structure.
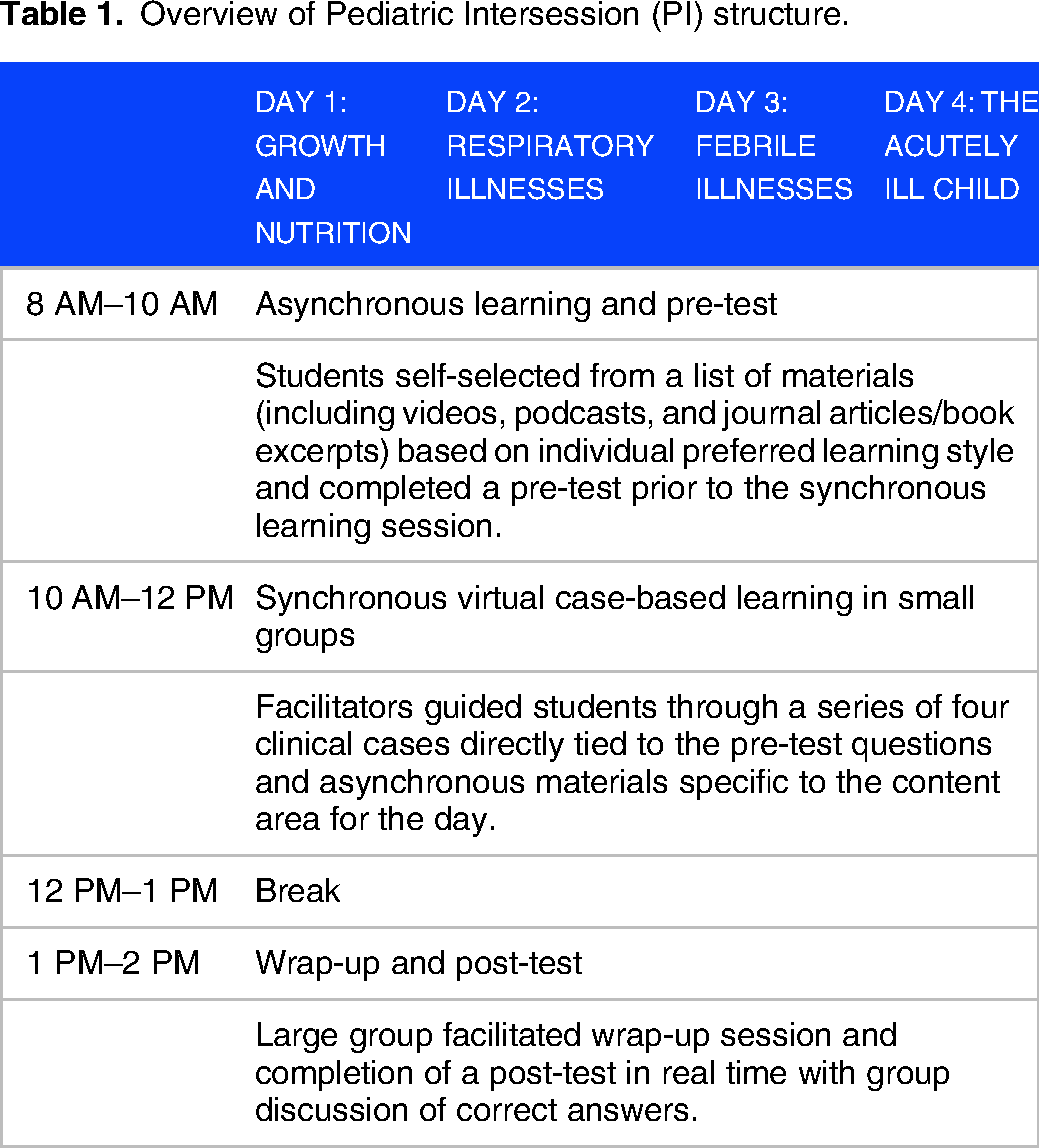
Instructional design was further grounded in the assumption of self-determination theory that learners require perceived autonomy (as well as competence and relatedness) to feel engaged in learning. 18 Prior to each day, students received a list of recommended resources. Students were able to self-select asynchronous materials (including videos such as 20–30 min prerecorded PowerPoint lectures, podcasts, and journal articles/book excerpts) based on individual preferred learning style. Videos were created by educators at our institution. Each day was designed to include asynchronous learning time with completion of a pre-test assessment, followed by facilitated virtual synchronous case-based learning in small groups. Finally, each day ended with a large-group wrap-up and post-test assessment completed by each participant. Pre-test questions were content-specific questions related to the learning objectives for the day and ranged from 6–8 multiple-choice questions per day. Pre- and post-test questions were the same for each day and optional for all students (Supplemental Appendix 1). Questions were reviewed by PI course faculty prior to implementation. Our session materials are available upon request to educators who are interested in implementing aspects of this curriculum into their programs.
Small-group facilitators, including faculty and fellows within our institution's Department of Pediatrics, were recruited in advance of each session. Facilitators received case materials and facilitator guides ahead of the session and no prior knowledge of the curriculum was required. Students were assigned to learning teams of 4–7 students per facilitator; they remained in consistent groups for all synchronous small group sessions throughout the four-day period to promote a sense of relatedness.
Implementation
We pilot-tested the curriculum during its first iteration in January 2021, eliciting feedback from students and small-group facilitators that informed minor adjustments to the assessment questions (to increase total correct responses), curricular content (additional audiovisual resources), and PI structure (additional time allowed for asynchronous work). All clerkship students participated in this mandatory curriculum immediately prior to their PC. The PI was delivered every 12 weeks (Supplemental Appendix 2). There were no exclusion criteria.
Evaluation and feedback
We reviewed the data from the entire academic year of 2021 (January–December) and completed data analysis by August 2022. Students completed a voluntary, confidential course evaluation at the end of the week administered by the medical school. The course evaluation components specific to the PI included one yes-no question related to perceived clerkship preparedness, one question specific to students’ ability to complete the pre-work during asynchronous time, two Likert scale questions related to preparation for and appropriateness of pre-test questions, and one open-ended question for free text comments. De-identified results were released to clerkship directors after each PI. Authors reviewed all free text comments relevant to the PI, independently assigned valence (positive, negative, or neutral) to each comment, then compared valence assignments with discussion among the group until consensus was achieved. Additionally, all students after completion of the PC were informally surveyed via email by student course representatives to assess course satisfaction and clerkship readiness. Student NBME Subject Exam scores were compared from the PI year to the prior five years as a separate measure of student performance. Curricular evaluation methods were determined not to meet criteria for human subjects research by the Institutional Review Board at the Children's Hospital of Philadelphia.
Statistical analysis
We evaluated knowledge acquisition using assessment via pre- and post-test questions. The median and interquartile range for the number of correct responses for questions in the pre- and post-test groups by day and block were calculated. Pre- and post-test data from Block A was used for pilot purposes only (n = 40). We reviewed the difference in distribution between pre- and post-test scores using a Wilcoxon signed rank test at the group level as the data was not paired by student. We evaluated for differences in score for the NBME subject exam for each year compared to the 2021 year using a two-sample t-test for difference of means. Data analysis was performed using Stata 16 (StataCorp LP, College Station, TX).
Results
We completed four sessions with a total of 152 clerkship-year medical students from January 2021 to December 2021 (40, 40, 36, and 36 students, respectively); these sessions were inclusive of all students completing their clerkship year in 2021.
Knowledge gain
In Block B, 38 students (95%) completed the pre-test, and 30 students (75%) completed the post-test secondary to issues with polling software; in Block C, 36 students (90%) completed the pre-test, and 28 students (70%) completed the post-test; and in Block D 35 students (97%) completed the pre-test and 34 students (94%) completed the post-test. We saw an increase in the percentage of correct responses for the Day 3 case (median pre-test 86% correct, post-test 97%; p-value 0.04) only. The median and interquartile range for all available data is shown in Table 2. There was no significant difference in student NBME subject exam scores in the PI year compared to the five years prior (Table 3).
Comparison of pre- and post-test scores for each student group by day and block.

Note: Day 1: Growth and Nutrition; Day 2: Respiratory Illnesses; Day 3: Febrile Illnesses; Day 4: The Acutely Ill Child. Block A data was for pilot testing purposes only and is excluded from the table. Missing data for Blocks B and C due to polling software difficulties are excluded from the table. Abbreviation: IQR, interquartile range.
Mean annual National Board of Medical Examiners (NBME) subject exam scores (2016–2021).
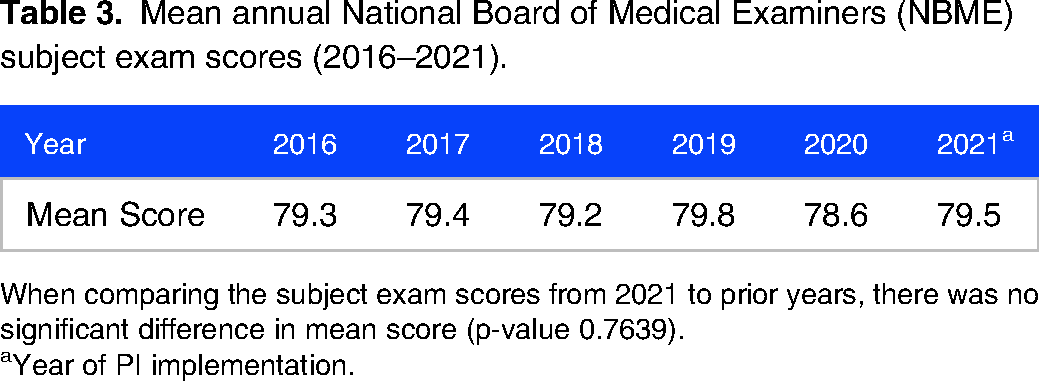
When comparing the subject exam scores from 2021 to prior years, there was no significant difference in mean score (p-value 0.7639).
Year of PI implementation.
Acceptability and clerkship readiness
Sixty-six percent of students completed course evaluations throughout the academic year (Blocks A-D). More than 90% of students who completed the course evaluations reported that the small group facilitated cases enhanced their clinical learning (Table 4). The majority of students reported being able to finish the prework during the asynchronous time and felt that the prework prepared them for the facilitated cases (Table 4). Students reported that the pre-/post-test questions were appropriate for their level of learning. There were 36 positively valanced, 6 neutral, and 16 negatively valanced free text comments from the PI course evaluation. Of the positively valanced comments, students reported that the PI was an enjoyable, well-organized, well-structured course that was overall a good introduction to the PC. Students reported enjoying the FC instruction. Of the negatively valanced comments, five students reported not having enough time during the asynchronous session, referring to the optional journal article readings in particular; three of those students, as well as two additional students, requested additional video resources in place of reading assignments. Example student reflections on the PI from course evaluations are shown in Table 5. Of eight total respondents on the course representative survey, all indicated that the PI curriculum allowed them to feel well-prepared for the PC. The remaining students opted not to complete the voluntary survey.
Pediatric Intersession (PI) survey responses from the clerkship evaluation administered by the medical school.

Clerkship evaluation questions that were not relevant to the PI are excluded from the Table. N = 100 across Blocks A-D. Abbreviation: SD, standard deviation.
Narrative comments about the Pediatric Intersession (PI).

Representative comments taken from course evaluations (total: 100 (66%) evaluation responses with 36 positively valanced, 6 neutral, and 16 negatively valanced free text comments across all four blocks).
Discussion
Our PI was designed as a comprehensive PC readiness curriculum using an interactive small group FC format. Our curriculum evaluation, specifically our post clerkship evaluation questionnaire, suggests that content, timing, and instructional design were well-received by students, and that all voluntary respondents felt well-prepared for the clerkship. Moreover, students performed equally well on the NBME as compared with prior cohorts that received traditional clerkship didactics. These findings suggest that clerkship didactic curricula can be reformatted to prioritize clerkship readiness without compromising student satisfaction or academic performance.
Our finding of self-reported clerkship readiness by students is noteworthy. Clerkship readiness is critical to successful performance, and it may alleviate some of the profound stress associated with the transition from preclinical to clinical learning.19-21 Given that students have historically reported limited pediatric clerkship readiness,4-7 curricula that achieve improved pediatric-specific competencies are needed. Practically, however, the breadth of introductory pediatrics content is difficult to cover effectively in traditional lecture format while maintaining student engagement. Thus, we were pleased that the majority of feedback about our interactive, student-driven FC approach was positively valanced.
While many institutions nationwide have adopted FC methodology for core didactics,13-16,22 we are the first pediatric group, to our knowledge, to directly describe its implementation. When compared with students receiving traditional lectures, prior studies have shown that students receiving content via FC performed at a similar level on standardized assessments but were generally more satisfied with their clerkships.12-15 We saw similar findings related to unchanged NBME scores but, importantly, positive evaluation feedback with our PI. Students praised the incorporation of preferred learning modalities such as podcasts and videos with asynchronous instruction as part of FC methodology but noted the time required to prepare for sessions and requested even more video-based resources. These findings align with recent studies outlining the benefits of technology-based resources as part of clerkship learning.22,23
Finally, the timing of our PC readiness curriculum, delivered in an uninterrupted sequence prior to the clerkship, did not appear to improve the overall knowledge of students as it relates to NBME scores. We did, however, note an unanticipated benefit: without required afternoon didactics, students were present on the clinical wards and, presumably, more immersed in their clinical experiences. Anecdotal feedback from stakeholders was also positive: attendings and residents valued uninterrupted time with learners, and students appreciated not needing to juggle clinical and non-clinical responsibilities. As such, the timing and delivery of our PI may serve as a feasible alternative to the longitudinal integrated didactic approach standard at other institutions.7,24 Notably, institutions that have moved toward an upfront clerkship preparedness design have struggled to find metrics capable of assessing curriculum effectiveness compared to prior curricula. 25 We would favor additional studies investigating how an upfront readiness curriculum versus a longitudinal schedule may impact students’ career choice, perception of connectedness to patients and team-members, and professional identity formation.
Our curriculum is not without limitations. It is both faculty and time-intensive, requiring four dedicated days for instruction. While we delivered the PI in an uninterrupted sequence, the curriculum could be separated and interspersed throughout the clerkship. The feasibility of FC methodology should also be considered given the time it takes for learners to complete pre-work.14,16 That said, our curriculum was specifically designed to include dedicated time for asynchronous learning, mitigating some of this burden on students. Our curricular content was based on findings from our needs assessment, which may impact its generalizability; however, we feel its instructional design methodology is relevant to educators across institutions. Our assessment of knowledge acquisition was also limited by low post-test response rates, particularly in early course iterations. Notably, the data became more robust as comfort with polling software improved. We additionally utilized no validated evaluation questionnaires. Our course representative survey had a low number of responses which is consistent with prior cohorts, as most students choose to reserve clerkship feedback for the mandatory clerkship evaluation form. Finally, we had no comparison group as this was out of the scope of our study.
Conclusions
Prompted by a unique opportunity during a global pandemic, we restructured the content, structure, and delivery of core PC didactics. Our experience suggests that PC didactics can be feasibly and successfully converted to an FC model to promote clerkship readiness and case-based learning with equivalent performance on standardized assessments. Future study will include systematic comparisons of different didactic structures to inform ongoing curriculum development that will best promote medical students’ satisfaction, sustained knowledge gain, and clerkship success.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241229774 - Supplemental material for Pediatric Intersession: An Upfront Flipped-Classroom Curriculum to Promote Pediatric Clerkship Readiness
Supplemental material, sj-docx-1-mde-10.1177_23821205241229774 for Pediatric Intersession: An Upfront Flipped-Classroom Curriculum to Promote Pediatric Clerkship Readiness by Morgan Congdon, Laura Goldstein, Kristin D. Maletsky, Meghan Craven, Stacey Rose and Erin Pete Devon in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205241229774 - Supplemental material for Pediatric Intersession: An Upfront Flipped-Classroom Curriculum to Promote Pediatric Clerkship Readiness
Supplemental material, sj-docx-2-mde-10.1177_23821205241229774 for Pediatric Intersession: An Upfront Flipped-Classroom Curriculum to Promote Pediatric Clerkship Readiness by Morgan Congdon, Laura Goldstein, Kristin D. Maletsky, Meghan Craven, Stacey Rose and Erin Pete Devon in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205241229774 - Supplemental material for Pediatric Intersession: An Upfront Flipped-Classroom Curriculum to Promote Pediatric Clerkship Readiness
Supplemental material, sj-docx-3-mde-10.1177_23821205241229774 for Pediatric Intersession: An Upfront Flipped-Classroom Curriculum to Promote Pediatric Clerkship Readiness by Morgan Congdon, Laura Goldstein, Kristin D. Maletsky, Meghan Craven, Stacey Rose and Erin Pete Devon in Journal of Medical Education and Curricular Development
Footnotes
Author contributions
Congdon and Goldstein crafted and delivered curriculum content, analyzed the data, drafted the initial manuscript, and revised the manuscript. Maletsky and Craven crafted and delivered curriculum content and revised the manuscript. Rose and Pete Devon conceptualized and designed the curriculum, contributed to data collection, and critically revised the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Consent for publication
Consent was waived given exemption by the Institutional Review Board as there was no direct or indirect risk to study subjects.
Data availability
All data generated or analyzed during this study are included in this published article (and its supplementary information files).
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate:
Curricular evaluation methods were determined not to meet criteria for human subjects research by the Institutional Review Board at the Children's Hospital of Philadelphia.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.