
Abstract
Purpose:
Investigate whether number of logged Accreditation Council for Graduate Medical Education (ACGME) surgical cases correlates with likelihood of Virginia Commonwealth University Health System (VCUHS) ophthalmology residents being selected as the chief resident.
Design:
Retrospective study.
Participants:
VCUHS ophthalmology residents from 2006 to 2016.
Methods:
Analyze association between chief resident selection and logged cases.
Main outcome measures:
Review number of archived logged ACGME surgical cases of all residents between the years 2006 and 2017. Review chief resident selected each year 2006-2016.
Results:
Our analysis correctly predicted the chief resident in 2 of the 10 years analyzed.
Conclusion:
Those residents performing the most surgical procedures in each respective class were not more likely to be selected as chief resident.
Keywords
Purpose
Ever since Dr. William S. Halsted coined the term “chief resident” in 1899, the position has been held in high regard.1-3 Despite such respect, the role has not been well defined 1 and the way the position is garnered is even less well understood.1,2,4-8 Divisions such as emergency medicine, psychiatry, family medicine, pediatrics, and radiology have examined the chief resident role and provided good insight.1,2,4-11 To date, there has been no published literature on the chief resident within a surgical specialty, including ophthalmology. Moreover, the selection process has been rather vague and mostly inundated with bias. Methods of selection vary among training centers with either peers, faculty, program directors, or chairpersons serving as the main voice.1,2,4-8 In an effort to provide a guide for an unbiased selection process, we sought to determine whether the number of surgeries performed correlated with the selection of the ophthalmology chief resident at Virginia Commonwealth University Health System (VCUHS).
In 1940, the Commission on graduate medical education listed duties of the chief resident within the practice of psychiatry. 1 Aside from this, there has been no formal definition of the chief resident role. Without defined roles, it is difficult to select the proper person to fill the chief resident position. Characteristics such as good teaching skills, personality, leadership qualities, organization, strong peer advocacy, popularity, and even sense of humor have been cited as important in the selection of a chief resident.1,2,4-7,9-11 Given the frequent demand for high performance, under very stressful situations, often times at all hours of the day and night under constant scrutiny from attending ophthalmologists, one would suppose emotional intelligence should be considered in the selection of the ophthalmology chief resident. Emotional intelligence can be divided into four attributes: self-management, self-awareness, social awareness, and relationship management. Although these are four great attributes to have in any leader, Kilpatrick et al 8 showed although emotional intelligence improves with age, is a teachable skill, and is higher in women, administrative chief residents did not demonstrate higher emotional intelligence than their classmates. With the exception of Panicek and Caravelli, 7 most studies cited scholastic achievement as an important characteristic. In 1949, Ashford stated, “A man should receive responsibility as rapidly as he acquired knowledge and demonstrates the ability to take responsibility.” 3 Yet in still, this ability to accept such a responsibility is subjective at best. Considering the aforementioned characteristics, bestowing the chief residency position is still rather misguided and arbitrary.
Bias is common, normal, and ubiquitous. 12 It is even present in the assessment of the quality of journal manuscripts. Even judges, the personnel we appoint to be impartial, have been shown to give more lenient sentences after eating—which the judges denied. 12 To help alleviate bias in residency education, Dickey et al go on to propose a simple Microsoft excel–based program that graphs competency development over time equitably and transparently when assessing residents that may be helpful as an objective measure to aide in selection of a chief resident. Our study aimed to provide a measure by which residents could be judged against their peers in an unbiased manner. Simply put, would the number of Accreditation Council for Graduate Medical Education (ACGME) logged surgical cases performed correlate with the likelihood of VCUHS ophthalmology residents being selected as chief resident?
Methods
Prior to beginning this project, the study was submitted to the VCU office of research and innovation for institutional review board (IRB) review. It was found not to be subject to the regulations of Health and Human Services Regulations for the Protection of Human Subjects and therefore the IRB/Ethics Committee ruled that approval was not required for this study. This retrospective study was performed using logged data by residents archived into the ACGME Case Log System (www.acgme.org/Data-Collection-Systems/Case-Log-System) from 2006 to 2017. The data obtained from the ACGME also included the national average for the various procedures or categories for each respective year. To identify the respective chief resident each year, the records of the residency coordinator of VCUHS department of ophthalmology were used. The names were de-identified and assigned a number only known to the residency coordinator and therefore no informed consent was obtained. At the conclusion of our data collection and analysis, the residency coordinator identified the selected chief resident with an asterisk adjacent to the de-identified number among each resident class. Based on the vast number of surgical procedures available within ophthalmology, we created 8 broad procedure categories based on procedural similarities to the specific area involved and type of procedure (Table 1). For example, the category of “Corneal Surgery” included all penetrating keratoplasty, pterygium excision, refractive surgery, LASIK, and other unnamed surgeries involving the cornea. We excluded the 2009-2010 year given there was only 1 resident instead of 3.
List of procedures included for each category of procedure.

To determine whether there is a correlation between being selected as the VCUHS ophthalmology chief resident and the volume versus type of procedures performed, the data were analyzed with principal components analysis (PCA). PCA is a method that reduces data dimensionality by performing a covariance analysis between variables as well as correcting for overlapping information between 2 or more correlated indicators. PCA is recommended as an exploratory tool to uncover unknown trends in data. It explores correlations between samples to help remove the signal out of a noise variable. PCA was used to assign weight to each of the 8 procedural categories based on the linear combination of all the variables. The weight was generated based on the variables from the 10 years of data and its correlation to the national average of ophthalmology residents. This is a better approach because it allowed us to circumvent the biasness of arbitrarily assigning weights to each surgical category. Although arbitrarily assigning weights to each category could have been an option, PCA helped generate a “fair” weight through a mathematical procedure which reduced the collinearity between the measures, thus giving us a pure weight which could be applied to each category (Table 2). Based on the weights, we calculated each resident’s overall procedures performed in each respective category and obtained the sum of each category to give us a total number (Tables 3 and 4). In addition, PCA also revealed the correlation between the data points and gave a P value of < .0001 leading us to reject the null hypothesis. Thus, we deduced that the resident in each class of residents with the highest weighted total would be the chief resident.
Baseline weight per category as generated by principal component analysis using 10 years of data from the ACGME data website national averages for each category (P < 0.0001).

Total number of procedures performed by each VCU resident: Also included is the national resident average (NRA) for each year.

Weighted procedures performed by each VCU Ophthalmology resident and National Resident average for each year of data collected in each respective category.

Results
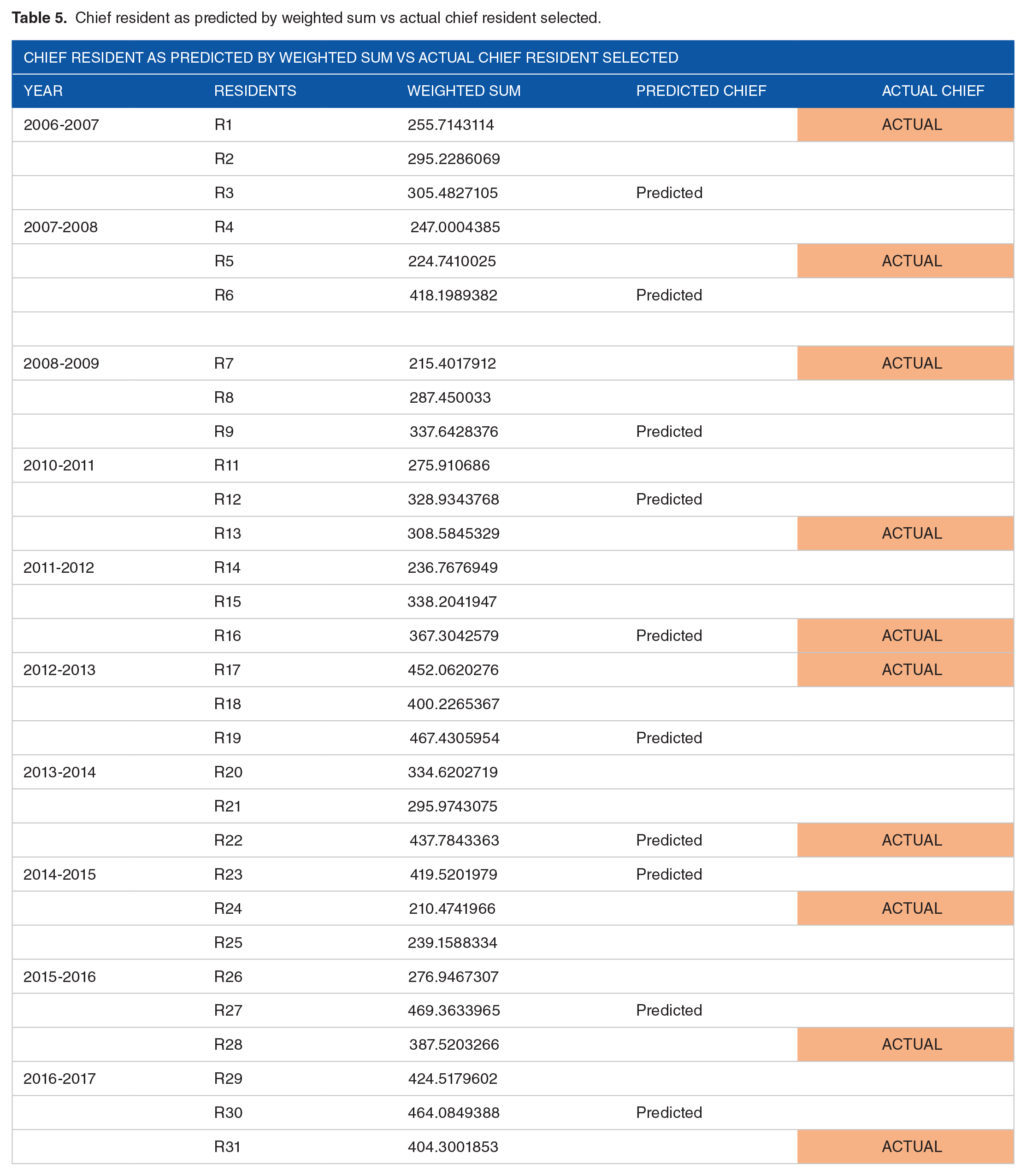
In all of the years reviewed, there were 3 ophthalmology residents in each class except 2009-2010 when there was only 1 VCUHS ophthalmology resident and therefore no chief resident was selected. Interestingly, the resident with the highest weighted total each year was not selected as chief resident. In other words, there seems to be no correlation between being selected as the VCUHS ophthalmology chief resident and the total volume of procedures performed (Table 5). When reviewing the total procedures performed in each respective category, this finding held true (Table 4). The only 2 years in which we correctly predicted the chief resident, 2011-2012 and 2013-2014, those residents logged the most total procedures compared with their 2 colleagues in different categories. The 2011-2012 chief had more cataracts, lasers, oculoplastics, and globe traumas compared with their colleagues versus the 2013-2014 chief who logged the most total procedures compared with their 2 colleagues in all categories except cornea and globes. These academic years, 2011-2012 and 2013-2014, are also the 2 years when the chief had the most categories among total cases performed, with the highest weighted values. When taking into account total cases logged as surgeon versus assistant, the 2011-2012 chief resident logged the most procedures as surgeon.
Chief resident as predicted by weighted sum vs actual chief resident selected.
There seemed to be a stronger correlation when considering those cases logged as surgeon only. This was particularly true within the cataract category. The most commonly ascribed surgery to the field of ophthalmology is cataract surgery. Currently, cataract surgery is the category of surgery set by the ACGME with the highest minimum number as surgeon to achieve for graduation from residency. The authors therefore believe it is paramount to review this category for secondary analysis. For 6 of the 10 years analyzed, the same chief resident was correctly predicted when comparing with the weighted value of cataracts performed as surgeon only (Table 6). This finding suggests there may be a correlation between the number of cataract cases performed as surgeon and selection as the chief resident.
Chief resident as predicted by the weighted total cataracts performed as surgeon only vs actual chief selected.

Chiefs as predicted by the total cataract surgery performed and the actual chief resident selected by VCU department of Ophthalmology.
In 5 of the 10 years analyzed, the VCUHS ophthalmology program average of total cases performed was below the national average for those respective years but this was not statistically significant (P = 0.35) (Figure 1).

Average procedures performed by VCU ophthalmology residents as compared with the national resident average (P = 0.35).
Discussion
Ophthalmology is a surgical sub-specialty requiring many attributes and abilities not unlike other surgical subspecialties. The critical desiderata required to become a competent, compassionate, successful ophthalmic surgeon are developed over the surgeon’s career and begins in residency. Each year within ophthalmology residency programs across the nation, there seems to be one resident setting themselves apart from their peers. Qualifying attributes used to determine chief resident and recognized by a candidate’s peers, program directors, chairs, other attending physicians, and others remarking on their performance remain imprecise. Such an important honor and responsibility should not only be awarded based on biased attributes but also on unbiased data. Although our research did not uncover these data, it did highlight that surgical volume may not be a paramount factor in the selection process of an ophthalmology chief resident.
There are limitations of this study and other circumstances to consider when determining why surgical volume proved to not correlate with selection as chief resident. One major consideration is the ACGME data are based on resident-logged cases and therefore it is the sole responsibility of the resident for logging cases. It should also be taken into consideration that the attending physician will vary the level of autonomy and participation depending on what point in time during their residency tenure a resident completes a specific rotation. This may help to promote anchoring bias when the time comes to select a chief resident. 12 It would be interesting to perform the same analysis on other programs of varying class sizes and surgical volume to investigate if our conclusions would remain. It would likewise be interesting to survey current ophthalmology professors of all levels affiliated with an academic health system to not only better understand their perception of the importance of surgical volume in the selection of a chief resident but other components that are or should be considered.
Footnotes
Acknowledgements
The authors thank Mrs. Brenda Ayala, VCUHS ophthalmology residency coordinator, for masking the authors to the identity of the participants and Mr. Rexford Anson-Dwamena, MPH, for statistical analysis without whom the study would not have been completed.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
NQR wrote a portion of the abstract, purpose, methods, results, and discussion sections. RKO wrote a portion of the methods, results, and discussion sections as well as performed the majority of the data calculations.