
Abstract
Purpose:
To assess the satisfaction and competency of Saudi ophthalmology residents and compare their performance against International Council of Ophthalmology (ICO) standards.
Methods:
A cross-sectional web-based survey of senior ophthalmology residents (postgraduate years [PGY] 3-4) and recent graduates (from 2010 to 2015) assessed various aspects of training. The questionnaire was sent to the participants and was divided into 3 main domains: demographics, training program evaluation, and preparedness for board exams and clinical practice.
Results:
Out of the 145 invitees, 120 (82.8%) responded. Fifty percent of respondents reported an overall satisfaction with the program. Adequate clinical exposure was reported in most subspecialties except refraction and low vision rehabilitation with inadequate exposure reported by 55.8% and 95.8%, respectively. Surgical exposure was reported as adequate for phacoemulsification (58.3%) and strabismus surgery (68.3%) only. Eighty-nine percent of respondents reported performing less than 80 cases of phacoemulsification. Of the respondents who had graduated, most (89.7%) passed the final board exam at the first attempt. There were 73.5% of respondents who reported that residency training prepared them well for the board exam. Ongoing clinical and call duties were reported as having a negative impact on exam performance.
Conclusions:
Saudi ophthalmology residents demonstrate a high level of clinical competency. However, additional efforts should aim at improving surgical training to increase the level of satisfaction among residents and improve the quality of training to meet international standards.
Introduction
The Saudi ophthalmology residency training program was established in 1984, following a recommendation from a nationwide survey investigating the causes of blindness in Saudi Arabia. 1 At this time, the lack of trained ophthalmologists was identified as a major contributor to blindness in Saudi Arabia. Currently, the residency training program spans over 5 geographic regions within Saudi Arabia and accepts around 50 trainees every year.
The Saudi ophthalmology residency is a 4-year program that is structured to ensure adequate clinical and surgical exposure for trainees to become competent general ophthalmologists. The training curriculum is divided into monthly rotations in different subspecialties. Basic ophthalmic surgical skills are taught during the first year of training, and the surgical experience of a resident is built with time aiming to meet objectives specified according to the year of training. By the end of the second year of training, residents would have completed rotations in all ophthalmic subspecialties, and during the last 2 years of training, they repeat the same rotations aiming to further advance their skills in these subspecialties especially in the surgical aspect. Residency training is currently under the supervision of the Saudi Commission for Health Specialties (SCFHS), a regulatory body that manages admission, continuous evaluation, and certification of trained residents.
The International Council of Ophthalmology (ICO) published a detailed statement 2 defining competencies that should be included in any postgraduate ophthalmic training curriculum. This document outlines essential cognitive and technical skills required in every subspecialty, as well as generic competencies such as patient care, professionalism, and communication skills. This report allowed residency programs worldwide to evaluate their performance against international standards.3,4
To date, the Saudi ophthalmology training program has not been objectively evaluated. In addition, the Saudi ophthalmology residency program has not been compared with other international programs. Therefore, the objective of this study was to evaluate the satisfaction and competency of Saudi ophthalmology residents, and to compare the performance of Saudi residents with the ICO standards.
Subjects and Methods
This cross-sectional study was performed from February to December 2016. The study protocol was approved by the Institutional Review Board at King Saud University. Email invitations were sent to senior ophthalmology residents in postgraduate years (PGY) 3 and 4, as well as recent graduates (from 2010 to 2015), to participate in an online survey. Data collection was carried out in 2 phases: during the first phase (February-July 2016), the survey was sent out to graduated residents, and the second phase (July-December 2016) was used to collect data from current residents, coinciding with the end of the residency academic year in Saudi Arabia. The questionnaire was divided into 3 main segments: demographics, evaluation of the training program, and preparedness of graduates for board exams and clinical practice.
Data were collected electronically and stored in a spreadsheet. In this study, categorical variables are reported as frequencies and percentages, and continuous variables as mean ± standard deviation (SD). Figures were created with data visualization software (Tableau Software, Seattle, WA, USA).
Results
Out of the 145 invitees, 120 participated in the survey (82.8% response rate). The average age of the participants was 30.4 years, 69% were men, and 48% were trained in Riyadh. Senior residents comprised 43.3% of participants and the remainder (56.6%) were recent graduates. Table 1 presents the demographics of the survey respondents.
Demographics of the survey respondents (n = 120).

Abbreviations: PGY, postgraduate years.
The satisfaction level with residency training is presented in Table 2.
Level of satisfaction among survey respondents (n = 120).
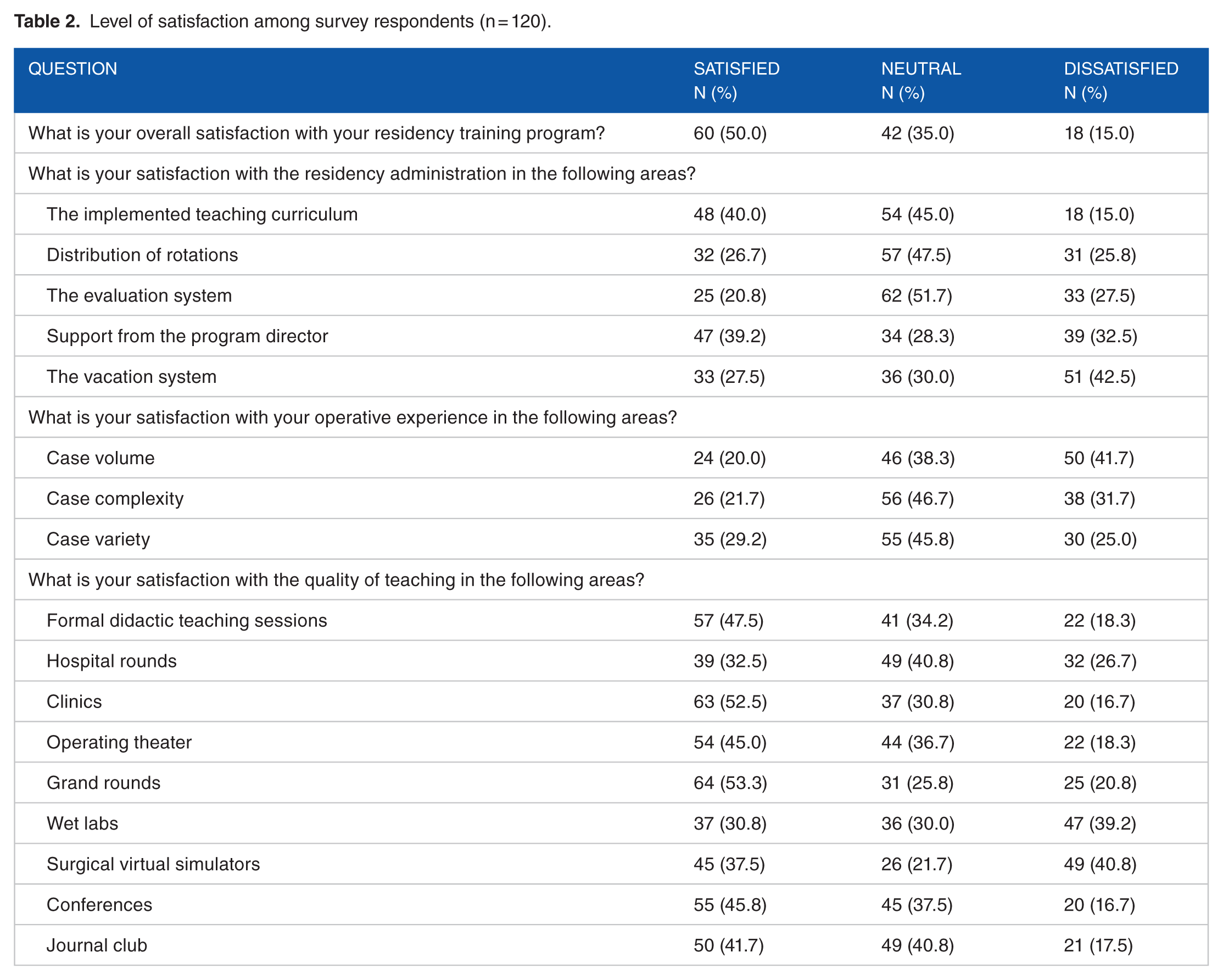
In terms of overall satisfaction, 50% were satisfied with their training program. Administrative domains that yielded a low rate of satisfaction were evaluation (20.8%), distribution on rotations (26.7%), and the vacation system (27.5%). For surgical experience, less than a third of respondents were satisfied with the case volume, complexity, and variety. More than a third of respondents were dissatisfied with the quality of teaching in wet labs (39.2%) and on surgical simulators (40.8%).
More than half of the respondents reported adequate clinical exposure in most subspecialties (Figure 1).

Reported adequacy of clinical exposure among survey respondents (n = 120).
However, inadequate exposure was reported for refraction (55.8%) and low vision rehabilitation (95.8%). Most respondents reported inadequate surgical exposure in most procedures (Figure 2).
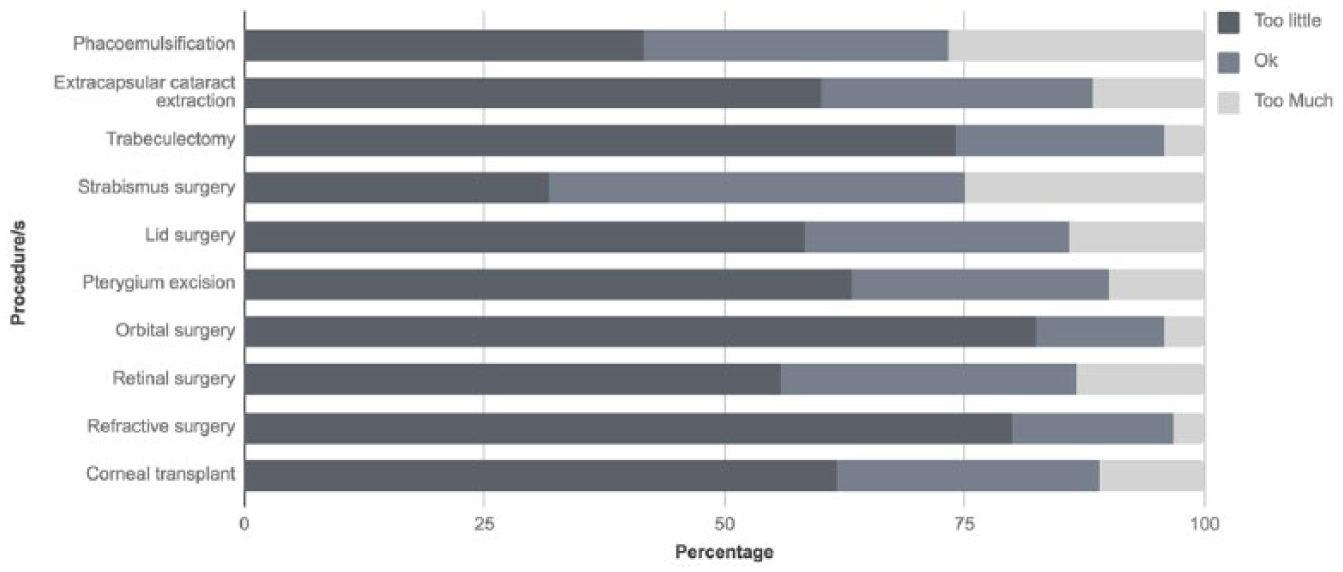
Reported adequacy of surgical exposure among survey respondents (n = 120).
The only 2 procedures that were reported as adequate by more than half of the respondents were phacoemulsification and strabismus surgery (58.3% and 68.3%, respectively).
The vast majority of respondents (89.2%) performed less than 80 cases of phacoemulsification. Less than a third of respondents reached more than 15 cases of either extracapsular cataract extraction, trabeculectomy, or strabismus surgery. Table 3 presents the surgical volumes achieved by the survey respondents.
Reported surgical volume achieved by survey respondents (n = 120).

Table 4 presents the reported competency in achieving ICO learning objectives.
Reported competency in achieving ICO learning objectives for ophthalmology residency graduates (n = 120).
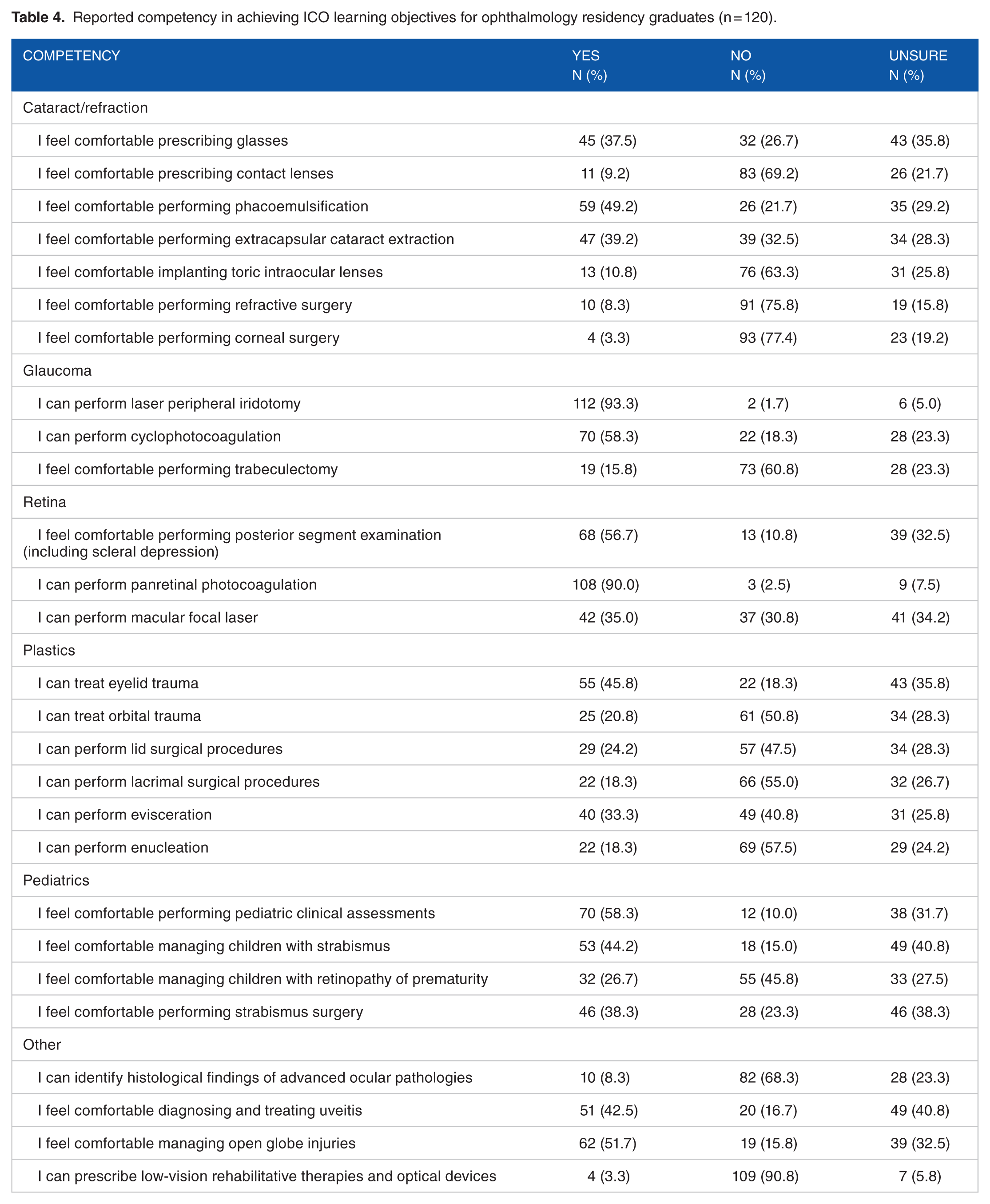
In the cataract and refraction domain, around one-third of the respondents (37.5%) feel comfortable prescribing glasses and about one half (49.2%) were comfortable performing phacoemulsification. Most (75.8%) respondents did not feel comfortable performing refractive surgery. For glaucoma, most could perform laser procedures such as peripheral iridotomy and cyclophotocoagulation (93.3% and 58.3%, respectively); however, only a few (15.8%) feel comfortable performing trabeculectomy. Ninety percent of respondents felt comfortable performing panretinal photocoagulation. Thirty-five percent were comfortable with performing focal macular laser treatments. An overall reduced level of competency (ranging from 18.3% to 33.3%) was noted in most of plastics learning objectives, with the exception of eyelid trauma for which 45.8% of respondents felt competent. For pediatric ophthalmology, 58.3% of respondents felt competent in performing a clinical assessment of a pediatric patient, and only 38.3% were comfortable performing strabismus surgery.
Conducting research was a mandatory component of residency training in most responses (70.8%). Furthermore, most respondents (75%) published at least one paper during their training. A summary of research experience during residency among respondents is shown in Table 5.
Research experience during residency among survey respondents (n = 120).

Respondents were also asked about their satisfaction with non-clinical aspects of training (Figure 3).

Reported satisfaction with training in non-clinical skills among survey respondents (n = 120).
Ethics, professionalism, and relationship with peers and other health care professionals were skewed toward satisfaction. A skew toward dissatisfaction was noted in staffing, administration skills, information management, and technology.
Graduates were asked additional questions about their experience with the final board exam (Table 6).
Preparedness for the final board exam among graduated respondents (n = 68).

Most (89.7%) passed the examination after the first attempt, while 4.4% passed following multiple attempts, and 5.9% did not pass at all. Most graduates (73.5%) felt that their training prepared them for the examination; however, only 57.3% had protected study time prior to their examination. Furthermore, more than two-thirds of the respondents reported that continuing clinical and call duties while studying negatively affected their performance.
Discussion
The SCFHS recently underwent a major transformation in which the number of residency training positions offered annually were increased to accommodate the growing number of graduate medical students. 5 Conducting our survey at this point in time, in particular, was essential to benchmark the performance of current ophthalmology training programs and ensure that expanding the number of positions does not negatively affect training quality.
Fifty percent of respondents reported overall satisfaction with the residency program and an additional 35% gave a neutral response. This level of satisfaction is higher than other ophthalmology residencies in the region. For example, the overall satisfaction among ophthalmology residents was 34% in Jordan 3 and 36% in Iran. 6 However, the overall satisfaction in the current study is low compared with well-recognized international training programs in the United States 7 (93%) and Canada 4 (85%).
An acceptable rate of satisfaction was reported with the main domains of clinical teaching such as attending clinics, formal teaching sessions, and grand rounds. However, respondents were dissatisfied with most areas of surgical training, particularly wet labs and surgical simulators. These findings reflect the fact that some training programs in Saudi Arabia still lack well-established wet labs as well as simulators required for surgical training. Previous reports have suggested that wet labs and virtual simulators are associated with improved perceived surgical competency among residents. 8 Hence, to ensure appropriate surgical training, these elements should be included in any future training program in the Kingdom.
Inadequate clinical exposure was mainly reported in 2 areas: refraction and low vision rehabilitation. This finding is attributed to the fact that these services are usually provided by optometrists rather than ophthalmologists at the training centers. Spectacle and contact lenses prescription is an ICO learning objective for ophthalmologists. 2 In addition, the growing burden of blindness from age-related eye diseases in Saudi Arabia9–11 portents a considerable demand for treating the visually impaired. Therefore, we recommend that training programs enhance efforts to ensure that residents are well-trained in refraction, spectacle and contact lens correction, and low vision rehabilitation.
In this study, surgical exposure was reported as inadequate for most procedures. This outcome may be less significant as surgical training is usually achieved at a fellowship level (ie, orbital surgery, retinal surgery, and corneal transplant). However, it is alarming that respondents noted inadequate exposure to routine procedures performed by a general ophthalmologist such as extra-capsular cataract extraction, trabeculectomy, and pterygium excision. Low exposure to refractive surgery has been reported in training programs worldwide.4,12 In Saudi Arabia, the contributing factor is that refractive surgery is performed at private clinics and not in training centers. However, refractive surgery is a significant component of many general ophthalmology practices and warrants greater exposure during residency.
The SCFHS has set a required minimum number for each surgical procedure at the time of graduation. 5 For example, a resident is expected to have performed a minimum of 80 phacoemulsification cases on graduation. Comparing the results of our survey against these requirements indicated that most respondents failed to achieve the required numbers. Using the example above, our results show that only 10% of respondents performed 80 or more phacoemulsification cases. We found similar results for other procedures such as extra-capsular cataract extraction, trabeculectomy, strabismus surgery, and primary repair. However, 43% of respondents are still in training at the time of the survey, thus they still have time to complete the surgical requirements.
Our study has some limitations. First, a lot of subjective indicators were used (ie, satisfaction, adequacy, competency). Although these measures somewhat reflect the quality of training, they do not provide an objective assessment. Second, given that the data were collected through a survey, the information reported from respondents is subject to recall bias. In addition, 43.3% of respondents are still in training (PGY 3-4). Hence, with their progression in training to latter stages, their perception of the program and their preparedness may change.
It was crucial to assess the competency of achieving ICO learning objectives (Table 4) as this provides, for the first time, an insight into how Saudi residents are performing against international standards. However, from a local perspective, it is important that trainees are competent in managing the most prevalent ocular disorders in the Kingdom. A rapid assessment of avoidable blindness survey in Saudi Arabia 13 reported that the 2 major causes of avoidable blindness are cataract and diabetic retinopathy. Therefore, the main focus in Saudi Arabia should be to ensure that graduating ophthalmologists are competent in performing cataract surgery and treating diabetic retinopathy.
In summary, this study sets a benchmark for comparison to future changes in ophthalmology training in Saudi Arabia. Currently, Saudi ophthalmology residents have a high level of clinical competency. Nonetheless, more efforts should be directed toward surgical training to increase the level of satisfaction among residents and improve the quality of training to meet international standards.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All the authors made substantial contributions to drafting, revising, and approving the final version of the manuscript.