
Abstract
Introduction:
As providers of a large portion of the care delivered at academic health centers, medical trainees have a unique perspective on medical error. Despite data suggesting that errors in physical examination (PE) can lead to adverse patient events, we are not aware of previous studies exploring medical trainee perceptions of the relationship between patient harm and inadequate PE. We investigated whether first-year residents at a large tertiary care academic medical center perceive inadequate PE as a cause of adverse patient events.
Methods:
As part of a larger survey given to incoming interns at Thomas Jefferson University Hospital orientation (2014-2018), the authors examined the perceptions of inadequate PE and adverse patient events. We also examined other details related to PE educational experiences and self-reported PE proficiency. The survey was developed a priori by the authors and assessed for face validity by expert faculty.
Results:
Ninety-eight percent of respondents (695/706) reported that inadequate PE leads to adverse patient events. Seventy percent (492/706) believe that inadequate PE causes adverse events in up to 10% of all patient encounters, and 30% (214/706) reported that inadequate PE causes adverse events in greater than 10% of patient encounters. Forty-five percent of surveyed interns (319/715) had witnessed a patient safety issue as a result of an inadequate PE. Only 2% of surveyed interns (11/706) did not think patients experience adverse events because of inadequate PEs. Ninety percent of surveyed interns (643/712) reported feeling proficient in performing PE. From 2015 to 2018, 80% (486/604) indicated that they received “just enough” PE education.
Conclusion:
Nearly all incoming interns surveyed at our institution believe that inadequate PE leads to adverse patient events, and 45% have witnessed an adverse patient event due to inadequate PE. We urge clinicians, educators, and health care administrators to consider enhanced PE skills training as an important and viable approach to medical error reduction, and as such, we propose a 5-pronged intervention for improvement, including a redesign of PE curricula, development of checklist-based assessment methods, ongoing skills training and assessment of physicians-in-practice, rigorous study of PE maneuvers, and research into whether enhanced PE skills improve patient outcomes.
Introduction
As providers of a large portion of the care delivered at academic health centers, medical trainees have a unique perspective on medical error. In one study, over half of the residents surveyed had cared for a patient with an adverse event. 1 Residents have identified excessive work hours, insufficient supervision, and inadequate hand-offs as common causes of patient harm.1,2 Despite data suggesting that errors in physical examination (PE) can lead to adverse patient events, we are not aware of previous studies exploring medical trainee perceptions of the relationship between patient harm and inadequate PE.
An evolving body of literature has linked PE error with patient harm. When Verghese et al 3 surveyed physicians about the causes of PE errors, 63% reported that an appropriate PE was not performed, 14% reported a PE finding was misinterpreted, and 11% said that the relevant sign was missed or not sought. These mistakes were felt to have caused misdiagnosis, diagnostic delays, and treatment errors. 3 In a chart review of patients admitted to a major urban hospital, 26% of patients had a pivotal PE finding that was initially missed or misinterpreted, resulting in a delay of appropriate diagnosis and management. 4 Wray and Friedland 5 reported that a PE error occurred in nearly two-thirds of hospitalized patients examined by residents. In addition, closed malpractice claims of serious errors in both the emergency department and ambulatory setting showed that failure to perform an adequate PE occurred in 20% of claims.6,7
Given the data linking PE errors to patient harm, we investigated whether first-year residents at a large tertiary care academic medical center perceive inadequate PE as a cause of adverse patient events.
Methods
As part of a larger survey given to all incoming interns at Thomas Jefferson University Hospital (TJUH) from 2014 to 2018, the authors examined the perceptions of inadequate PE and adverse patient events. We also examined other details related to PE educational experiences and self-reported PE proficiency. This survey was completed during intern orientation.
Survey
In 2014, a 32-item survey about prior PE skills training, experience, and perceptions was developed a priori by 2 of the authors (L.A.R. and D.B.). Faculty members then independently reviewed the survey for face validity. In 2015, 7 additional items pertaining to PE were added. In 2016, 4 additional items pertaining to PE were added and 3 items were deleted. From 2016 to 2018, the survey contained 40 items. The paper survey was distributed individually to incoming interns during a clinical skills orientation session during orientation week, prior to clinical work. The survey was collected by personnel running the session who were not associated with the analysis.
Analysis
Data were manually entered into the statistical database. Descriptive analyses were conducted using SPSS (version 25) statistical software. We used the χ2 test for categorical questions, with an α of 0.05 for significance. The Institutional Review Board (IRB) at Thomas Jefferson University (TJU) reviewed this study and granted IRB exemption.
Results
We administered the survey to 733 incoming interns representing all residency programs present at intern orientation at TJUH: 117 in 2014, 152 in 2015, 158 in 2016, 166 in 2017, and 142 in 2018. Response rate was 74% (117/159) in 2014, 96% in 2015 (152/159), 94% in 2016 (158/168), 74% in 2017 (166/225), and 93% (142/152) in 2018. Sizes of interns at orientation each year varied due to changes in program size and inclusion of various satellite sites or programs in various years. Interns came from 5 geographic regions, with most being from the northeastern United States (Table 1); 21% attended medical school at the Sidney Kimmel Medical College of TJU.
Geographic regions of the United States of the medical school attended by incoming interns surveyed at Thomas Jefferson University.

n = 114.
n = 139.
n = 154.
n = 166.
n = 141.
Ninety-eight percent (695/706) of interns reported that they believe patients experience adverse events due to inadequate PEs (Table 2). Sixty-eight percent of interns (481/706) believed that inadequate PE causes adverse events in up to 10% of all patient encounters, and 30% (214/706) believed that inadequate PE causes adverse events in greater than 10% of patient encounters. Forty-five percent (319/715) of interns reported that they had witnessed a patient safety issue as a result of an inadequate PE. This proportion did not significantly vary by survey year (P = .078 from the Cochran-Armitage χ2 test for trend).
Incoming interns’ reported medical school experience with physical examination skills education, experience, and perceptions survey.

Abbreviation: PE, physical examination.
Sample range is 85 to 117.
Sample range is 141 to 152.
Sample range is 150 to 158.
Sample range is 114 to 166.
Sample range is 104 to 142.
Sample range is 587 to 733 for questions that appear all 4 years.
Sidney Kimmel Medical College is the medical school associated with Thomas Jefferson University Hospital, the hospital where the survey was administered.
Ninety percent of interns (643/712) reported feeling proficient in performing the PE. From 2015 to 2018, 83% (501/604) indicated that they received “just enough” PE education. In the first 3 years of medical school, more than 75% of medical students reported more than 5 hours of PE skills training. Forty-nine percent of students (348/717) reported 5 hours or less of PE skills training during their fourth year of medical school. Ninety-one percent (647/711) reported being taught PE skills using a standardized PE checklist. Sixteen percent indicated that they had attended an advanced physical diagnosis course during their third or fourth year. Physical examination training was provided by faculty, residents, standardized patients, upper-level medical students, and nonphysician health care professionals (Table 3).
Who taught incoming interns physical examination skills by year in school, 2014-2018.
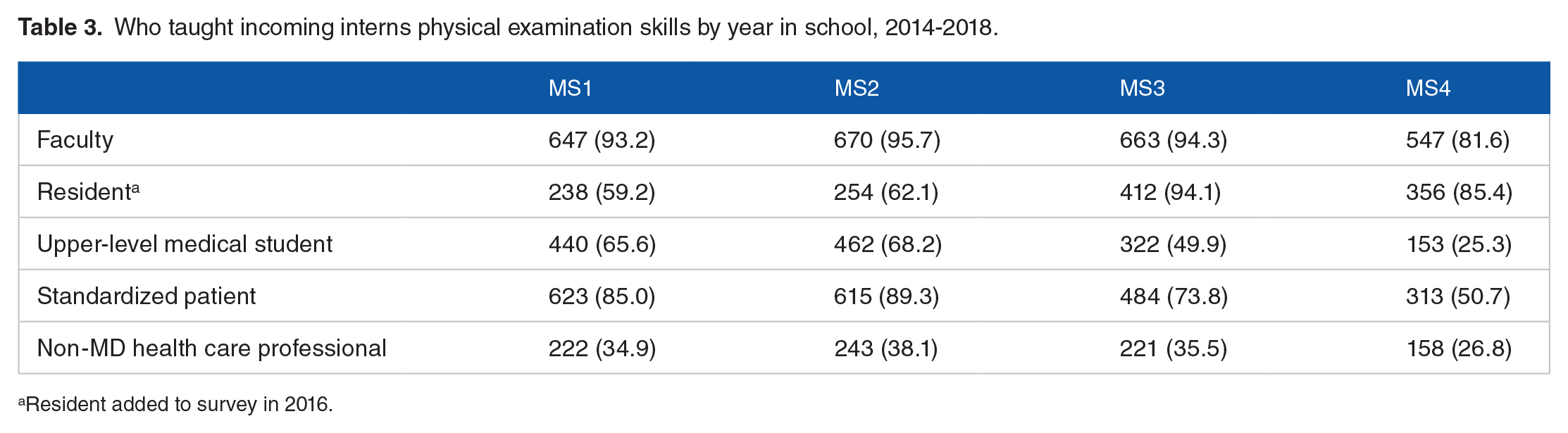
Resident added to survey in 2016.
Discussion
Our survey results demonstrate that medical trainees recognize errors in PE as a cause of patient harm. Ninety-eight percent of interns (695/706) believe inadequate PE causes adverse patient events. Thirty percent believe that inadequate PE causes adverse patient events in more than 10% of all patient encounters. Forty-five percent of all interns (319/715) reported that they had witnessed a patient safety issue as a result of an inadequate PE. Our findings suggest that incoming interns identify inadequate PE as a frequent cause of adverse patient events.
Inadequate PE can include not performing an appropriate PE, misinterpreting a PE finding, missing a relevant sign, and not understanding how to apply the gathered information to the clinical scenario. Physical examination errors may occur for several reasons, but inadequate skill development is likely an important contributor. Suboptimal PE skills of medical trainees have been documented across subspecialties, including dermatology, ophthalmology, cardiology, pulmonology, and musculoskeletal examination.8–12 Berg et al 13 found that fourth-year medical students could correctly identify only 39% of “classic” PE findings. On assessment in the United States Medical Licensing Exam (USMLE) Step 2 Clinical Skills exam, medical students score 20 points lower on the PE component than the history component (59.6% vs 78.1%). 14 Deficits in PE skills seem to persist in graduate medical education. Incoming interns scored just over 50% on assessments of PE knowledge, including a written test and performance on real patient objective structured clinical exams (OSCEs). 15 In a separate study, after just 1 month of internship, Postgraduate Year (PGY) 1 residents performed as well as PGY3 residents on OSCEs developed to assess PE skills, suggesting that little PE learning may happen beyond the first month of internship. 16
Notwithstanding the above data, medical trainees in our study and others self-report a high degree of proficiency in PE skills and view their PE education as sufficient. 17 Multiple studies have shown a mismatch between medical trainee confidence and competence levels. Data suggest that trainees overestimate their clinical skills, including communication, PE, procedural, and management skills.18–22 In addition, while medical trainees may know how to perform the PE, they may struggle with application of this knowledge to clinical decision making. 23
Recent publications have explored how and when PE teaching occurs in medical school. There is wide variation in how PE is taught, and optimal strategies for PE instruction remain unclear.24,25
Our study shows that almost half of the surveyed interns reported receiving less than 5 hours of PE training in the fourth year of medical school, raising the possibility that incompletely developed skills or attrition of skills may be present.
We believe that the link between inadequate PE and patient harm adds an urgency for medical educators to determine how and when to best teach PE with the goal of optimizing patient well-being. We agree with Clark et al 26 that a renewed emphasis on the PE is a potentially powerful and underexplored strategy to reduce medical error. We urge clinicians and educators to consider enhanced PE skills training as an important and viable approach to medical error reduction, and as such, we propose a 5-pronged intervention for improvement (Figure 1). (1) Redesign PE curricula: PE education should be iterative and longitudinal across levels of training, checklist-based, and allow ample opportunity for deliberate practice. After basic PE skills training in the preclinical years, advanced skills sessions should include best practice techniques and continued supervised practice. (2) Develop checklist-based assessment methods: Appraisal of PE skills requires checklist-based assessment tools. Importantly, formative assessment tools should complement the overall teaching strategy by providing students specific training needs. Summative assessments, using the same checklists used in PE teaching curricula, then allow for credible statements of competence in this skill domain. (3) Provide ongoing PE skills training and assessment of physicians-in-practice: The first 2 recommendations rely on having trained faculty to teach, interpret, and apply both the basic and advanced PE to clinical decision making. Ongoing training and competency assessment are needed to do this. Continuing education requirements should include PE education and, importantly, hands-on training. Recertification efforts should include continuing education/training and assessment of PE skills. (4) Design rigorous prospective studies of PE maneuvers: A set of new data is needed to help determine which PE maneuvers are most effective. Current efforts, including JAMA’s well-respected Rational Clinical Examination 27 series, provide a springboard for this much-needed future research. (5) Investigate whether improved PE skills improve patient outcomes. This final prong remains a critically important question and requires further study.

Five-pronged Framework for improving physical examination training.
Limitations
Despite the strengths of this study, there are several limitations. Recall bias can affect survey responses, and hence responses may not correlate with actual experience. This analysis was completed in a single institution, and therefore, the results may not be generalizable to a national intern population. However, our survey represented students from throughout the United States, multiple specialties, and equal distribution of sex.
Conclusion
Nearly all incoming interns surveyed at our institution believe that inadequate PE leads to adverse patient events, and 45% have witnessed an adverse patient event due to inadequate PE.
Future research is needed to further elucidate how PE errors lead to patient harm and whether advanced PE education can improve patient safety. We urge clinicians and educators to consider enhanced PE skills training as an important and viable approach to medical error reduction.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
KB, DB, LR, SR planned the survey and developed the survey questions. LC assisted with data collection and input. RD and CM performed the statistical analyses. SR, KB, DB, LR, JD, RD, CM contributed to the interpretation of the results. SR took the lead in writing the manuscript. All authors provided critical feedback and helped shape the research, analysis and manuscript.
Ethical Approval
This survey study was determined to be exempt by the Thomas Jefferson University Office of Human Research. Original IRB application: Exempt status 1/13/2010; reference # 09E.306; Amendment: Exempt status 3/18/19; reference # 09E.306.
Previous Presentations
S. Russo, D. Berg, J. Davis, R. Davis, L. Riesenberg, K. Berg. Intern Perceptions of Physical Exam Errors. Poster presented at: Directors of Clinical Skills Courses (DOCS) Annual Meeting; November 3, 2017, Boston, MA.