
Abstract
“I am not young enough to know everything.”
Background:
There is insufficient knowledge among providers and patients/caregivers of ionizing radiation exposure from medical imaging examinations. This study used a brief, interactive educational intervention targeting the topics of best imaging practices and radiation safety early in health professions students’ training. The authors hypothesized that public health, medical, and physician assistant students who receive early education for imaging appropriateness and radiation safety will undergo a change in attitude and have increased awareness and knowledge of these topics.
Materials and methods:
The authors conducted a 1.5-hour interactive educational intervention focusing on medical imaging utilization and radiation safety. Students were presented with a pre/postquestionnaire and data were analyzed using t tests and multivariate analysis of variance.
Results:
A total of 301 students were enrolled in the study. There was 58% (P < .01) and 85% (P < .01) improvement in attitude and knowledge regarding appropriateness of imaging, respectively. The authors also found an 8% increase (P < .01) in students who thought informed consent should be obtained prior to pediatric computed tomographic imaging. Physical assistant students were more likely than medical students to prefer obtaining informed consent at baseline (P = .03).
Conclusions:
A brief educational session provided to health professions students early in their education showed an increased awareness and knowledge of the utility, limitations, and risks associated with medical imaging. Incorporation of a best imagining practice educational session early during medical education may promote more thoughtful imaging decisions for future medical providers.
Introduction
Over the past 3 decades, high-tech medical imaging has influenced patient care through its transformative capabilities for rapid diagnoses, close monitoring, and management of many conditions. Lately, however, it has become equally as concerning for its overutilization.1–3 Studies suggest that up to 20% to 50% of high-technology imaging such as multisection computed tomography (CT), magnetic resonance imaging, and positron emission tomography fail to provide information that improves patient care and hence may represent unnecessary imaging services.1,4 Such high-intensity practice patterns run at cross-purposes with ensuring high-quality care of patients, all the while exposing patients to unnecessary risks, most notably radiation-induced cancer. 5 Estimates show that approximately 29 000 future cancers could be related to CT use in the United States in 2007.6,7 Children are especially vulnerable to the harmful effects of radiation.7–12 Two recent epidemiologic analyses on large populations over many years have shown similar results: a 24% increase in cancer in children and adolescents exposed to ionizing radiation from CT scans.9,13,14
An overwhelming majority of both providers and patients/caregivers believe that communicating radiation risks before CT scans are important.15–20 Yet, knowledge regarding potential radiation-induced cancer risk from CT among both groups is poor.10,16,21–23 Most recent statistics show that 48% of physicians and 72% of trainee physicians are uncomfortable sharing radiation risk information with patients. 21 Most of the providers underestimate radiation doses of common radiologic examinations. 21 Furthermore, many providers’ display misconceptions regarding different imaging procedures, with up to 28% of clinicians unable to correctly identify which modalities expose patients to ionizing radiation.23,24 Most recent systematic literature reviews and historical comparisons spanning more than a decade demonstrate that this knowledge gap has not diminished significantly over time.16,21 Lack of an understanding of radiation risks jeopardizes effective risk/benefit discussions and undermines the decision process for ordering the CT.19,21 Studies show that sharing radiation risk information between providers and patients occurs seldomly (<25% cases).10,16,21,22,25,26 Despite the fact that radiation risk communication occurs rarely, there is evidence to suggest that risk-benefit dialogue with patients could be a valuable tool for decreasing unnecessary CT use in an acute care setting.27–30
A recent study revealed that most of the emergency department (ED) providers thought that the CT scans they ordered may have been unnecessary 25% to 50% of the time. 27 However, in this same study, the subset of providers who considered patients’ radiation dose history and conducted risk-benefit discussions before ordering a study were less likely to order unnecessary CT scans. 27 Studies stress that the provision of radiation safety information and appropriate understanding of radiation exposure will influence the number of advanced imaging studies requested by the provider. 31 Furthermore, parents are more willing to avoid radiation exposure from a CT scan for their child if the likelihood of a positive finding is low. 32
Educating our future health care professionals and imaging prescribers regarding appropriate imaging utilization to optimize quality and safety and minimize risk is crucial. Nonetheless, public health, advanced practice provider and medical students receive little or no exposure to imaging appropriateness principles and radiation safety practices.33–35 Our goal in the present project was to pilot a brief, interactive educational intervention, aimed at instilling an awareness of best imaging practices and radiation safety, early in health professions student training. We hypothesize that public health, physician assistant (PA), and medical students who receive early education on the major challenges of imaging appropriateness and radiation safety will undergo a change in attitude and will improve awareness and knowledge of these topics. In turn, these interventions may promote improved critical thinking and self-directed learning. 36
Methods
General study design
Our pilot study consisted of a single 1.5-hour interactive educational intervention for health profession students that included a PowerPoint presentation and a facilitated discussion (Table 1). Our primary objective was to test the initial feasibility of the intervention. The secondary objective was to compare results of the intervention by student type, specifically medical and PA students. The interactive session comprised the issues surrounding medical imaging overutilization and CT radiation safety. To evaluate the intervention, we presented students with a questionnaire (Appendix 1) to complete prior to the educational session and again directly following it. The UNC Biomedical IRB (institutional review board) determined this study to be exempt from IRB review under 45 CFR 46.101(b). To the best of our knowledge, this is the first quality improvement educational interactive session that addresses medical imaging overutilization and CT radiation safety targeting health professions students early in their training.
Topics covered during the educational session.

Study participants
The principal investigator (D.A.) presented the educational intervention to multiple cohorts of students within their health professions programs at 3 different academic institutions between 2014 and 2018. Specifically, we included public health graduate students, second year PA students, and medical students (ranging from first to fourth year) in our study, whom we selected through convenience sampling. The latter 2 groups included students who were on clinical rotations/electives. One institution invited the principal investigator (D.A.) to speak to the entire medical school class enrolled in their preclinical years (first and second) of medical school.
During their second year on clinical rotations, PA students intermittently return to campus as an entire class for scheduled didactic sessions. In contrast, medical students during their third and fourth year of required clinical rotations may select to participate in a radiology elective. For iterative cycles (annually and/or monthly) involving PA and medical student cohorts, respectively, the course directors invited the principal investigator (D.A.) for didactic lectures on the topic.
Educational session
Drawing from the most recent medical literature and lay press, we presented a balanced overview of imaging overuse, often cited statistical projections and direct epidemiologic data related to radiation-induced cancer risks from CTs, concerns surrounding health care-related harms, and health care costs. Moreover, we emphasized current literature underscoring effective provider/patient/caregiver interactions. The lecturer (D.A.) functioned mainly as a facilitator because students were encouraged to interject with their own personal experiences, interpretations, and lines of questioning. The educational session included 2 interactive student-based case presentations: (1) the Ottawa Ankle Rules 39 : teenage baseball player with minor ankle injury and (2) validated clinical prediction rules for children at very low risk of clinically important traumatic brain injury (ciTBI) 40 : toddler with minor head injury.
Survey instrument
The questionnaire (Appendix 1) consisted of a total of 7 questions grouped into 3 categories—attitude, knowledge, and opinions toward informed consent. We also collected written comments during the posttest about the presentation from students that wished to provide them. Following data collection from each session, we coded survey data and compiled them into an Excel spreadsheet for analyses. The data analyst (T.H.) rereviewed data at a later date to ensure accuracy of coding. We scored attitude questions (questions 1 and 2) on a scale from 0 to 4, where 0 represented “not at all important” and 4 represented “very important.” To rate knowledge questions (questions 3, 4, 6, and 7), we used a score of 0 or 1 for incorrect and correct answers, respectively. For students who failed to answer a knowledge question, we used a score of 0. For question 5, which asked students whether informed consent should be obtained prior to a pediatric CT examination, we used a score of 0 and 1 for “no” and “yes,” respectively. At the conclusion of all survey collection, we compiled selected student comments and grouped them into 3 categories—previous experiences, current reactions, and future practice changes.
Evaluation
We defined feasibility as successfully conducting the intervention involving each student type and an overall increase in knowledge after the intervention. Our statistical analyses of survey results used SAS 9.4 (SAS Institute Inc., Cary, NC, USA). First, we assessed all data for normality using a Shapiro-Wilk test. Once data were confirmed to be normally distributed, we compared variables using t tests and included all students in the overall analysis and the analysis by sex. However, to compare the results of medical students and PA students, we excluded public health graduate students because PA and medical students will eventually be involved in the decision-making process and prescribing imaging studies, whereas public health graduate students per se will not generally be involved in direct patient care. Finally, we employed a χ 2 test and a multivariate analysis of variance (MANOVA) to test for an association and any interactions between sex and student type. Statistical significance was defined as P < .05.
Results
Cohort characteristics
Our sample included 301 students. An additional 5 students and 1 nonstudent physician also completed the pretest but did not complete the posttest. These individuals were excluded from all analyses and not included in the total. Of these, 204 (67.8%) were women and 96 (31.9%) were men. One student did not report sex. A total of 11 (3.6%) were public health graduate students, 142 (47.2%) were PA students, and 148 (49.2%) were medical students. Medical students were pursuing postgraduate residency training in Emergency Medicine, Family Medicine, Internal Medicine, Pediatrics, Surgery, Radiology, Radiation Oncology, Anesthesiology, Neurology, Obstetrics and Gynecology, Ophthalmology, and Geriatrics. The PA students were pursuing practice opportunities in Family Medicine, Surgery, Emergency Medicine, Gastroenterology, Internal Medicine, Orthopedics, Cardiology, Behavioral Medicine, Pediatrics, and Critical Care.
Study feasibility
We successfully completed 15 invited sessions. Of these sessions, we conducted 1, 10, and 4 with public health, medical, and PA students, respectively. Lively in-session questions, responses, and discussions served to promote students’ critical thinking and to motivate self-directed learning (Tables 1 and 4). Course directors were grateful for the new experience, pleased with the success of the session, and requested the session be repeated over a 4-year period.
Survey results
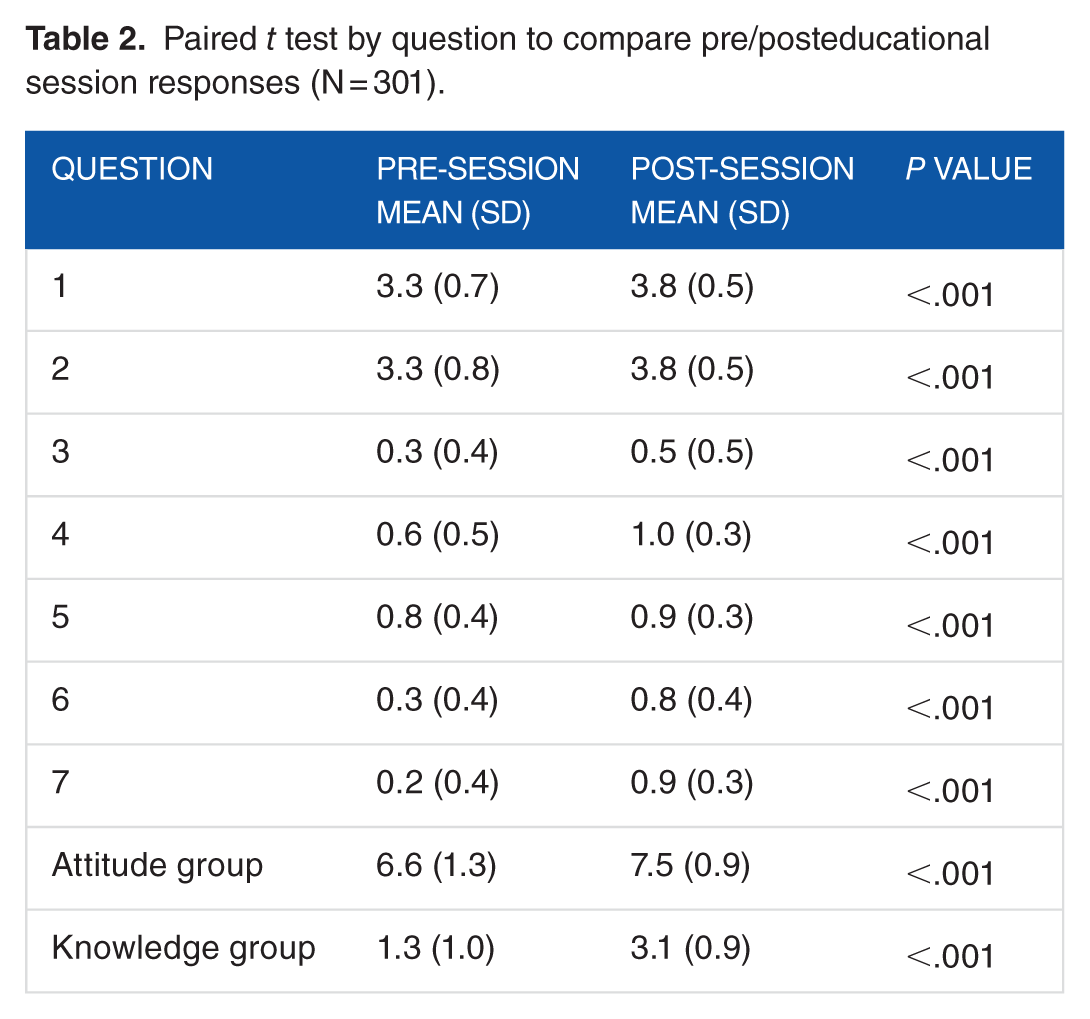
Our study showed that the pilot intervention was readily feasible with all 3 student types. Based on the pre/postevaluation, we found a statistically significant difference in all survey questions before and after the session. Results are summarized in Table 2 and Figures 1 and 2. One student failed to answer an attitudinal question and was not given a score for this specific question. All students answered question 5.
Paired t test by question to compare pre/posteducational session responses (N = 301).

Graphical summary of attitude scores (total Likert) by pre/posteducational session questionnaire.

Graphical summary of knowledge scores (total number correct) by pre/posteducational session questionnaire.
We found an increase in attitude score favoring the importance of a risk discussion associated with obtaining a CT in 174 (58%) students with a mean increase of 1 (1) point on a 5-point Likert scale (P < .001). In addition, we found an increase in knowledge in 256 (85%) students who, on average, answered approximately 2 (1) more questions correctly on the posttest (P < .001). When asked whether pediatric CT examinations should require written informed consent, 249 (83%) students felt that they should prior to the session. After the session, this increased to 273 (91%) students, representing an 8% increase (P < .001).
The PA students were more likely than medical students to prefer obtaining informed consent prior to the session (P = .03). The PA students also reported increased attitude scores toward the importance of radiation risk considerations, such as the patient’s radiation dose history and engaging in radiation risk discussion with patients both before and after the intervention. Results are summarized in Table 3.
Comparison of educational session responses for medical and PA students by student type (n = 290).

In general, the data appear to suggest differences between male and female students in attitude scores toward the importance of radiation risk considerations and favor for obtaining informed consent prior to a pediatric CT study. However, in comparing sex and student type using a χ 2 test, we found that there is a significant association between sex and student type (P < .01). Given this association, the differences between medical students and PA students may be related to either sex or student type differences. For example, the medical students included 64 (43.5%) men and 83 (56.5%) women, whereas more PA students were women (113 [79.6%]) compared with men (29 [20.4%]). Our MANOVA revealed that the differences in pre/postvalues are likely explained by the student type (P < .01). When controlling for students type, we found that sex no longer had a significant effect (P = .09).
In addition to our quantitative analyses, we obtained several comments from students, which we summarized in Table 4.
Selected student comments on the educational session for all student types.

Discussion
For all health care providers, the practice of imaging appropriateness demands a strong skill set, including the “interpretation of the clinical presentation, due regard for available evidence and best practice, cost-effectiveness, limitations, and risk-benefit analysis.” 34 Despite strong advocacy on the part of the radiology community for a compulsory medical school curriculum in radiation safety and appropriate imaging use through initiatives including the Alliance of Medical Student Education in Radiology, Liaison Committee on Medical Education, the Association of American Medical Colleges, and the American Medical Association, important contextual principles of the practice of medicine, including imaging appropriateness, radiation safety, imaging modality differences, and provider-patient risk/benefit communication, are taught rarely.5,23,34,35,41 Importantly, such lack of exposure to the challenges of appropriate imaging and the presence and effects of radiation in diagnostic imaging leaves students feeling unprepared and unsure about their future radiology ordering practices.29,34,42
Our study demonstrates feasibility and a statistically significant impact of a single, brief interactive session on increased awareness and knowledge of the utility, limitations, and risks associated with medical imaging. One recurring theme from our study is the shift in attitude on the part of young students toward the importance of checking the patient’s radiation dose history and discussing risks and benefits of the examination with the patient/caregiver so they can make an informed decision. Students were also more likely to believe that patients/caregivers should provide informed consent before a pediatric CT is ordered. Here, it is important to note that the responses and choices of young students may mirror those of practicing clinicians. According to a recent report, following an educational session, emergency medicine physicians were more likely to believe that patients should give informed consent before a CT scan and predicted that they would be more likely to discuss the risks and benefits of CT with their patients. 30 Despite the uncertainties, ambiguities, goal conflicts, and time pressures affecting both provider and patient/caregiver, imaging decisions and risk/benefit discussions can be open, respectful, and shared. In this study, guidelines for engendering trust within various contextual clinical frameworks, as exemplified in the Image Gently 15 and WHO (World Health Organization) guidelines, 19 were avidly sought and greatly appreciated by our students. The capacity of the provider/patient encounter for processing doubt is part of what makes this unique exchange beneficial.
Our study has several strengths. First, our study had a large sample size and our educational workshops incorporated a diversity of young graduate students, including trainees in the latter 2 groups. Second, our research team members, trained in radiology, public health, health services research, and emergency medicine worked collaboratively to develop and interpret our survey questions and results. Third, our study introduced a straightforward, first-step exposure to a challenge facing the wider community of postgraduate trainees and practicing clinicians. Importantly, young learners’ responses provided a glimpse into their early development and thinking patterns and showed how they anticipate such information informing their future ordering practices and interactions with patients.
One limitation of this study was the short-term evaluation of the outcome measures. Future studies may consider repeated measures of knowledge and attitudes to assess whether the intervention effect is sustained. Another potential limitation was our nonprobability sampling method, which was chosen due to the pilot nature of the study and to curriculum differences between graduate programs. When compared with the general population of medical students, some of the medical students who were enrolled in a radiology elective course may have a stronger interest in issues pertaining to medical imaging utilization and radiation safety. Future studies could use random samples of students to mitigate potential selection bias. Importantly, recent literature suggests that short radiology educational interventions with medical students during initial stages of their preclinical years can exert significant impact, promote critical thinking, inspire self-directed learning, and increase awareness.33,34,43
Conclusions
An educational session for medical and PA students early in their education showed an improved awareness and knowledge of the utility, limitations, and risks associated with medical imaging. Incorporation of a best imagining practice educational session early during medical education may promote more thoughtful imaging decisions for future medical providers.
Footnotes
Appendix 1
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: C.M.S. was supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through grant award number UL1TR001111. The present research represents a self-initiated, nonfunded quality improvement project. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Author Contributions
DA and TSH contributed equally to the development of this manuscript.