
Abstract
Objectives
Education holds transformative power in society, driving economic and social development. In medical education, training quality leads to well-prepared physicians and directly impacts patient care. In Brazil, a key measure of medical training quality is the National Student Performance Exam (Enade). This study aims to analyze the institutional, social, and economic determinants of the quality of medical education in Brazil through Enade scores.
Methods
An ecological study was conducted with all Brazilian higher education institutions participating in the Enade for the Medicine undergraduate course in the last 5 editions. Group comparisons and a multivariable logistic regression model were conducted to examine the associations between institutional, social, and economic aspects with the Enade score, categorizing institutions into high and low/medium score groups.
Results
Considering all editions, the average Enade score of medical schools in Brazil was 2.8. Geographic location was a determining factor of Enade results. The highest proportion of high scores was observed in South (62.4%) and Central-West (57.3%) regions, and low scores in the North (76.4%), Southeast (64.1%), and Northeast (52.6%). The proportion of medical schools with high Enade scores increased over time (P < .001), and they demonstrated significantly higher performance in general knowledge tests (+10.6%; 64.4 vs 58.20) and specific knowledge tests (+16.0%; 65.4 vs 56.4). Institutional factors associated with better student performance in Enade included a well-rated didactic-pedagogical organization (odds ratio [OR]: 1.62 [confidence interval (CI): 1.10-2.40]), a more qualified faculty (OR: 1.81 [CI: 1.27-2.59]), and being publicly administered (OR: 5.74 [CI: 3.44-9.95]).
Conclusion
This study highlights significant variations in training quality among medical schools nationwide, with the Center-South region showing a higher proportion of institutions achieving high Enade scores compared to more socioeconomically vulnerable regions in Brazil. Institutional characteristics such as well-rated didactic-pedagogical organization, a highly qualified faculty, and public administration are associated with better exam performance.
Background
Education is a fundamental social right governed by public policies aiming to ensure equitable access to education for all Brazilian citizens. 1 When offered widely and with quality, it has a transformative power in society, serving as a primary driver for economic and social development in a region. 2 In the context of higher education, educational institutions play a crucial role, acting as guarantors of quality teaching and research, training new professionals to meet social demands as new challenges arise. 3
In the health sector, especially in medical education, the training of new professionals is directly linked to the care provided to the population.4,5 This relationship requires the training of technically well-prepared professionals. However, given Brazil's vast territory and its socioeconomic disparities, it is essential to consider the diverse regional demands, their dynamics, and characteristics.2,6-11
Two of Brazil's 5 geographic regions, the Southeast and Northeast, together account for approximately 70% of the country's total population. In contrast, the North and Central-West regions are characterized by lower population densities. Socioeconomic indicators such as the Municipal Human Development Index (mHDI) and the GINI Index also vary significantly across regions, highlighting deep and persistent inequalities in income distribution, educational attainment, and access to essential public services. 12 In the context of healthcare access, these disparities are further reflected in the uneven distribution of medical professionals. The Southeast region, for example, has 3.39 physicians per 1000 inhabitants, 1.8 times more than the Northeast (1.93) and 2.3 times more than the North (1.45). 13
Due to this shortage of healthcare professionals in less developed regions of Brazil, stemming from the poor distribution of physicians, the country has witnessed a significant expansion, interiorization, and privatization of undergraduate medical courses. 5 This scenario was encouraged by public policies aimed at reducing regional health access inequalities, restructuring medical training, and improving the quality of services provided by the Brazilian Unified Health System (SUS).14,15 These strategies have resulted in a substantial increase in new and complementary medical school seats, especially in regions with a shortage of professionals. Additionally, they have heavily involved private higher education institutions (HEIs) in this educational system.5,16,17
In this context, the most recent data shows that the number of medical schools jumped from 143 in 2004 to 448 in 2024, with the private sector accounting for a substantial 72% of them. 18 A notable regulatory inflection point in this expansion was the enactment of the More Doctors Law (Lei do Mais Médicos) in 2013, which established a structured mechanism for authorizing new medical programs through public calls for municipalities and higher education institutions. This legislation prioritized underserved regions and required specific criteria for institutional participation, thereby promoting both geographic redistribution and diversification in medical education provision.19,20
Despite advances in education and healthcare, it is crucial to reflect on the historical challenges highlighting the complexity of Brazil's educational and health systems. The isolated expansion process raises legitimate concerns regarding the quality of education, as there is no point in increasing the number of graduates without concern for the quality of these new professionals. The increased privatization of medical education, the significant rise in available seats (with a consequent reduction in admission criteria), and the opening of undergraduate courses in economically weaker regions might, in some way, undermine the quality of training. 21
Developing strategies to measure the quality of HEIs and their graduates is essential to ensure efficient public access to healthcare. 22 Strategies implemented by the Brazilian Ministry of Education (MEC) broadly evaluate all undergraduate courses. Among the quality indicators used, one of the most relevant is the Brazilian Student Performance Exam (Enade). Established by Law No. 10,861 in 2004 as part of the Brazilian Higher Education Evaluation System (Sinaes), 23 this exam was designed to assess the quality of undergraduate education in Brazil. It evaluates graduating students’ performance concerning the content specified in their respective Brazilian Curriculum Guidelines (DCN), the development of general and professional skills, and the level of their knowledge on current Brazilian and global issues. 23
Given the exam's significance and impact, studies using it as a benchmark for evaluating the efficiency and effectiveness of health training in Brazil deserve dedicated attention. This study aims to analyze institutional, social, and economic aspects of the quality of medical training in Brazil through Enade performance data. It offers important contributions and reflections on new strategies and public policies related to health education quality and service provision, especially in the context of recent expansion, interiorization, and privatization of medical education in Brazil.
Methods
Ethical Considerations
This study used secondary data from public government sources, published on the Ministry of Education and Ministry of Planning and Budget portals. Therefore, it did not require submission to the Brazilian Research Ethics Committee, as dictated by Resolution No. 510/2016 of the Brazilian Health Council on norms applicable to Human and Social Sciences research.
Design and Setting of the Study
This is an ecological, quantitative study with a descriptive and analytical approach. All Brazilian medical schools that participated in one or more editions of Enade between 2007 and 2019 were included and analyzed according to the number of participations.
Variable Definitions and Data Collection Protocol
The data for this study were sourced from the database provided by National Institute of Educational Studies and Research Anísio Teixeira (INEP). 24 Basic data were identified according to the exam year, higher education institution, undergraduate course (Medicine), municipality, federative unit, state, and geographic region. Institutional information was defined by infrastructure and didactic-pedagogical organization scores, administrative category (public and private), percentages of PhD faculty, and full-time faculty.
For socioeconomic evaluation, indicators such as the Index for the socioeconomic development of municipalities in Brazil (FMDI), the mHDI, and the Statistical measure of income inequality within a nation or a social group (GINI) were used. The national territory was divided into 5 regions according to the official division established by the Brazilian Institute of Geography and Statistics (IBGE). 25
All variables were accessed on public government data websites at the federal, state, and municipal levels, collected in the form of reports, microdata, and statistical summaries. These data were transferred and tabulated in the Microsoft Excel Program. Institutions participating in the exam that had one or more missing variables of interest were excluded from the inferential analyses.
About the Enade
The Enade exam 23 is mandatory for all Brazilian undergraduate courses (ie, medical schools) and is specifically aimed at graduating students. It consists of multiple-choice and open-ended questions, divided into 2 sections: general and specific tests. The general knowledge section includes topics such as Portuguese language, logical reasoning, and geopolitics. In turn, the specific knowledge section focuses on the core curriculum of the medical program, assessing the competencies and skills acquired throughout the training. This section includes questions based on practical scenarios and case studies, aiming to evaluate the student's ability to apply theoretical knowledge in real-life medical contexts. The Enade’s main objective is to evaluate the performance of undergraduate students in relation to the syllabus in the National Curricular Guidelines (DCNs) and, indirectly, the overall quality of the teaching offered by the courses.
Each undergraduate course is evaluated triennially, allowing for a longitudinal assessment of learning processes and institutional teaching quality. Enade results are inputs for Higher Education Quality Indicators, the focus of this study. 23 It is combined with assessments of infrastructure, pedagogical design, and faculty qualifications to compose quality indicators for undergraduate programs in Brazil, such as the Preliminary Course Score (CPC), which is used by the Ministry of Education to evaluate higher education institutions.
The Enade score represents the relative performance of students in a specific undergraduate course, measured against the average performance of students within the same evaluation area nationwide. It is initially calculated as a raw score based on students’ responses across both general and specific knowledge tests. To ensure comparability across institutions, this raw score undergoes a standardization process that adjusts for contextual variables such as the students’ socioeconomic background and prior academic preparation.
The resulting standardized Enade score is then categorized into 5 performance bands, ranging from 1 to 5. Band 1 indicates the lowest performance, while band 5 indicates the highest. 26 This banding process allows individual student scores to be translated into a standardized, comparative indicator of program quality across institutions. While a low Enade score does not directly affect the student, it can have significant implications for the undergraduate program and the higher education institution. As previously mentioned, Enade results feed into the CPC, a broader quality metric. When a program receives a CPC rating of 1 or 2 (on a scale from 1 to 5), it is classified as underperforming and may face a range of consequences, including the obligation to implement a formal improvement plan, and, in more serious cases, the suspension or even termination of the program.
Data Analysis
In descriptive statistics, medians and interquartile ranges were used for continuous variables as measures of central tendency and dispersion. Categorical variables were represented by absolute and relative frequencies. Group comparisons were made using the Mann-Whitney test (for 2 comparison groups), Kolmogorov-Smirnov test (for more than 2 comparison groups), or chi-square test for categorical variables. Bonferroni adjustment for multiple comparisons was applied when appropriate. A P-value < .05 was considered statistically significant.
A logistic regression model was constructed using geographic and institutional characteristics to evaluate their associations with the Enade score. Institutions with all data available were categorized into 2 groups based on their Enade scores: (i) “High score” for institutions classified in bands 4 and 5 and (ii) “Low/medium score” for institutions classified in bands 1, 2, and 3.
Spatial analyses were conducted using the free software Quantum GIS Version 3.32.
Results
Medical Schools Participating in Enade
Among all the participations computed in the editions from 2007 to 2019 that covered undergraduate medical courses, 406 (43.5%) records were in the Southeast region, 213 (22.8%) in the Northeast, 162 (17.4%) in the South, 81 (8.7%) in the North, and 71 (7.6%) in the Central-West region. Despite the increasing number of institutions over the years, the regional proportion remained stable (P-value: 0.998) (Figure 1).
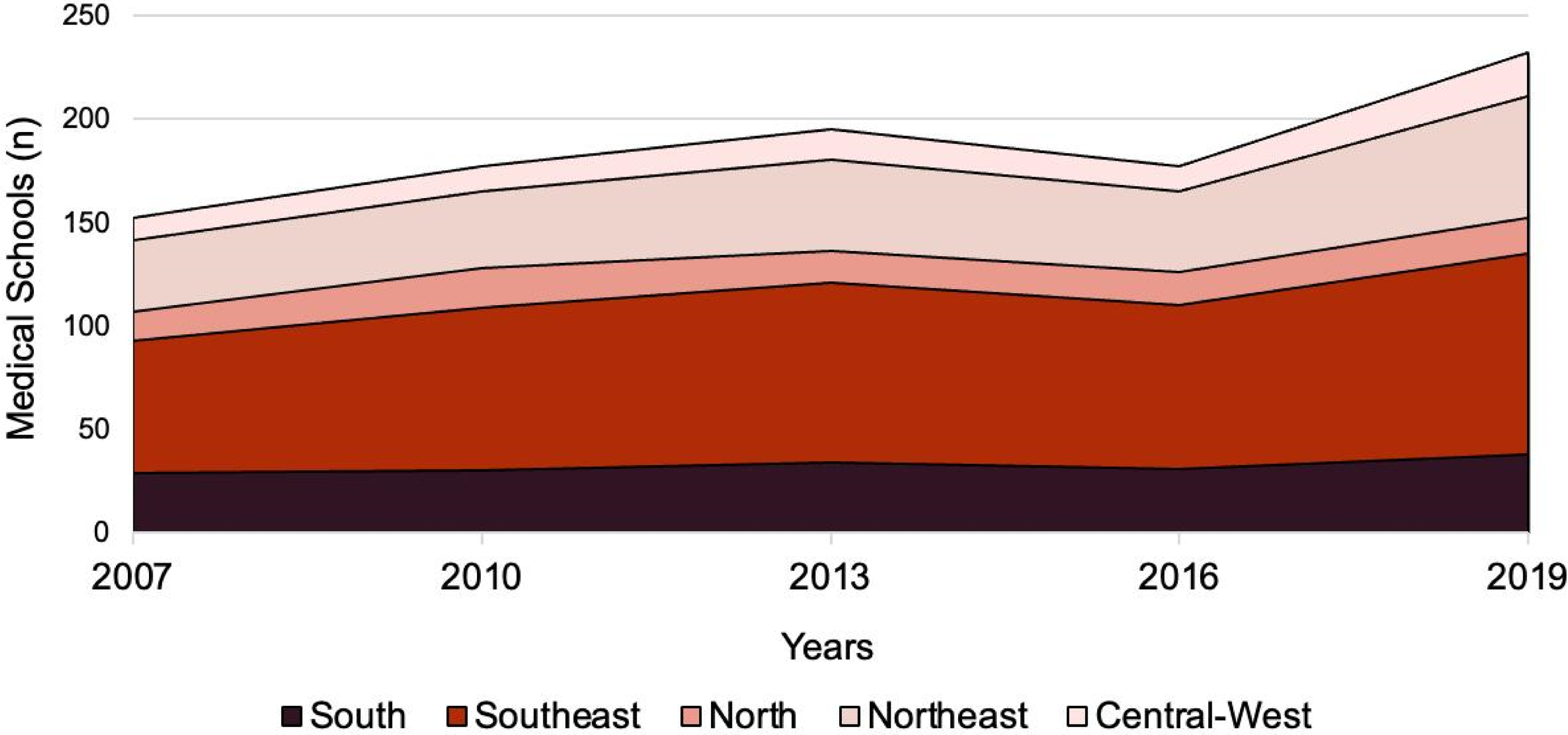
Proportion of Medical Schools Participating in Enade by Region and Year in Brazil.
Performance of Medical Schools in Enade
Considering all exams, medical schools achieved an average Enade score of 2.8, with significant regional variation. The South and Central-West regions had the highest percentage of schools with high scores (62.4% and 57.3%, respectively). Although the Northeast and Southeast regions have the most schools, they had a notable frequency of institutions with low/medium scores (52.6% and 64.1%, respectively). The North region stood out negatively, with a large share (76.4%) of schools in the low/medium category (Figure 2).
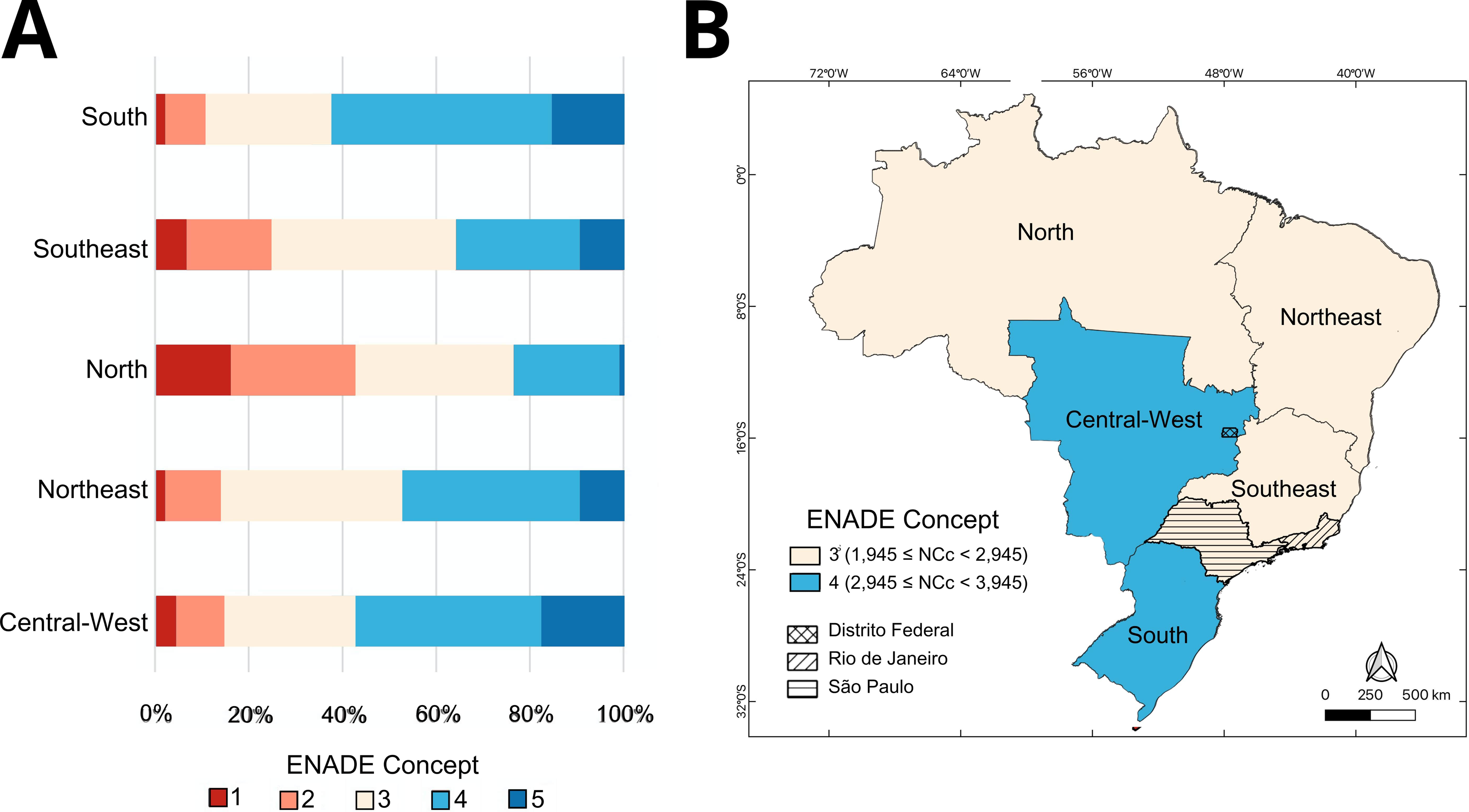
Regional Distribution of Enade Scores Obtained by Medical Schools in Brazil. (A) Proportion of Medical Schools by Enade Score Considering All Exams (2007, 2010, 2013, 2016, and 2019). (B) Map Representing the Majority Band of Each Brazilian Geographic Region.
Longitudinal analysis showed that, despite some fluctuations, the proportion of medical schools with high Enade scores (bands 4 and 5) increased over time when comparing 2007 to 2019 (P < .001; Table 1). Furthermore, during the study period, these schools achieved significantly higher scores in general knowledge tests (+10.6%; 64.4 vs 58.2) and specific knowledge tests (+16.0%; 65.4 vs 56.4).
Comparison Between Enade-Participating Medical Schools With High Versus Low/Medium Performance Scores.

*Only schools that did not contain missing study-relevant data were included; **Enade Notes: “High Score” was considered for bands 4 and 5, and “Low/Medium Score” for bands 1, 2, and 3; Differences between low/medium and high Enade scores were compared using Mann–Whitney and Chi-squared test. ***Number and proportion of public and private participating medical schools in each region—South: 81 private (54.4%) and 68 public (45.6%); Southeast: 271 private (73.0%) and 100 public (27.0%); North: 29 private (42.6%) and 39 public (57.4%); Northeast: 64 private (34.4%) and 122 public (65.6%); Central-West: 29 private (42.6%) and 39 public (57.4%).
Abbreviations: FMDI, Index for the socioeconomic development of municipalities in Brazil; GINI, Statistical measure of income inequality within a nation or a social group; mHDI, Municipal Human Development Index.
Socioeconomic Factors Associated With Enade Scores
When analyzing socioeconomic characteristics, FMDI, mHDI, and GINI index did not show associations with Enade results. However, geographic location was a determining factor. Better performances in the exam were concentrated in HEIs located in the Center-South regions, contrasting with more socioeconomically vulnerable areas (Table 1). For example, 62.4% of HEIs in the South had scores in bands 4 to 5, while only 23.5% of institutions in the North achieved similar performance (Figure 2A).
Institutional Factors Associated With Enade Scores
Faculty qualifications, infrastructure, and the administrative category of HEIs were associated with student performance in Enade. Well-rated didactic-pedagogical organization (adjusted odds ratio [ORa]: 1.62; 95% confidence interval [CI]: 1.10-2.40), a more qualified faculty regarding academic degrees (ORa: 1.81; 95% CI: 1.27-2.59), and being publicly administered (ORa: 5.74; 95% CI: 3.44-9.95) were factors associated with better Enade performance (Figure 3).

Characteristics Associated with High Enade Scores.
Discussion
This ecological study provides a detailed overview of the quality of academic training in undergraduate medical courses in Brazil from 2007 to 2019 through student performance in Enade. To our knowledge, this is the most comprehensive study focusing on this topic.
Analyzing the institutional quality of medical schools revealed that most of them nationwide have low/medium scores. As shown in Figure 2B, no region had an average score in the highest Enade band (band 5). Similarly, it has previously been shown that “most courses obtained a score 3 in the quality indicators proposed by the Ministry of Education.” 27 On the one hand, this observation is concerning and prompts reflection on the training of these professionals and equitable distribution across the country, especially in regions with healthcare shortages. On the other hand, it shows there is substantial room for improvement.
Similar to other socioeconomic aspects in the country, the distribution of medical schools, when considering their number and exam performance, showed an unequal distribution. The Southeast and Northeast regions stand out in the number of schools, correlating with their major populations: the Southeast has 41.8% and the Northeast 26.9% of the Brazilian population. 25 However, in terms of student performance, schools in the central-south region excelled, places with high per capita gross domestic product. 28 Conversely, the North region, less populous and poorer, stood out negatively in both analyses.
In this regard, it is well known that the North and Northeast regions of Brazil are socioeconomically more vulnerable. Given existing evidence of correlations between socioeconomic indicators, such as the GINI Index and the Human Development Index (HDI), and outcomes in education and health29-31 we investigated the impact of these regional indicators on the performance of medical schools. These variables did not show statistically significant associations, possibly because the Southeast region, which stands out in terms of socioeconomic indicators, had the second-lowest proportion of high-performing medical schools.
Still regarding regional disparities in medical school performance, it is important to highlight that, particularly in the field of Medicine, the local health infrastructure plays a crucial role in shaping the quality of training. Learning in medical education is closely tied to the availability and complexity of healthcare services, which directly influence the opportunities for practical experience during clerkships and internships. Evidence shows that several municipalities and states in Brazil face significant shortages in healthcare infrastructure, such as limited numbers of health facilities, diagnostic equipment, and practicing physicians32-34. These limitations may reduce the diversity and depth of clinical exposure, thereby affecting students’ development of essential competencies. This structural inequality in the health system may, at least partially, explain the geographic disparities observed in Enade scores across regions.
Assessing professional training quality cannot be done simplistically through Enade scores alone. However, as SINAES advocates, one of the exam's purposes is to “conduct a longitudinal evaluation of the learning process and teaching quality of institutions.” In this context, noting that medical schools, despite following the same guidelines, perform differently on the national exam is a factor worth reflecting on. These data should guide actions to mitigate this effect, which contributes to perpetuating historical regional inequalities in Brazil, including access to quality healthcare.
Another relevant observation is the association between the administrative category of HEIs and the Enade scores achieved. Public HEIs, generally universities, historically stand out in this regard.21,35 This fact seemingly highlights the inequity in access to education, which has made it paradoxically easier for higher-income backgrounds students from private high schools—generally better than public ones—to achieve higher scores on entrance exams and, consequently, enter public universities (tuition-free) more easily. 36
Although some studies indicate advantages of private institutions in some aspects such as infrastructure and learning environments in clerkships,2,37 the public HEIs account for over 90% of the laureates in the University Talent Award. 38 Additionally, in general, the public HEIs offer more and greater learning opportunities to students (scholarships, scientific initiation, exchanges, university hospitals, etc) and have historical pedagogical foundations ensuring secure teaching operations. Furthermore, there is a higher concentration of faculty members with doctoral degrees and full-time dedication. Together, these aspects may partially explain why public HEIs still present better performance on exam.
Furthermore, it is appropriate to reflect on the possible paradox presented: while public institutions perform better in Enade, there has been a significant and consistent increase in new private medical schools. Currently, 7 out of 10 medical seats in the country are offered by private, for-profit institutions. Therefore, there is an urgent need to adequately and thoroughly regulate this sector, supervising the functioning of all schools (public and private) and providing incentives for quality teaching activities.21,39
Another noteworthy aspect is the association of faculty quality and dedication with student training. It is known that the teacher's activity greatly impacts this aspect, and therefore, it can be inferred that a motivated, engaged, and well-trained faculty can make consistent pedagogical transformations. 40 Thus, the fact that a higher proportion of doctoral faculty is associated with high Enade scores of HEIs is not surprising. Here it is important to mention that, in general, the teaching staff of Brazilian public universities is mostly composed of PhD professors with more time dedicated to research and teaching. On the other hand, professors in the private HEIs are younger, have less teaching experience, and dedication (in hours) to teaching and research. 2
Also, the faculty members at public HEIs complain about the infrastructure offered for work, 2 which may explain our finding that associates poor infrastructure ratings with higher Enade scores. Additionally, private institutions, driven by market dynamics and competition, especially in the medical education field in the country, contrast with the deterioration of public schools, stemming from numerous factors such as poor management, lack of planning, and government investments.
The recent launch of the National Examination for Medical Education Assessment (Enamed) by the Brazilian Ministry of Education reinforces the urgency of addressing structural disparities in medical training. 41 As a unified assessment tool that will combine the Enade and the national residency entrance exam, Enamed aims to evaluate competencies aligned with national curriculum guidelines and strengthen the preparation of medical graduates for the SUS.
In addition to initiatives like this, based on our findings, it is recommended that public policies prioritize targeted faculty development programs, particularly in regions where low Enade performance is concentrated, as a means of enhancing teaching quality and pedagogical consistency. Moreover, regionally sensitive resource allocation, including funding for health infrastructure, faculty qualification incentives, and pedagogical support, is essential to mitigate persistent geographic disparities.
Although Brazil's medical education landscape is shaped by its unique historical, socioeconomic, and political context, the disparities identified in this study—particularly those related to geographic inequities and institutional differences—mirror challenges observed in other low and middle-income countries (LMICs). For instance, India and China have also experienced rapid expansion in medical schools yet differ in how resources are distributed across regions and how regulatory frameworks support quality assurance. In India, private schools are concentrated in wealthier areas, whereas Brazil's policies, such as the “More Doctors” Program, have explicitly promoted expansion in underserved regions. China's emphasis on national accreditation and centralized quality control offers a contrasting model to Brazil, which is more heterogeneous and characterized by regulatory permissiveness and fragility. These international examples suggest that faculty development programs, coupled with equitable allocation of financial and institutional resources, are critical policy tools to mitigate regional disparities in training quality. By integrating lessons from comparable LMICs and tailoring them to Brazil's decentralized higher education system, policymakers can more effectively address educational inequities and enhance the social accountability of medical education nationwide.
As a limitation, the ecological design of this study restricts the ability to make individual-level inferences or establish causal relationships. Additionally, it is important to consider that medical education in Brazil has undergone significant changes over the past decade, shaped by shifting political and social contexts. Among the most impactful factors are student financing policies and the implementation of the “More Doctors” Law (Lei do Mais Médicos), which, in the context of higher education, triggered a major expansion in the number of medical schools and available seats. 42 This law also supported a pronounced process of interiorization and privatization of medical education, especially in underserved regions.13,20 As a result, some of the observed patterns may reflect transitional dynamics, and the full effects of these structural changes, particularly those implemented after 2013, might not yet be fully captured within the study period analyzed.
This program, however, started in 2013. So, its results in the Enade context cannot yet be clearly visualized since many of the new schools had not reached the necessary maturity to participate in this exam during the years analyzed in this study. The HEIs authorized through the “More Doctors” public call began operating around 2017, becoming eligible for the Enade exam from 2023 onwards, an edition whose results had not yet been published at the time this study was conducted. This fact helps to explain why the number of participating schools is significantly lower than the total number of medical schools in Brazil. So, it is important to continuously investigate the quality of the expansion process of schools/seats in the country.
Despite the complexity and difficulty of measuring HEI teaching quality, it is essential to consider the available indicators to track success and progress in medical education. This study sheds light on a well-recognized theme in the Brazilian educational scenario but still underexplored. Understanding the landscape of medical training in the country and the spatial inequality of teaching quality and course offerings highlights the relevance and need to (re)evaluate the training process of these essential professionals to meet the health demands of the Brazilian population and communities.
Conclusion
This study provides a panoramic view of the quality of medical training in Brazil, considering institutional, social, and economic aspects. Overall, medical schools nationwide show clear variation in training quality. The Center-South region has the highest percentage of schools with high Enade scores, contrasting with the more socioeconomically vulnerable regions, suggesting that geographic location may be a determining factor in exam excellence.
Institutionally, having a well-rated didactic-pedagogical organization, a highly qualified faculty, and being publicly administered characterize HEIs with better exam performance. This study brings important reflections on new strategies and public policies related to health training quality and service provision, considering (I) the scenario of expansion, interiorization, and privatization of medical education in Brazil; (II) Brazil's historical regional inequalities; (III) the different performances of medical schools, despite following the same curricular guidelines; (IV) the responsibility of medical professionals in meeting the health needs of the Brazilian population and communities.
Finally, it is hoped that this work will contribute significantly to the field and serve as a foundation for new discussions on the efficiency and effectiveness of health professional training quality and its impacts on Brazil's landscape of scarcity and inequality.
Footnotes
Abbreviations
Ethical Considerations
This research did not require ethics approval or informed consent as it did not involve human participants. The study was conducted in accordance with local and institutional regulations.
Consent to Participate
Written informed consent was not applicable.
Author Contributions
QHF and FGMS was involved conceptualization, investigation, methodology, validation, writing—original draft, and writing—review & editing; KMA in conceptualization, formal analysis, methodology, validation, writing—original draft, and writing—review & editing; RCM in formal analysis, methodology, validation, writing—original draft, and writing—review & editing; and BBA and LFQ in conceptualization, data curation, formal analysis, funding acquisition, methodology, project administration, supervision, writing—original draft, and writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Intramural research program of the Oswaldo Cruz Foundation (Fiocruz), Brazil. BBA is a senior scientist from the Brazilian National Council for Scientific and Technological Development (CNPq 1D). KMA is a postdoctoral researcher at Gonçalo Moniz Institute, Oswaldo Cruz Foundation. QHFB was supported by the Coordination for the Improvement of Higher Education Personnel (CAPES), Brazil, through a master's scholarship. The funding source played no role in study design, data collection, analysis or interpretation, or the writing of the manuscript. The researchers retain complete independence in the conduct of the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.