
Abstract
Background
Goals of care (GOC) conversations in the emergency department (ED) are often a brief discussion of code status rather than a patient-oriented dialogue. We aimed to develop a guide to facilitate conversations between ED clinicians and patients to elicit patient values and establish goals for end-of-life care, while maintaining ED efficiency. Paths of ED Care, a conversation guide, is the product of this work.
Design
A multidisciplinary/multispecialty group used recommended practices to adapt a GOC conversation guide for ED patients. ED clinicians used the guide and provided feedback on content, design, and usability. Patient-clinician interactions were recorded for discussion analysis, and both were surveyed to inform iterative refinement. A series of discussions with patient representatives, multidisciplinary clinicians, bioethicists, and health care designers yielded feedback. We used a process similar to the International Patient Decision Aid Standards and provide comparison to these.
Results
A conversation guide, eight pages with each page 6 by 6 inches in dimension, uses patient-oriented prompts and includes seven sections: 1) evaluation of patient/family understanding of disease, 2) explanation of possible trajectories, 3) introduction to different pathways of care, 4) explanation of pathways, 5) assessment of understanding and concerns, 6) code status, and 7) personalized summary.
Limitations
Recruitment of sufficient number of patients/providers to the project was the primary limitation. Methods are limited to qualitative analysis of guide creation and feasibility without quantitative analysis.
Conclusions
Paths of ED Care is a guide to facilitate patient-centered shared decision making for ED patients, families, and clinicians regarding GOC. This may ensure care concordant with patients’ values and preferences. Use of the guide was well-received and facilitated meaningful conversations between patients and providers.
Introduction
We face an aging population, increased longevity with chronic illness, and more patients visiting emergency departments (EDs) at end-of-life—potentially receiving unwanted care. 1 Intensity of care at end-of-life does not always improve quality of life or quality of death. 2
In Dying in America, the Institute of Medicine analyzes the gaps in care for patients near end-of-life. Barriers include personal/cultural variability in approach to dying, few palliative and end-of-life care specialists, and a rising elderly population within a health care culture that does not readily engage in discussions on death/dying. 3 With more older Americans, 4 clinicians will be increasingly challenged to bridge end-of-life care with patient/family values and communicate to prioritize alignment.
Barriers to obtaining patient-centered goals of care (GOC) in the ED has been previously evaluated,5,6 and publications have called for focused research in this area within emergency medicine (EM).7–9 The 2016 Society of Academic Emergency Medicine Consensus Conference focused on shared decision making (SDM), including at end-of-life. Early palliative team involvement improves patient care, although palliative consultation from the ED is infrequent. 7 SDM has been shown to be a feasible endeavor in the ED. 10
With a common commitment to treat patients with dignity and respect at the end-of-life, we engaged patients, caregivers, emergency clinicians, geriatricians, intensivists, palliative care specialists, bioethicists, and health care designers to produce a conversation guide, Paths of ED Care, to facilitate meaningful GOC discussions and SDM in the ED. We aimed to develop a guide that would elicit what is important to the patients/families at end-of-life, aligning care and values.
Methods
Multidisciplinary conversations established the goal of the conversation guide: ensuring concordance of patient wishes and treatment with mutual understanding of the current situation of illness. The study was conducted at Mayo Clinic St Marys Hospital, a quaternary care hospital with 77,000 ED visits annually. Patients and providers were recruited as a dyad. Early in the process only ED clinicians who volunteered to participate were included, but this was later broadened to include all ED clinicians. Inclusion criteria for patient/family were the following: presentation to the ED, patients at risk for critical illness as determined by Elders Risk Assessment (ERA) Score 16+ (Supplementary Figure 1), 11 age greater than 60 years, two or more hospitalizations in the last 6 months, ability to provide informed consent, medical stability, and ability to participate without delaying care. During the latter part of the trial we expanded criteria to include ED clinician gestalt, rather than ERA score, with the goal of increasing recruitment. This change allowed us to recruit patients without the burden of accessing the ERA score within the medical record, a step that was perceived to be a barrier to recruitment. ERA scores were initially collected as part of eligibility screening, and were ultimately gathered for all patients, including those who were recruited after this criterion was eliminated. Exclusion criteria were the following: Glasgow Coma Scale score <15, altered mental status, incarcerated/police custody, or communication barriers that precluded guide use. Signed informed consent was required for both patient and clinician participants per Institutional Review Board of Mayo Clinic in Rochester, Minnesota.
The primary designer observed the milieu of the ED in order to understand the context in which the guide would be used. These observations were shared with the team developing the conversation guide. Roundtable discussions and iterative revision process using team feedback resulted in a pilot version.
Emergency medicine physicians, nurse practitioners, and physician assistants (“ED clinicians”) were asked to use the guide. Trained research coordinators obtained consent, recorded the encounter, and took notes using an observation guide. We used a predefined observation grid to identify patterns of patient-clinician conversations, nonverbal behaviors, and attitudes, incorporating results into subsequent iterations. A brief structured interview with the patient/family and clinician included targeted questions for each group.
We performed iterative revisions and feedback cycles (Figure 1)12–14 until we had a guide that was discrete, intuitive, required minimal training, met patient/caregiver and clinician needs, and facilitated continuity with downstream specialists.

Iterative refinement process for creation of the conversation guide.
After developing our conversation guide, we did a retrospective comparison of our process compared to International Patient Decision Aid Standards (IPDAS) criteria.15,16
Results
We recruited 25 patients, and 10 unique providers participated in the study. Care providers included EM-boarded physicians, EM residents, nurse practitioners, and physician assistants. Feedback was not segmented by role. The median ERA score was 15.5 (mean 13.7; n = 24, missing = 1). The most common chief complaint was shortness of breath. Other common complaints included weakness/fatigue, abdominal pain, and gastrointestinal bleeding. Enrollee demographics were not collected. We initially created an electronic guide. After initial experimentation, we agreed that transitioning to a single-use paper form the clinician brings to the bedside would be more beneficial. Feedback on this iteration included adding graphic representation, inclusion of patient values by naming different potential concerns, and conversion to paper to improve accessibility and allow the patient/family to keep the guide for reference.
Prior to implementation of the guide, observations of overall ED workflow revealed a common theme of fragmentation in patient and digital interactions. Activity was near-constant with frequent interruption. Clinicians had limited time to spend on any single case, switched modes often between patient interactions, medical record use, forming hypotheses, and documentation. The information-scape was fragmented—code status, advanced directives, alternate decision makers, advance care planning, and ERA were scattered across modules.
Multispecialty stakeholder discussions, informed by observations of the ED milieu and local patient flow, resulted in a vision of a guide to help clinicians co-create a care plan with patients that might 1) centralize information related to advance care planning, 2) improve ease of obtaining GOC, 3) provide a way to initiate GOC conversations, 4) help clinicians navigate deeper discussion of patients’ priorities and values, 5) provide a location to indicate patient preferences for downstream clinicians, and 6) identify patient resource needs to transition to discharge.
As part of our development process, we evaluated existing resources and their relative applicability to our setting. The Serious Illness Conversation Guide (SICG) 17 is a high-quality resource, and we began with modifications to the SICG to meet ED needs.
The revised eight-page prototype, Paths of ED Care, included seven sections: 1) evaluation of patient and family understanding of disease, 2) presentation of care team view (possible trajectories of disease), 3) introduction of different pathways of care, 4) care pathway explanation, 5) assessment of patient/family understanding and concerns, 6) discussion of code status, and 7) personalized summary. Patient-oriented prompts facilitated dialogue between patients and clinicians. The patient choice to pursue either relief of symptoms or repair (curative/procedural interventions) was introduced, based on feedback from our design team patient representative. A frank discussion on code status and a form to document discussion highlights to encourage sharing with loved ones and downstream care teams concluded the guide.
The third version included new images tying together the pathway theme with GOC concepts. A splitting walkway introduced the concept of choice and a fallen tree represented an impetus to discuss code status. Hand-written text was converted to typeface. Feedback on this prototype centered on nonintuitive flow of the conversation, and a near-universal patient sentiment of discomfort with some imagery. Clinicians and patients appreciated the content, and there were no concerns regarding time to use.
The final prototype, an eight-page, 6 by 6 inch paper guide, was completed in January 2020 (Figure 2). It included reversion to a typical page flow, removal of the fallen tree, and the blank form. Prior versions are available in the Supplementary Figure 2.

Paths of ED care decision aid.
Feedback on our conversation guide indicated surprise and appreciation for how brief, yet in-depth, conversations were. Patients appreciated having a meaningful conversation with their clinician, and felt they were able to spend more time with the physician than usual. No clinicians indicated that the conversation took excessive time to use. The mean time to complete the conversation was 9.7 minutes (SD 5.1 minutes). An assessment of each component of the IPDAS15,16 is available in Table 1.
Comparison of Utilized Design Process with International Patient Decision Aid Standards
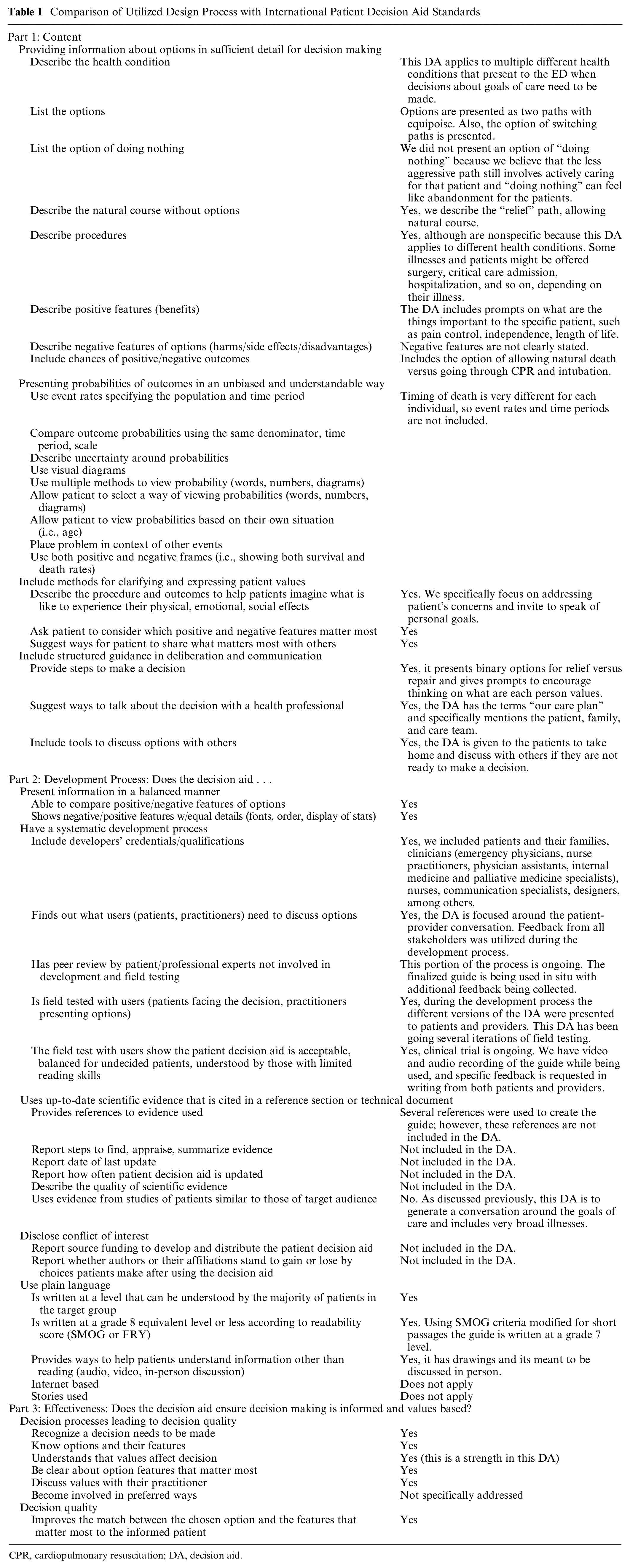
CPR, cardiopulmonary resuscitation; DA, decision aid.
Discussion
This conversation guide is novel and is intended for ED use. This setting requires efficient decisions about GOC. The fragmented environment, frequent interruptions, and lack of care continuity have created barriers to having patient-centered GOC conversations.
Paths of ED Care does not include instructions and is designed with novice users in mind. ED clinicians receive minimal training to discuss patient preferences regarding end-of-life 18 yet often need to urgently engage patients in these decisions. Utilization of this guide may bridge the confidence and skills gap to enable more clinicians to provide care that is concordant with patient values.
Our conversation guide was developed with SDM in mind, although the form evolved throughout the process away from more traditional SDM tools. Use of the IPDAS criteria as comparison illustrates the similarities between traditional SDM guide and our conversation guide. Of the 50 items on the checklist, our conversation guide fulfills 30, and of the 20 that were not met, 9 were prompts to include probabilities of different events, which is not possible to do with the broad context of GOC at end-of-life (Table 1).
Limitations
The primary challenge in this study was enrollment. We were initially required by our institutional review board (IRB) to involve only clinicians who were involved in ED GOC initiatives, resulting in a potentially biased sample, and limiting the patients who were eligible due to the dyad recruitment method. Broadening the clinicians who were able to recruit increased the pool of potential patients. We also adjusted the inclusion criteria from objective criteria (ERA score) to gestalt during the study, which may affect the results. The first field-testing period overlapped with implementation of a new electronic medical record, creating systems, and technical and human factors challenges. These barriers prompted us to reduce the number of participants per iteration cycle. After a few months of recruitment, we were granted permission by the IRB to enroll all ED clinicians in the study, and they were consented at a scheduled department meeting. The changes in our recruitment criteria lowered the average ERA score. By the original criteria the minimum score would be 16, and the mean was 15.5. There are many ways to assess if a patient is appropriate for GOC conversations, and we do not think that moving away from the initial inclusion criteria by ERA score compromises the value of the study and the applicability of the conversation to many individuals.
The choice between relief and repair may represent a less nuanced approach to the conversation and does not account for situations in which the patient may want to pursue a degree of repair within the broader context of seeking symptomatic relief.
We did not utilize a formal checklist for decision aid development, such as the IPDAS checklist, which would have strengthened our methodology, 16 though most of the criteria were fulfilled.
Conclusion
Using iterative development, we created a GOC conversation guide for use in the ED. We found that the approach was well received and the time taken to have conversations were not a burden to ED clinicians. Feedback on the quality of the tool improved throughout the phases of development, and we believe the current iteration is feasible to deploy in the ED setting. Our next study phase will focus on feasibility of implementing this product within our department and, ultimately, externally. This will serve as additional peer review of the guide and as an opportunity to learn from the experiences with different settings, clinicians, and patients.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683211058082 – Supplemental material for Paths of Emergency Department Care: Development of a Decision Aid to Facilitate Shared Decision Making in Goals of Care Discussions in the Acute Setting
Supplemental material, sj-docx-1-mpp-10.1177_23814683211058082 for Paths of Emergency Department Care: Development of a Decision Aid to Facilitate Shared Decision Making in Goals of Care Discussions in the Acute Setting by Laura E. Walker, M. Fernanda Bellolio, Claudia C. Dobler, Ian G. Hargraves, Robert J. Pignolo, Kevin Shaw, Jacob J. Strand, Bjorg Thorsteinsdottir, Michael E. Wilson and Erik P. Hess in MDM Policy & Practice
Supplemental Material
sj-png-2-mpp-10.1177_23814683211058082 – Supplemental material for Paths of Emergency Department Care: Development of a Decision Aid to Facilitate Shared Decision Making in Goals of Care Discussions in the Acute Setting
Supplemental material, sj-png-2-mpp-10.1177_23814683211058082 for Paths of Emergency Department Care: Development of a Decision Aid to Facilitate Shared Decision Making in Goals of Care Discussions in the Acute Setting by Laura E. Walker, M. Fernanda Bellolio, Claudia C. Dobler, Ian G. Hargraves, Robert J. Pignolo, Kevin Shaw, Jacob J. Strand, Bjorg Thorsteinsdottir, Michael E. Wilson and Erik P. Hess in MDM Policy & Practice
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by a grant from the Emergency Medicine Foundation, a philanthropic foundation. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Authors’ Note
This work was performed in the Emergency Department of Mayo Clinic in Rochester, Minnesota, with support from the Knowledge and Evaluation Research Unit at Mayo Clinic. This study was previously presented at the American College of Emergency Medicine Scientific Assembly, 2018.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.