
Abstract
Introduction
Historically, copperhead snake (Agkistrodon contortrix) envenomations were not treated with antivenom owing to related adverse events and little benefit. However, recent studies have shown improved outcomes with antivenom use. We hypothesized that the frequency of antivenom use for copperhead envenomation in Ohio has increased as benefits of administration became more widely known.
Methods
All copperhead snakebites reported to the Ohio poison control centers from 2006 through 2016 were compiled. Antivenom use, bite severity, and disposition were abstracted. A nonparametric test for trend was used to evaluate changes over time for the number of patients treated with antivenom and patient disposition. Logistic regression was used to assess the odds of admission vs discharge with antivenom administration, bite severity, age, and sex as independent variables.
Results
Ninety-eight patients reported copperhead snakebites to the poison control centers. The test of trend showed no change in the proportion of patients treated with antivenom by year (P=0.42). There was no difference in the proportion of patients discharged home (P=0.38) per year. Logistic regression showed antivenom use was associated with an odds ratio for admission of 46.7 (95% CI: 7.3–296.4).
Conclusions
The frequency of antivenom use for copperhead bites did not significantly increase between 2006 and 2016. Administration of antivenom was associated with a large increase in the odds of admission to the hospital, even when controlling for bite severity. Further education regarding the benefits and safety of antivenom may increase its use for copperhead snakebites, but may lead to an increase in hospital admissions.
Introduction
Approximately 5000 to 9000 people in the United States present to an emergency department (ED) each year with snakebites. 1 Copperhead (Agkistrodon contortrix) snakes, a member of the family Crotalidae, are one of the more common, resulting in approximately 2000 ED visits in the United States per year. 2 As shown by NatureServe and the International Union for Conservation of Nature from 2007, their range extends throughout Mexico and much of the United States, including the Midwest, Southeast, and Mid-Atlantic (Figure 1). However, despite the frequency of copperhead envenomation, management of these bites remains controversial. 3 -8
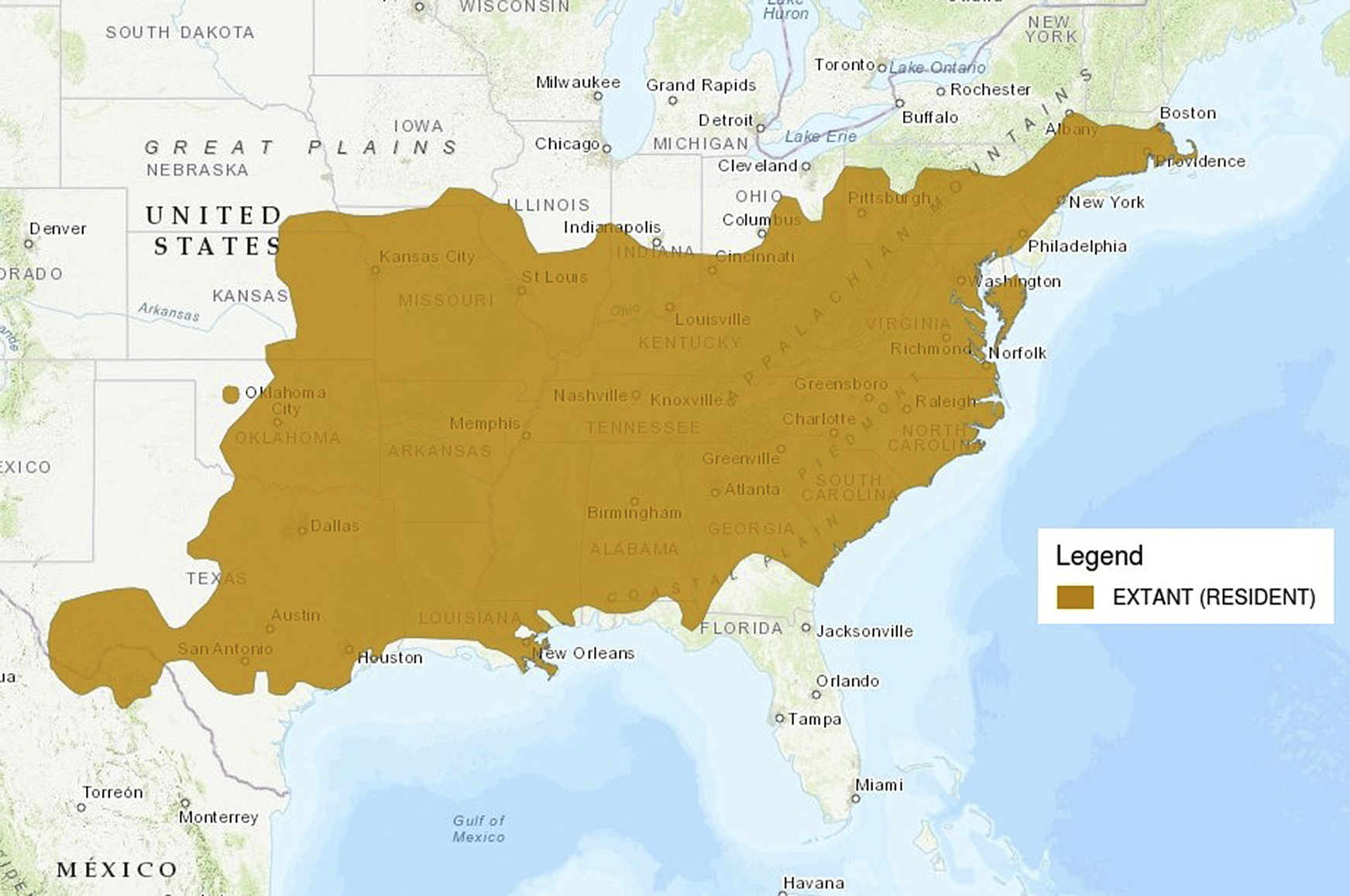
Distribution map of copperhead snakes (Agkistrodon contortrix), courtesy of NatureServe and International Union for Conservation of Nature, 2007.
Severe crotalid envenomations can result in local tissue destruction, coagulopathy, shock, and death. 9 -11 In instances of severe envenomation, the decision to use antivenom is fairly straightforward. 12 However, copperhead snake envenomations rarely cause severe symptoms and are almost never fatal.10,13,14 Most copperhead envenomations result in only local pain, swelling, and ecchymosis, with rare nausea or paresthesias.10,13,14 Coagulopathy is often the most concerning symptom of pit viper envenomations.10,13 However, it is a minor concern with copperheads, because most coagulopathy is not associated with significant bleeding.10,13 Approximately 7% of copperhead bites in patients who present to the ED are dry bites. 15 As a result, copperhead snakebites were not historically treated with antivenom, because the risks of adverse events were thought to be too high.5,16,17 This was especially true before the release of Crotalidae Polyvalent Immune Fab-Ovine (CroFab, BTG, UK) in 2000. 18 CroFab is a much smaller polyvalent antibody fragment (Fab), with a much lower incidence of allergic reactions and serum sickness than the previously available horse-derived IgG antibody. 19 It is typically dosed from 4 to 6 vials as an initial dose, with repeat doses of 2 vials given every 6 h for 18 h. 20 Vials contain a lyophilized powder with standard minimum mouse LD50 neutralizing units per vial for 4 common pit vipers found in the United States. 20 The powder is first reconstituted and then diluted in normal saline and infused intravenously over 60 min. 20 Hospital admission is often required when administering antivenom for repeat dosing. 20
Despite the historical reluctance to use antivenom for copperhead bites, recent studies and case reports have shown improved outcomes in copperhead envenomations treated with antivenom, including less morbidity, quicker return to work, and less opiate pain medication use.21,22 Thus, anecdotally, toxicologists and poison controls centers have become more aggressive with the use of antivenom for copperhead bites.
As part of this change, it has been suggested that bite severity is being inadequately gauged in copperhead bites.8,23 Bite severity has traditionally been measured with a traditional snakebite severity score, which focuses on systemic symptoms and laboratory analysis to determine the need for antivenom. 23 Bites are graded 0 to 4, with grades of 2 to 4 requiring involvement of systemic symptoms. 23 Given this requirement, some have postulated that traditional snakebite severity scores minimize the symptoms associated with copperhead envenomations, leading to undertreatment. 8 Instead, they have recommended focusing on local effects with a local severity score to better determine the need for antivenom. 8 In this score, bites are graded from 0 to 4, but pain, swelling, ecchymosis, and time of progression determine the grade, with no weight put on systemic effects. 8
We hypothesized that use of antivenom for copperhead envenomations would increase over time. We also hypothesized that antivenom administration would increase the odds of admission to the hospital when controlling for bite severity.
The primary objective of this study was to describe the use of antivenom for copperhead envenomations over a 10-y time frame (2006–2016) in the state of Ohio. Secondary objectives included assessing temporal patterns for the amount of antivenom used per treated bite, changes in disposition over time, bite severity, and contributing factors to disposition from the ED.
Methods
This study was approved by the institutional review board of the University of Cincinnati. The requirement for informed consent was waived by the institutional review board. This study is a retrospective chart review of all copperhead snakebites reported to the Ohio poison control centers (PCCs) from January 1, 2006, through December 31, 2016, for which records were readily available. Patients who were bitten by a snake, with the bite reported to the PCC by the patient, the patient’s family, or a medical facility, were identified by searching the PCC medical record. Cases were included if the snake was positively identified as or suspected to be a copperhead snake. Cases were excluded if the snake could not be identified at all or if it was confirmed or suspected to be another species. Paper copies of the PCC medical record were printed, and data were extracted and entered directly into an electronic research database (REDCap). 24
The primary study outcome was the number of patients who had a copperhead envenomation treated with antivenom per year over the study period. CroFab was the only antivenom used. Secondary outcomes were the amount of antivenom used per treated snakebite, disposition from the ED, bite severity as estimated by the PCC practitioner, and bite severity estimated using both a traditional snakebite severity scale and the local snakebite severity scale.8,23
Fisher exact test was used to compare categorical data and Student’s t-test to compare continuous variables in bivariate comparisons. A nonparametric test of trend was used to assess the change in the proportion of patients treated with antivenom, the proportion of patients dispositioned home over time, and bite severity over time. Negative binomial regression was used to compare the total amount of antivenom per patient over time, and linear regression was used to examine the number of patients with snakebite reported over time. Multivariable logistic regression was used to identify risk factors associated with ED disposition after snakebite treatment. Model fit (Hosmer-Lemeshow goodness-of-fit test) and calibration (area under the receiver operating characteristic curve) were used to assess the quality of the final model. Data are presented as mean±SD. A P-value of ≤0.05 was considered statistically significant. Statistical analyses were conducted using Stata v15.2 (Stata Corp LLC, College Station, TX).
Results
Ninety-eight patients were included in this analysis. Seventy (71%) patients were male, and the age was 34±20 y. Forty-four (45%) patients were treated with antivenom, with 8±5 vials of antivenom used per patient treated. Fifty (52%) patients were admitted to the hospital. Bite severity and additional demographics are described in Table 1.
Clinical and demographic characteristics of patients with copperhead snakebite reported to Ohio poison control centers from 2006 through 2016, stratified by patient disposition from the emergency department
AMA, against medical advice.
Fisher exact test.
Student’s t-test.
Denotes significant P values < 0.05.
The proportion of patients treated with antivenom, amount of antivenom used per patient treated, and disposition from the ED did not significantly vary over time (Table 2). There was no change in bite severity over time (Table 2). Admission to the hospital was significantly associated with use of antivenom, as well as increased severity graded by a traditional bite severity scale, a local bite severity scale, and the severity as estimated by PCC (Table 1). Logistic regression revealed that patients treated with antivenom had an adjusted odds ratio for admission of 46.7 (95% CI 7.3–296.4) compared with those not treated. Bite severity as measured by local bite severity scale also increased the odds of admission, with each point increase in bite severity associated with an adjusted odds ratio of admission of 4.6 (95% CI 1.7–12.6; Table 3).
Number of snakebite patients, proportion of patients treated with antivenom, proportion of patients with a disposition home from the emergency department, amount of antivenom per treated patient by year, and bite severity by year
IQR, interquartile range.
Linear regression.
Nonparametric test for trend across ordered group.
Negative binomial regression.
Logistic regression for hospital admission as outcome
Adjusted for all variables listed; Hosmer-Lemeshow goodness of fit: P=0.25; area under the receiver operating characteristic curve: 0.951.
Discussion
Management of copperhead envenomations remains controversial. Historically, providers were concerned about the negative effects of antivenom in the setting of mild envenomation symptoms.13,17,25 However, recent studies have shown improved outcomes with the use of antivenom. 6,7,13,17,26-29 Despite new evidence showing the benefits of antivenom therapy, the use of antivenom for copperhead snake envenomations did not change in Ohio between 2006 and 2016. There was no increased use of antivenom for all reported patients bitten by copperhead snakes. There was no change in the severity of bites that were discussed with the PCC over the study period, so it is unlikely that patients with less severe envenomation were treated with antivenom over time. Additionally, there was no change in the amount of antivenom used per snakebite treated with antivenom.
Unfortunately, reasoning for the decision of whether to administer antivenom was not available; only information from the PCC was available. Staff and toxicologists at PCCs act in an advisory role, and the final decision rests with providers managing the patients in person. The lack of change over time may reflect the controversial nature of the use of antivenom for copperhead snakebites, or it may reflect a lack of dissemination or integration of newer research. The majority of studies and guidelines promoting or describing aggressive use of antivenom in copperhead bites have been published from 2010 onward, and there have been studies showing lack of benefit in that time frame as well.3,7,16,21,22,30 Before 2010, most published reports of successful use of antivenom for copperhead envenomations were case reports.9,31,32 Increased provider education may lead to increased use of antivenom for copperhead bites, which may lead to decreased use of narcotic pain medication and improved return of limb function.
There was no change in ED disposition for patients presenting with copperhead bites, with similar proportions being admitted and discharged year to year. There was no association between disposition and sex, despite some evidence that males have demonstrated better recovery than females from copperhead bites. 33 Both bite severity (by all 3 scales) and use of antivenom were significantly associated with increased odds of hospital. Use of antivenom had the strongest association (ie, higher odds ratio) with admission in the multivariable model that included bite severity. This likely corresponds with the underlying concern about adverse events, such as anaphylaxis, which may require intervention, or the need for additional doses of antivenom should symptoms recrudesce. It is also possible that the severity of the bite does not capture the anticipated clinical course and need for antivenom, as the severity of bite did not have as strong an association with admission to the hospital as use of antivenom. If less severe bites are treated with antivenom, this may lead to an increase in hospital admission and possibly increased cost for these patients. 34 This is relevant in the setting of increasing concerns about healthcare costs and emergency department boarding.35,36
Future studies should evaluate antivenom use across the United States as more studies are published and the current studies become more disseminated into standard emergency medicine and toxicology practice.
Limitations
The data collected represent a 10-y period that ended in December 2016, and more studies recommending the use of antivenom for copperhead bites have been published since. These data represent a single state and may not reflect nationwide practice patterns. Grading for severity of bites was performed by staff at PCCs, and no standard grading system was used for the grading. Outcomes other than ED disposition were not available. Potential dry bites were not excluded because it was impossible to definitively determine which bites were dry. However, these were included across all years and are thus unlikely to introduce systemic bias. Suspected copperhead bites were included because definitive identification by a provider significantly limited the number of envenomations. However, these suspected copperhead envenomations were managed by PCCs and providers as if they were confirmed copperhead bites. It was also believed that including suspected bites would accurately reflect clinical practice, where definitive identification of a snake is usually unavailable. Additionally, the only other venomous snakes in Ohio are rattlesnakes, which are unlikely to be confused with copperheads. 37 Finally, this is a retrospective study that cannot establish cause and effect, and we cannot rule out the effect of unknown or unstudied confounders or sources of bias.
Conclusions
We did not detect any significant changes in the proportion of copperhead snakebites treated with antivenom or amount of antivenom used in the state of Ohio over the years 2006 through 2016. Use of antivenom was associated with increased odds of hospital admission after treatment in the ED. Increased provider education may lead to increased use of antivenom for copperhead bites, which may lead to an increase in hospital admission.
The work described in this manuscript was presented as a lightning oral abstract presentation at the virtual Society of Academic Emergency Medicine annual meeting, May 12–15, 2020 (meeting was scheduled to be in Denver, CO, but transitioned to virtual format due to COVID-19).
Footnotes
Acknowledgements
Author Contributions: Study concept and design (WP, SG, EO); acquisition of the data (WP, SG); analysis of the data (WP, US); drafting of the manuscript (WP, US); critical revision of the manuscript (US, SG, EO); approval of final manuscript (WP, US, SG, EO).
Financial/Material Support: None
Disclosures: None