
Abstract
Background:
Recreational drug use is common at large-scale dance events such as the Amsterdam Dance Event (ADE) and severe drug-related complications and deaths occur. Increasing concentrations of cocaine, amphetamine and MDMA have been observed in samples from dance events. Therefore, large dance events are expected to cause an increasing amount of recreational drug related complaints (RDRC) and an increased demand on emergency medical services.
Aim:
To evaluate the impact of recreational drug related complaints (RDRC) during ADE 2016, compared to regular weeks, and to evaluate the requirement for additional medical personnel.
Methods:
For this prospective, observational cohort study, patients >12 years old presenting with RDRC at first aid stations (FAS), ambulance service (AA) and ED during ADE, between October 19th and October 24th 2016 were included. From 2 EDs and AA, the RDRC 2 weeks before and after ADE were also collected.
Results:
An estimated 375.000 people attended ADE. The number of patients with RDRC was 459 at the FAS, 113 at AA and 81 at the ED, and increased significantly during ADE with 225% at AA and with 236% at OLVG ED. Eight patients were admitted. A higher percentage of poly-drug use among ED patients (58%) was found, compared to FAS patients (25%). Also, the proportion of tourists in ED’s (51%) was higher compared to FAS (30%).
Conclusions:
During ADE 2016, the number of intoxicated patients increased significantly. Eight patients were admitted to the hospital, without any deaths. The absolute number of patients stayed within normal range of emergency medical services capacity.
Introduction
It is estimated that more than 25% of the European Union population, aged 15 to 64 years old, have used illicit substances at least ones in their lifetime. 1 Over the years, the Dutch national Drugs Information and Monitoring System DIMS showed a substantial increased concentration of cocaine and amphetamine in samples, and 3,4-methyleendioxymethamfetamine (MDMA) in ecstasy (XTC) tablets (76 mg in 2006 to 156 mg in 2016), raising concern among medical professionals for increased risk of complications from these drugs.1-4 It is known that electronic dance music festivals (EDMF) are associated with psychoactive substance abuse and deaths. 5
Amsterdam Dance Event (ADE) is the largest indoor electronic dance music festival in the world, with over 300 000 visitors annually. At large-scale dance events like ADE, recreational drug use is common,6,7 and 27.4% of incidents at these events are drug-related. 4 Besides frequent alcohol and cannabis use (>50%), in 2016 the most commonly used recreational drugs at these events were MDMA, amphetamine, and 4-Fluoramphetamine (4FA).6,7 Despite preventive measures, such as drug test stations, social media education, controlling environmental factors during festivals (chill out areas), providing free drinking water, and first aid stations (FAS), 8 severe drug-related complications and even deaths occurred during previous events.9-11 In combination with the increasing drug concentrations, ADE 2016 and similar large EDMF are expected to cause an increased demand on emergency medical services due to increased recreational drug related complaints (RDRC), including sympathomimetic symptoms, like agitation, anxiety, hyperthermia, hypertension, and multi organ failure.12,13 Nevertheless, little is known about the impact on acute health services during EDMF. This is important information to improve harm reduction and prevention and to estimate if additional medical personnel are required during ADE or similar events. This is specifically relevant considering ED crowding and limited ED capacity, 14 especially since current predictive models are inaccurate for planning ambulance transfer rates. 15
The aim of this study was to evaluate the impact of recreational drug-related complaints at first aid stations, ambulance services and emergency departments during ADE 2016 compared to regular weeks, and to evaluate the requirement for additional medical personnel. The hypothesis was that recreational drug-related complaints will be significantly higher during ADE, compared to the control weeks, requiring additional medical personnel.
Methods
Study type and participants: In this prospective observational study, all patients, >12 years old, with RDRC at first aid stations (FAS) of Event Medical services (EMS) and the 4 largest emergency departments, 2 academic level I trauma centers (AUMC) and 2 locations of the largest regional teaching hospital (OLVG) in Amsterdam, the Netherlands, between October 19th 8 am and October 24th 8 am 2016 were included. Additionally, retrospective data from ambulance Amsterdam (AA) was collected for the same population in this period.
Data collection procedure and sampling method: The Dutch institute for medical aid in the region, determined the number of permitted visitors per site where EMS was present. EMS, the biggest provider of FAS, is staffed with advanced life support skilled staff and able to monitor and treat non-severe recreational drug-related complaints. EMS medical staff recorded all patients with recreational drug-related complaints (RDRC). AA is the only ambulance service in Amsterdam, and serves a region with approximately 1.2 million inhabitants. All dispatches are recorded by paramedics, but the extent of information recorded depends on the amount of care that was provided. Records involving the use of recreational drugs, based on the preliminary diagnosis recorded by paramedics, were included in the database by an investigator (PG). At the EDs, all patients with RDRC as presenting complaints or diagnosed by the physician, were included in the toxicology database by the treating physician and additionally cross-referenced with the term “intoxication” in the Dutch computerized Diagnosis and Treatment Combinations system, a nationwide system used for reimbursement of medical care, by an investigator (PG). Two other, smaller, Amsterdam hospitals were not involved in the study because they rarely see patients with RDRC. From OLVG and AA, a control group was included of patients >12 years old presenting with RDRC to OLVG or AA 2 weeks before and after ADE. In order to evaluate the increase in RDRC this control group was compared to the OLVG and AA included patients with RDRC during ADE, the ADE group.
Variables and definitions: Medical chart review to obtain patient demographics and recreational drug(s) use was performed for EMS patients. For ED patients, additional information was collected including hospital admissions, length of ED and hospital stay, and mortality. For AA all these data were collected when available. Patients without a current permanent Dutch address were defined as tourists. An acute intoxication was defined as any complaint, diagnosed by the treating nurse or physician, related to the ingestion, injection or snorting of recreational drugs, like MDMA, 4FA, amphetamine, cocaine, new psychoactive substances, heroin, cannabis, psilocybin, gamma-hydroxybutyrate (GHB), ketamine, and/or alcohol. Poly-drug use was defined as the use of 2 or more of the above-mentioned substances. Recreational drug use was self-reported, information retrieved from witnesses, or based on available analytical information, like urine toxicology screening results. Patients presenting more than once within 24 hours, with the same complaint, were only included once.
Data Processing, statistical analysis and sample size: Castor (www.castoredc.com) was used to store patient data anonymously. Data was analyzed with IBM SPSS statistics version 22. Descriptive statistics were presented in frequencies (%) for categorical variables, and median (interquartile range [IQR]) or mean (standard deviation, SD) for continuous variables. Comparisons of proportions were made using the chi-squared test. A Bonferroni correction was used in order for a pairwise comparison to be made. The sample size was a convenience sample where all available patients were included. P-values of P < .05 were considered statistically significant.
Ethical approval: This study was approved by all 4 participating hospitals institutional ethical boards (WO-number 16.568). Since it involved the processing of anonymous data collected for medical purposes, no informed consent was required.
Results
Based on ticket sales, ADE organizers estimated a total of 375.000 visits (not unique visitors) during ADE 2016. EMS was present at 40 of the large-scale dance events with an estimated total of 201.850 visits, 54% of all ADE visitors. The number of RDRC at EMS, AA, and EDs is shown in Figure 1. Demographic data for EMS and ED patients are shown in Table 1.

Amount of patients with recreational drug-related complaints in the acute healthcare chain.
Demographic information.

Abbreviations: EMS, Event Medical Services; ED, emergency department.
At EMS, a total of 609 patients were seen including 459 with RDRC, of which 243 (53%) were male and 139 (30%) tourists, with a mean age of 24 years old (range 12-64). Poly-drug use was reported for 315 patients (69%) of which 104 (33%) tourists. 75% (n = 103) of all tourists, compared to 66% (n = 211) of Dutch patients, presenting at EMS, used 2 or more substances including alcohol. The use of 3 or more recreational drugs was reported by 115 (25%) patients of which 46 (40%) were tourists. A total of 11 intoxicated patients (2.4%) were referred, and transported by AA to the ED.
During ADE the AA dispatched 986 times, of which 113 (12%) were due to RDRC (Figure 2). This represents a significant increase (P < .001) compared to the 2 weeks prior and after ADE where on average 51 patients per week were seen with RDRC. Poly-drug use was reported by 39 (35%) patients.

Proportion of recreational drug-related ambulance dispatches.
At all participating EDs, a total of 81 patients presented with RDRC. Sixty patients were male (74%), and 41 (51%) were tourists. The mean age was 28 years (range 14-72 years). Poly-drug use was reported by 47 (58%) patients of which 26 (55%) were tourists. Twenty-four (30%) patients had used 3 or more substances, and in 59% (n = 48) alcohol was the most frequently used recreational drug. Of all tourists, 26 (63%) reported the use of 2 or more drugs, compared to 21 (53%) Dutch patients. The total amount of ED visits at OLVG hospital during ADE was 971 of which 52 (5%) were due to RDRC (Figure 3). Again, this is a significant increase (P < .001) compared to the 2 weeks prior and after ADE where on average 22 patients per week presented with RDRC.

Proportion of recreational drug-related ED presentations at OLVG hospital.
The 81 ED patients cumulatively, have used recreational drugs 158 times of which 48 times alcohol, 34 times MDMA, 34 times marijuana and 17 times cocaine (Figure 4). Of all ED patients, 90% (n = 73) were discharged home and 8 (10%) were admitted, half of which were tourists.
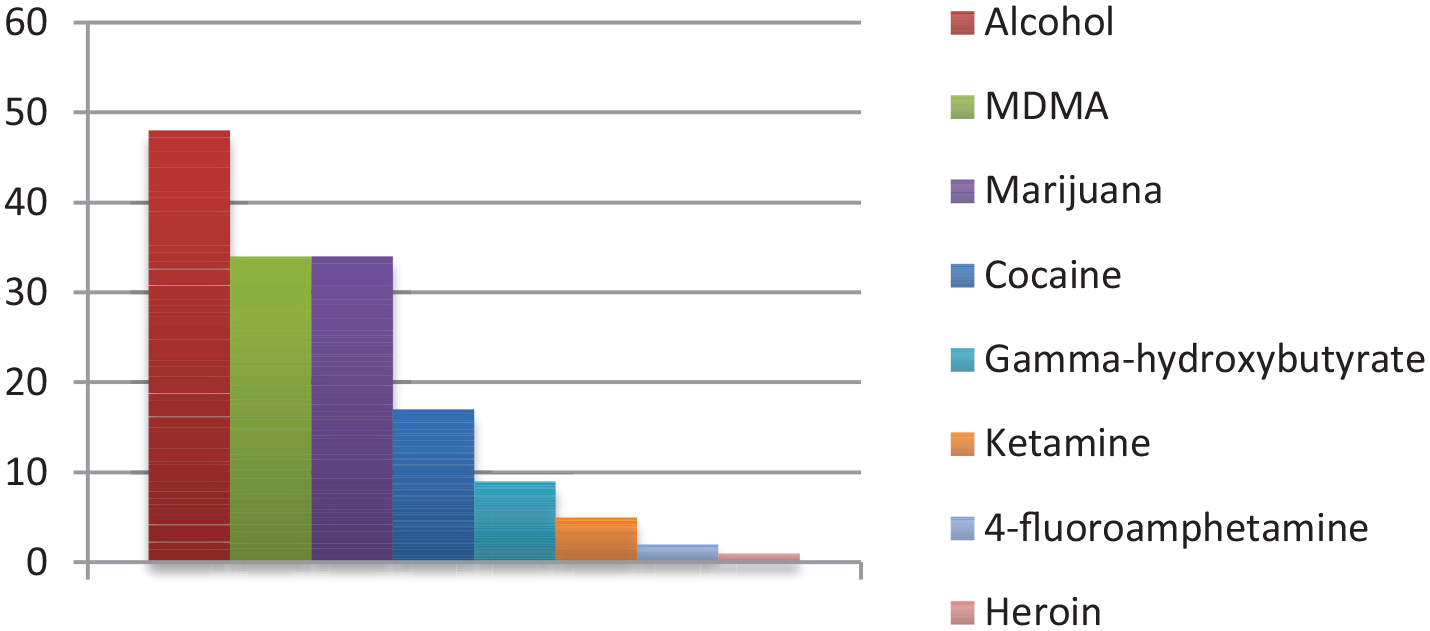
Recreational drugs taken by patients who presented at the EDs.
Average ED length of stay was 3.45 hours (range 0.25-13.25). Four patients (5%, n = 3) were transferred to the intensive care unit (ICU). One agitated patient had received a high dose of sedatives in the ambulance and was admitted for observation due to a lack of medium care beds, and was discharged within 8 hours. The other 3 ICU patients were intubated for airway protection, due to a low Glasgow coma scale score. They were discharged after 7, 21, and 34 hours. No deaths occurred during the study period.
Discussion
In this observational study we demonstrated that 81 ADE visitors (out of 375.000 attendees) presented with RDRC at Amsterdam EDs, leading to a minor strain on the acute health care system.
It is known that recreational drugs are widely used at EDMF with a potential strain on acute healthcare services.2,3,12,13 This is partly due to increased recreational drug dosage1,2 and due to serious drug-related complications during previous ADE editions,9-11 recreational drug use during large scale EDMF remains an important topic among healthcare professionals and the general public in the Netherlands. A previous study found that 33.5% of all EDMF attendees experienced a drug related adverse event in that past year. 16 Another study found that 160 out of 487 (33%) FAS encounters were RDRC, 17 which is much lower than the 459 out of 609 (75%) patients seen at EMS. Suggestion that recreational drug use is common during ADE.
One study reported a higher percentage of males and younger EDMF attendees (18-24 years old) reporting an adverse drug event. 16 This is comparable with our study, although the percentage of male patients at EMS was only 53%, comparable with the 51% reported by Friedman et al. 12 Additionally, Palamar et al 16 found a higher risk for adverse drug events in attendees with a college degree, suggesting that prevention information should specifically be aimed for young attendees with a college degree.
Tourists are over-represented at the EDs (51%) in our study, since at EMS only 30% of encounters were tourist. This difference is expected to be due to lack of recreational drug knowledge and difficulty accessing preventative information. Although we did not have exact data regarding the number of tourists visiting ADE and their recreational drug use, it is known that of all 5.3 million Amsterdam tourists in 2014, 8% visited clubs and raves, 18 which makes this a relevant group for the local government to address since preventive measures mostly target Dutch citizens.
In a previous study 67.8% of the EDMF attendees reporting a last year adverse drug event, alcohol use was reported. 16 Previous ED and FAS studies have shown that poly-drug use is common among recreational drug users.13,19-21 In this study, a much higher percentage of poly-drug use among ED patients (58%) was found, compared to FAS patients (25%). This suggests that poly-drug use causes more serious complications.
When FAS with high level of care like EMS were present at the EDMF, a decreased amount of ambulance transfers to EDs were reported. 22 Our study subscribes this, since EMS only referred 2.4% of their intoxicated patients to the ED. Interestingly, Munn et al reported an even lower ambulance transfer rate of 0.93% of patient encounters at FAS, however their nearest ED was 52 km (33 mi) from the EDMF, which might affect the decision to transfer the patient to an ED. 23 Nevertheless, this suggests that FAS equipped with higher level of care, combined with preventative measures like outreach teams, education, pill checking facilities, reduce Ambulance and ED burden. 23
Although the number of intoxicated patients increased by 225% at AA and by 236% at the OLVG EDs, the absolute number of patients stayed within the normal range of AA and ED capacity. Nevertheless, a previous study at a comparable sized ED like OLVG, did prepare with additional nursing staff for a 3-day EDMF that was equipped with FAS. 5 They reported an additional 28 patients, 25 after substance abuse, and admitted 3 patients with substance abuse complications, suggesting this was within normal capacity of an ED with >50 000 patients annually. However, the relatively long length of stay (225 minutes), 11 which was comparable to the previously reported median LOS of 216 minutes [IQR 210-347], might increase the mostly nocturnal workload at the ED. 5
Limitations
This study was conducted in a country with a liberal recreational drug policy; therefore, the results of this study may not be generalizable to other countries. Possibly, the amount of RDRC was underestimated, due to the fact that recreational drug use was identified by self-report or reported by witnesses. Analytical confirmation was rare. Also, the 2 small Amsterdam EDs might have treated self-presenting RDRC patients, not included in the study, however, it is expected this will be a limited number of patients. Furthermore, the total amount of tourists visiting the ADE is unknown. Besides this, patients with recreational drug-related trauma were most likely missed, therefore this study does not provide any information on indirect harm.
Conclusion
During ADE 2016, the largest 5-day indoor dance event in the world with 375 000 visits, 459 patients with RDRC presented to FAS, 113 to ambulance service and 81 to the ED. A higher percentage of poly-drug use among ED patients (58%) was found, compared to FAS patients (25%), and the proportion of tourists in the ED (51%) was higher compared to FAS (30%). Eight patients were admitted to the hospital, without any deaths recorded.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed to the development of the research protocol, inclusion of patients and writing of the manuscript. All authors have read and approved the manuscript.