
Abstract
Introduction
The North Shore Rescue (NSR) Advanced Medical Provider (AMP) program is composed of physicians and nurses based in North Vancouver who attend high acuity medical search and rescue (SAR) callouts in British Columbia, Canada. This study aimed to analyze the medical care provided by AMPs with appropriate comparisons to non-AMP callouts.
Methods
A retrospective review of all NSR callouts from January 1, 2018, to December 31, 2022, was conducted. The analysis included AMP involvement, rescue logistics, subject demographics, activity, primary cause, provisional diagnosis, treatments, medical decision-making, and extraction means. National Advisory Committee for Aeronautics (NACA) scores were assigned by physicians to evaluate medical acuity as well as under-triage and over-triage.
Results
Of the 767 NSR callouts over the 5-year span, 283 (37%) were medical, and of these, 35% (n = 99) involved AMPs. Seventy-five percent of AMP rescues involved traumatic injuries, and 31% involved nontraumatic medical illnesses. The mean NACA score for AMP callouts was significantly higher than non-AMP callouts (3.1 ± 1.3 vs 1.9 ± 1.3, p < .00001). Medications were administered in 40% of AMP rescues, procedures were performed in 54%, and 37% involved advanced medical decision-making. Over-triage occurred in 33% of AMP callouts, with under-triage in 10%.
Conclusions
The AMP program provides a useful service when advanced medical care in wilderness environments is needed. AMPs coordinate appropriate medical response and ensure safe, comfortable, and efficient transport to definitive care. The NSR AMP program may act as a model for the development of similar programs by other SAR teams.
Keywords
Introduction
The complex mountainous terrain, prominent outdoor tourism industry, 1 and vast, sparsely populated regions make wilderness medical response a necessary component of prehospital care in the Canadian province of British Columbia (BC).2–4 Despite this, wilderness medical response is an evolving domain that is region-specific, with multiple organizations of differing levels of medical training potentially responding.4,5 This is in contrast with Europe6–13 and Australia,5,14 where well-established prehospital rescue teams staffed with highly trained paramedics and physicians are the standard of care in similar terrain.
The designated providers of prehospital care in BC are paramedics and emergency medical responders employed by British Columbia Emergency Health Services (BCEHS), which provides both ground and air response.3–5,7 Professional firefighters, trained as first responders, also offer ground response and administer first aid and basic life support before BCEHS arrival.3,15 Both organizations face limitations in wilderness and/or mountainous terrain due to constraints in vehicle and helicopter accessibility and regulations, which limit these prehospital care providers’ ability to perform “medical rescue” in hazardous wilderness settings.4,5,16 In these technically challenging situations, BCEHS often requests the support of ground search and rescue (GSAR) volunteers who are capable of conducting wilderness rescues and providing high-quality basic medical care.17–19 However, since there is no requirement for GSAR volunteers to have advanced medical training, 5 this leaves a gap in care for patients requiring advanced medical care in wilderness and remote areas in BC.4,7
GSAR is largely performed by volunteer organizations in Canada. The vast majority of remote wilderness medical response falling outside the scope of designated professional prehospital care providers in British Columbia is tasked to the 78 government-subsidized volunteer GSAR teams overseen by the BC Search and Rescue Association and the BC Ministry of Emergency Management and Climate Readiness (EMCR).17–20 The Canadian Armed Forces (CAF),21,22 Parks Canada,23,24 and privately funded Helicopter Emergency Medical Services (HEMS)25,26 contribute much less frequently and are activated only under specific circumstances.5,19 The CAF utilizes military-trained search and rescue (SAR) technicians,21,22 Parks Canada employs mountain safety specialists,23,24 and private pay-for-service HEMS teams consist of paramedics, physicians, nurses, and technical rescue specialists.25,26 In contrast, GSAR teams are composed of volunteers who have completed at minimum a 100-h GSAR course and Basic First Aid with no formal mandate for advanced medical training. 5 Although made up of volunteers, GSAR teams are highly trained and organized and do not charge a fee for their services. 17
North Shore Rescue (NSR) is one of 78 independent volunteer SAR teams overseen by the BC Search and Rescue Association, which provides 24/7/365 coverage for 480 km2 of rugged mountainous terrain that is easily accessible from downtown Vancouver and is the busiest SAR team in Canada. 27 A prior study of NSR callouts found that 41 percent involved medical incidents, and approximately half of these rescues required acute intervention beyond the level of basic first aid. 27 These high-acuity rescues typically occur in complex mountainous terrain, which characteristically involves prolonged prehospital times.6,13,27 Due to the complexity of medical care and the technical nature of these rescues, NSR established the Advanced Medical Provider (AMP) program in 2018, the first civilian program of its kind in Canada, dedicated to providing advanced medical care in wilderness environments using a volunteer SAR platform. This specialized AMP team currently comprises 9 emergency physicians, 2 anesthesiologists, and 1 emergency nurse, all with previous experience in wilderness environments. Two AMPs are full, regular NSR team members, and the others, who are considered formal “resource members,” do not require GSAR training but receive basic SAR training provided through NSR. AMPs are part of a call response group and are selectively activated based on NSR Medical Advisory Committee Guidelines (Table 1), ensuring their response to medical rescues requiring advanced medical knowledge and skills. When deployed by air, AMPs are typically integrated into a crew composed of a helicopter pilot and full NSR team members with additional air-operations training to perform technical patient extractions and transport in accordance with the optimal air rescue crewmember concept established by the International Commission for Mountain Emergency Medicine. 10
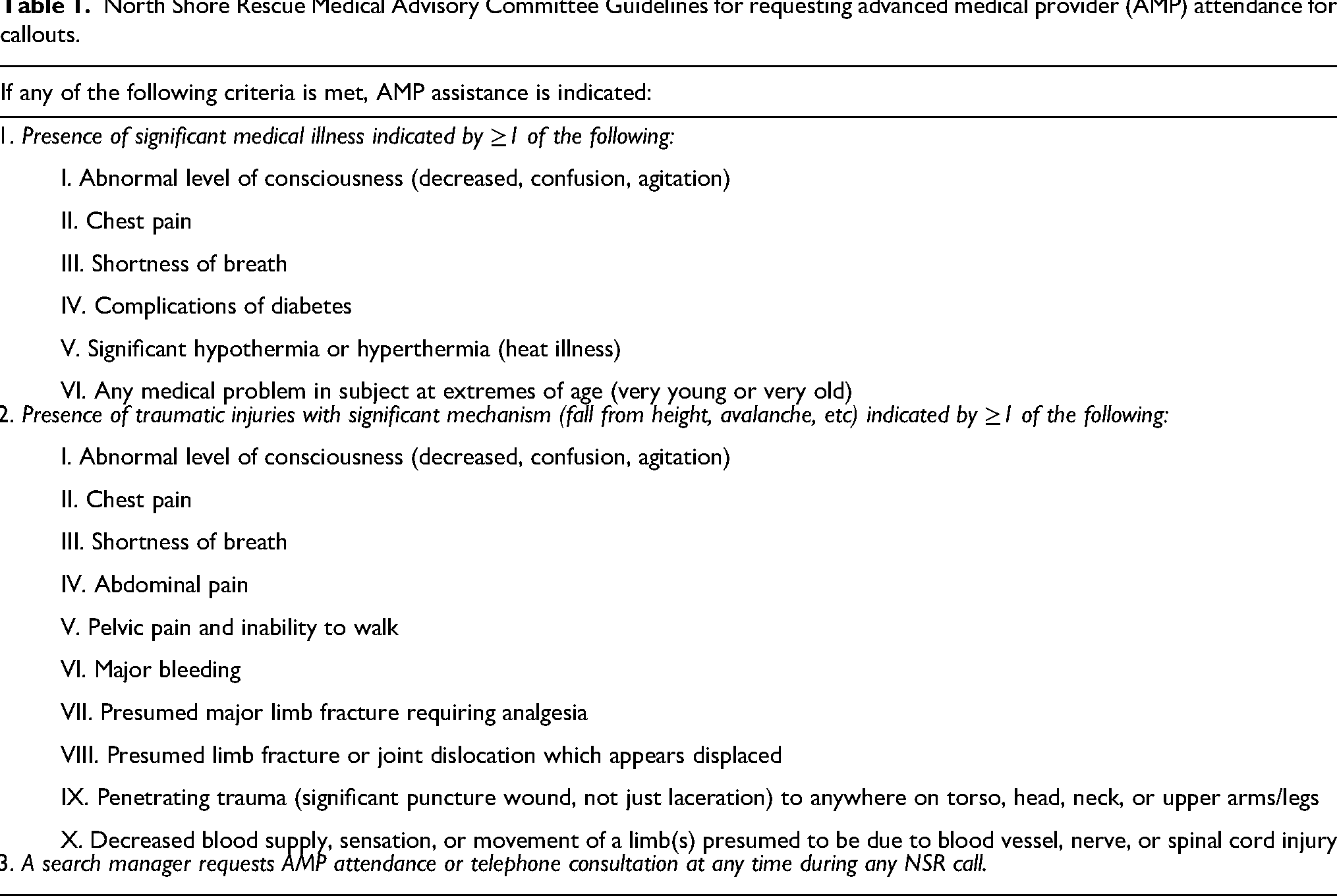
North Shore Rescue Medical Advisory Committee Guidelines for requesting advanced medical provider (AMP) attendance for callouts.
Through our review of all NSR callouts over the first 5 years of the AMP program, we aim to delineate the clinical and logistical aspects of medical calls and to highlight the similarities and differences between callouts attended by the NSR AMP program members in contrast to those not attended by AMPs.
Methods
We conducted a retrospective review and descriptive analysis of all NSR incident report (IR) documentation from callouts that occurred during the 5-year period between January 1, 2018, to December 31, 2022. Details about the mission objective, events, subject demographics, and outcome of the rescue are recorded in each IR and are stored on a secure online database.
Each IR was reviewed manually and determined to be medical or nonmedical using inclusion criteria based on previous research 27 (Online Table A1). For each medical callout, information pertaining to the rescue characteristics, subject demographics, and features of medical care were extracted and encoded into an encrypted data collection sheet in Microsoft Excel. For AMP rescues, the AMP who oversaw medical care and decision-making was also interviewed to supplement information gathered from each respective IR. No direct subject-identifying information was recorded.
Data collected included the date of the callout, whether it was a mutual aid callout (NSR assistance requested by another SAR team), the subject's age and sex, activity at the time of the incident, the primary cause of incident, use of a helicopter, method of subject extraction, AMP involvement, provisional diagnosis, medication used (including dose and route), medical procedures performed, and medical decision-making. Advanced medical decision-making was defined as a medical decision made by an AMP to improve patient care that would not have been made by a non-AMP team member due to their lack of advanced medical training, knowledge, and authority. An example of this would be possessing sufficient medical knowledge and authority to recognize when the transport of a patient should bypass a smaller local hospital and go directly to a hospital capable of providing definitive care.
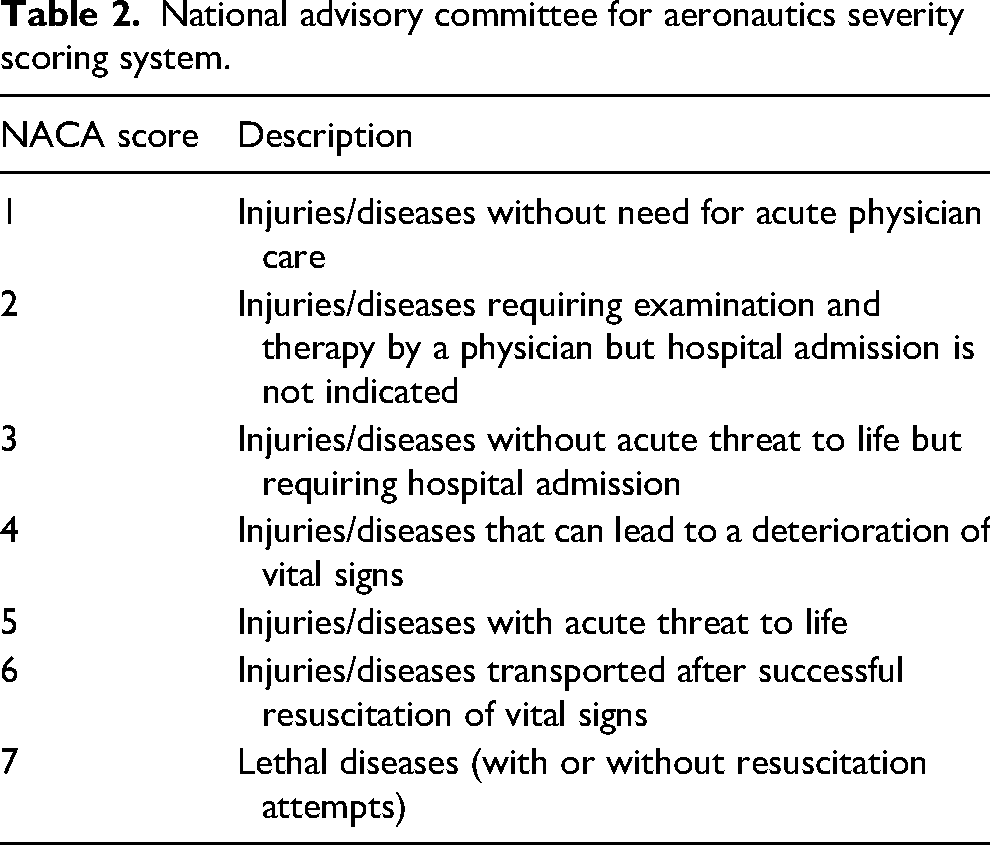
The severity of a subject's medical condition was described using the National Advisory Committee for Aeronautics (NACA) severity scoring system, a well-validated prehospital tool for predicting morbidity/mortality and the level of care required (Table 2).9,28 Each medical rescue was reviewed independently by 3 experienced attending physicians (AR, MC, MT), and the patient was assigned a NACA score. A score was selected when 2 or more reviewers agreed. Where differences in all 3 scores existed, a consensus decision was made by the panel of physicians.
National advisory committee for aeronautics severity scoring system.
Severity scores were used to judge whether callouts were under and over-triaged. Over-triage was defined as AMP involvement on a callout where the NACA score was ≤2, whereas under-triage was defined as no AMP involvement when the NACA score was >2. Rescues where the NACA score was 7 (death) were excluded if the subject was known to be deceased or if a medical issue was not suspected at the time of callout (for example, inadvertently finding a missing subject to be deceased).
All data collected was analyzed using the Microsoft Excel Analysis ToolPak. Descriptive statistics were calculated to summarize rescue characteristics, subject demographics, and features of medical care. Differences in categorical data between AMP and non-AMP medical rescues were analyzed using a Chi-square test. For comparing numerical data between AMP and non-AMP medical rescues, an F-test was first used to determine parametricity, and since all data was parametric, subsequent analysis applied a Student's t-test. Statistical significance was achieved by applying an alpha ≤0.05 for the lowest p-value. To reduce the risk of a type I error (false positive) due to repeated comparisons, the Holm-Bonferroni method was applied to subsequent p-values.
This project was reviewed and approved by The University of British Columbia Clinical Research Ethics Board (No. H23-00380).
Results
Subject Demographics
The mean age of subjects for AMP rescues was 41.2 ± 16.0 (range 9 to 74) years, and for non-AMP rescues, it was 45.4 ± 21.8 (range 7 to 95) years (Online Table A2). When sex was specified, males constituted 59% (n = 58) of AMP rescues and 41% (n = 76) of non-AMP rescues. Females accounted for 39% (n = 39) of AMP rescues and 42% (n = 78) of non-AMP rescues. Sex was unspecified in 2% (n = 2) of AMP rescues and 16% (n = 30) of non-AMP rescues.
Activity and Primary Cause
Hiking was the most common activity, constituting 67% (n = 66) of AMP rescues and 68% (n = 126) of non-AMP rescues (Online Table A2). Snow sports, which included backcountry skiing/snowboarding, snowshoeing, and snowmobiling, were the second most frequent activity for AMP rescues (17%, n = 17). In non-AMP rescues, wandering (non-goal-directed walking typically exhibited in subjects with neurocognitive impairments) was the second most common activity at 14% (n = 26), while no AMP callouts were for this reason. Mountain biking, climbing, watersports, and other activities combined constituted less than 14% of both AMP and non-AMP rescues. Rescues without a specific definable activity made up 3% (n = 3) of AMP rescues and 5% (n = 10) of non-AMP rescues.
The primary cause for the majority of AMP rescues was slips or falls, constituting 62% (n = 61) of all callouts. Nontraumatic medical illnesses, including physical, psychiatric, substance-related, and environmental exposure-related conditions, accounted for 26% (n = 26) of AMP rescues. In contrast, non-AMP medical callouts were primarily driven by nontraumatic illness, representing 46% (n = 85) of cases, followed closely by slips or falls at 42% (n = 78).
Rescue Characteristics
Over the 5-year period (2018–2022), NSR recorded 767 callouts, with 293 (38%) meeting inclusion criteria (Online Table A1). Ten callouts (3%) were excluded due to insufficient documentation, inability to locate a subject, service cancellation, or AMP deployment for team member safety, leaving 283 (37%) medical callouts for further analysis. Of the 283 medical callouts, 99 (35%) were attended by AMPs. During callouts, AMPs were primarily involved in field operations (87% of rescues, n = 86) while offering telephone support (9%, n = 9) or on active standby (4%, n = 4) in a smaller proportion of rescues. The number of AMP personnel on callouts varied from a minimum of 1 to a maximum of 4, with a median of 1. Over the 5-year period, the median number of callouts attended for an individual AMP was 9.5 (range 4 to 45). Mutual aid requests represented 24% (n = 24) of all AMP callouts, which was significantly more than the 13% (n = 24) of non-AMP callouts (χ2 = 5.7, p = .0167). Helicopters were used significantly more during AMP callouts (86%, n = 85) compared to non-AMP callouts (45%, n = 83) (χ2 = 44.3, p < .00001). The methods for extracting subjects via helicopter were categorized into two groups: cabin extraction, which includes both hover entry and helicopter landing, and Class D. As per Transport Canada Aviation Regulations, Class D helicopter rescue is used to define both fixed line and hoist/winch rescue operations. 29 In AMP rescues, the most common method of subject helicopter extraction was Class D, which accounted for 61% (n = 60) of all rescues and was significantly higher than cabin extractions (15%, n = 15) (χ2 = 14.9, p < .0001). Class D extractions were also significantly more prevalent in AMP rescues (61%, n = 60) when compared to non-AMP rescues (27%, n = 49) (χ2 = 31.4, p < .0001).
Diagnoses
For AMP medical rescues, 75% (n = 74) involved traumatic injuries, while 31% (n = 31) involved nontraumatic medical illnesses, with 6% (n = 6) having concurrent traumatic and nontraumatic medical conditions. The most frequent traumatic injury diagnoses were polytrauma (18% of total AMP rescues, n = 18), lower limb fractures (15%, n = 15), lower limb soft tissue injuries (8%, n = 8), and spinal injuries (8%, n = 8) (Figure 1). Regarding nontraumatic medical illnesses, cardiovascular issues were the most common (8%, n = 8), followed by environmental exposure (hypothermia or heat illness) (7%, n = 7) and mental health issues (6%, n = 6) (Figure 1).
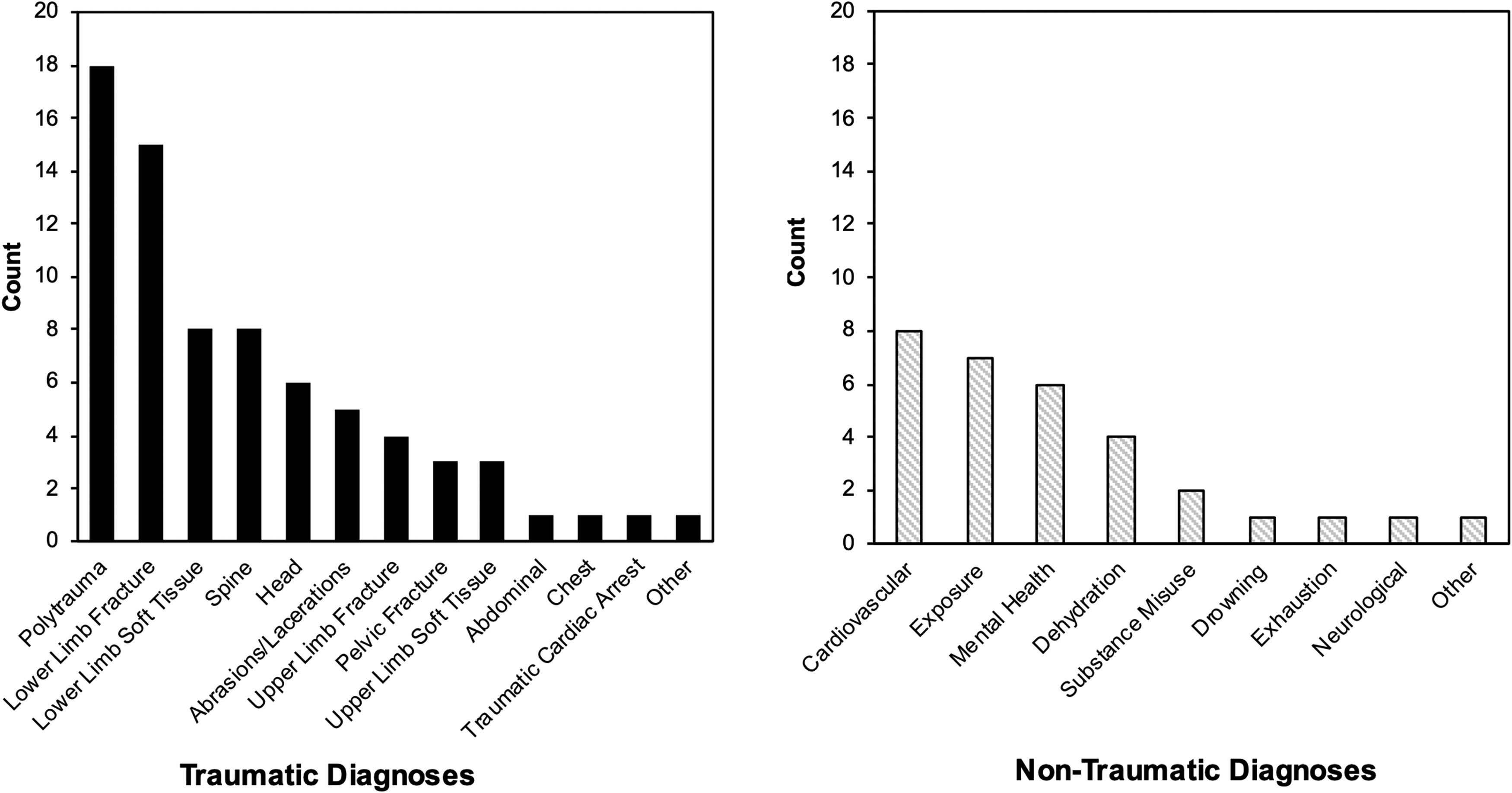
Traumatic and nontraumatic diagnoses given by AMPs.
The mean NACA score for all AMP rescues was 3.1 ± 1.3, significantly higher than the mean score of 1.9 ± 1.3 for non-AMP rescues (p < .00001) (Figure 2). Based on NACA scores, over-triage of AMP attendance at callouts was judged as 33% (n = 33), and under-triage was judged as 10% (n = 10).
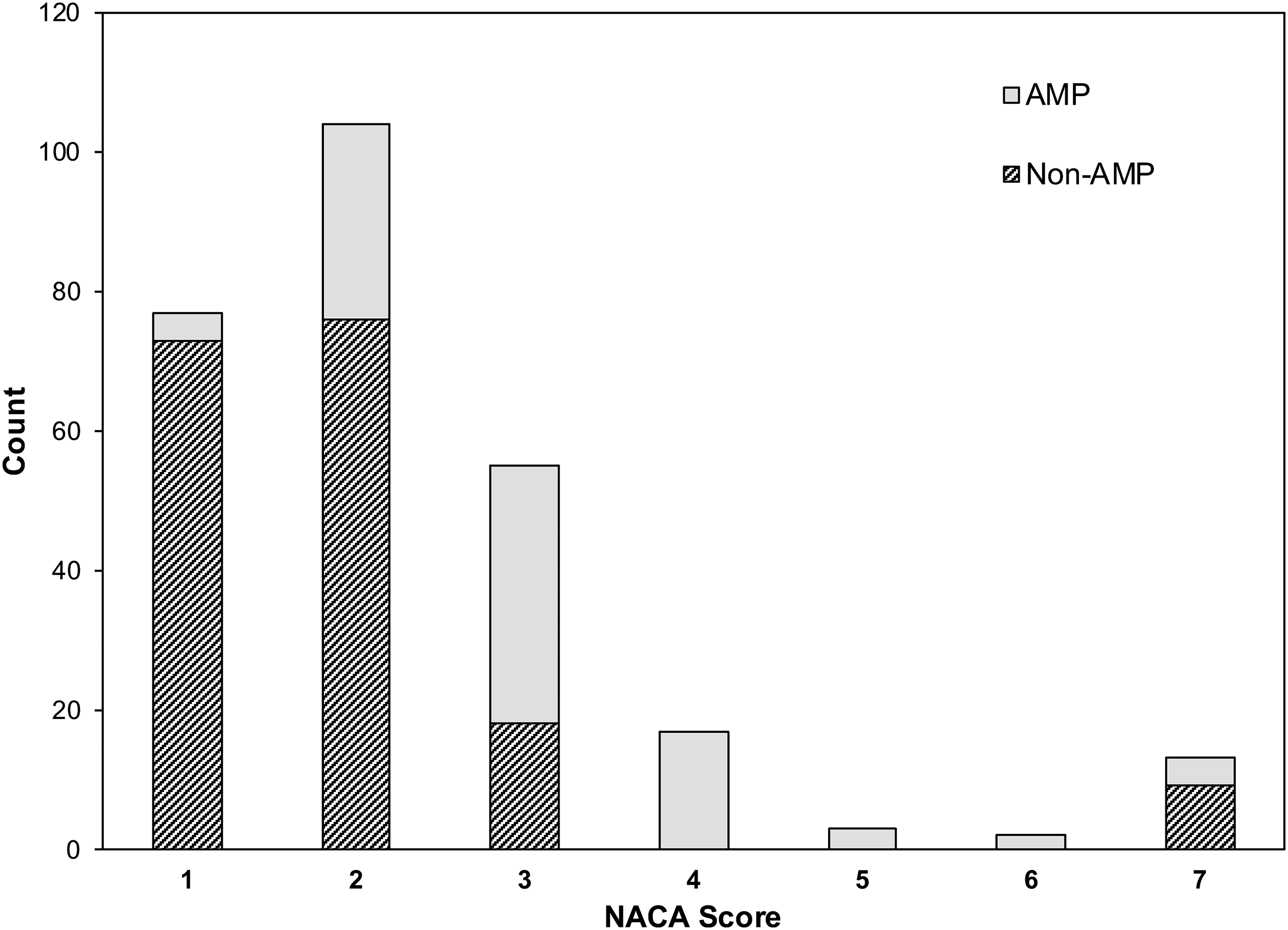
NACA scores of AMP and non-AMP callouts.
Treatments and Medical Decision-Making
Among AMP rescues, 40% (n = 40) involved the administration of medications. The most commonly administered were fentanyl (13% of medications, n = 10), dimenhydrinate (13%, n = 10), ketamine (12%, n = 9), morphine (9%, n = 7), inhaled methoxyflurane (9%, n = 7), and intravenous (IV) normal saline (9%, n = 7) (Figure 3).
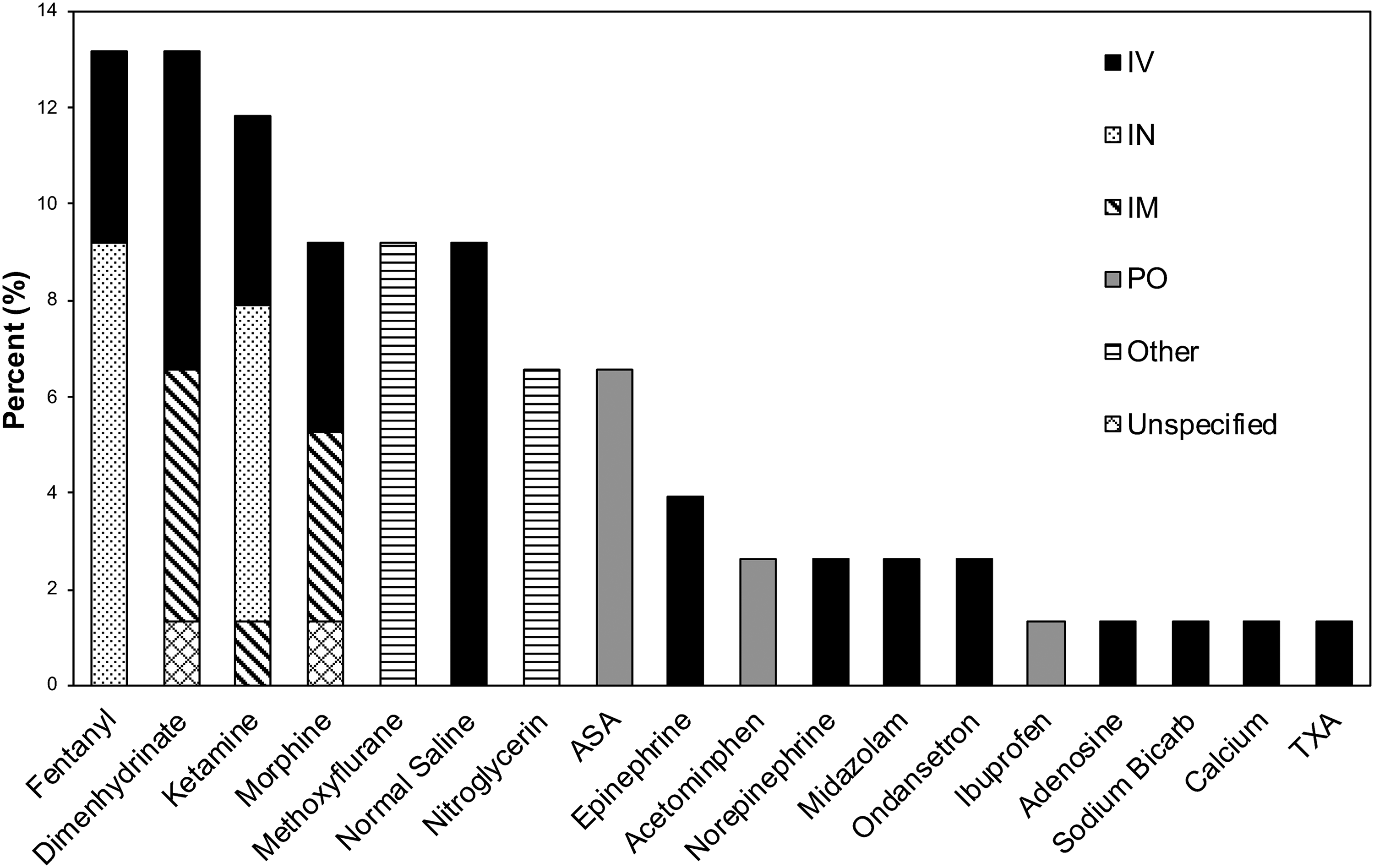
Summary of medications administered during AMP rescues.
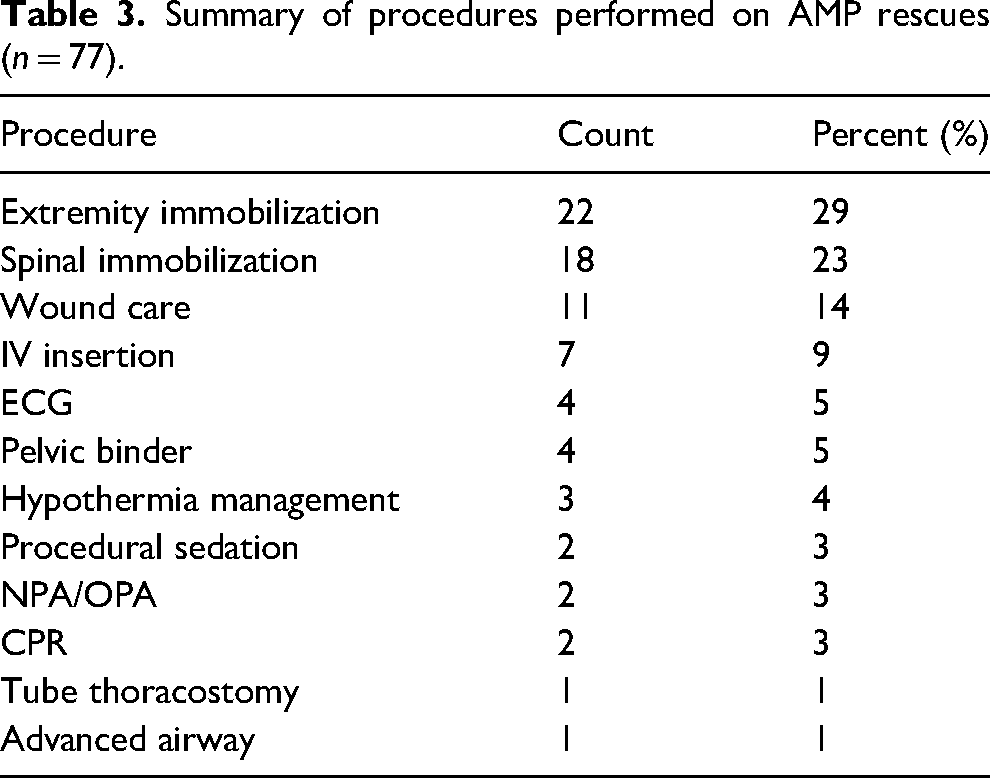
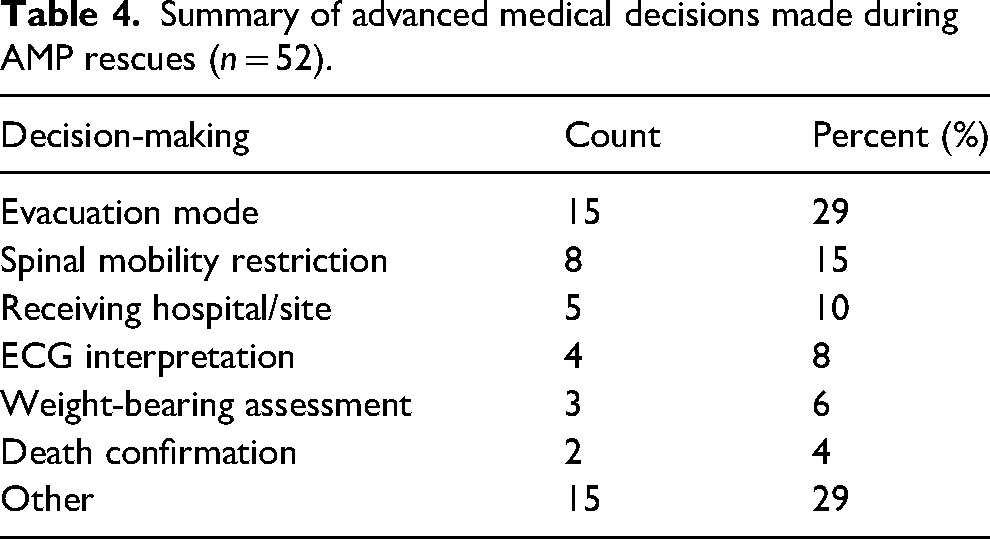
Procedures were performed in 54% (n = 53) of AMP rescues with extremity immobilization (29% of procedures, n = 22), spinal immobilization (23%, n = 18), wound care (14%, n = 11), and IV access (9%, n = 7) being the most frequent (Table 3). Furthermore, 37% (n = 37) of AMP rescues involved advanced medical decision-making with mode of evacuation decision-making (29% of decisions, n = 15), spinal motion restriction decision-making (15%, n = 8), and receiving facility transport choices (10%, n = 5) being the most common (Table 4).
Summary of procedures performed on AMP rescues (n = 77).
Summary of advanced medical decisions made during AMP rescues (n = 52).
Discussion
Preexisting literature on emergency medical care in wilderness settings by a dedicated advanced medical team has been more extensively studied in Europe6–13 and Australia,5,14 where more homogenous HEMS rescue teams staffed with medical professionals are the standard of care. This study provides valuable insight into prehospital emergency medical care in wilderness settings in North America by analyzing the demographics, clinical care, and rescue logistics for medical SAR calls attended by a volunteer SAR advanced medical team. Our study also compares callout characteristics between calls attended by AMP versus non-AMP NSR team members.
In our study, middle-aged men (AMP 41.2 ± 16.0 years, non-AMP 45.4 ± 21 years) were the most common demographic to need rescue. These findings are generally consistent with previous studies conducted in North America.19,24,27,30 In contrast to trends seen in some mountainous regions in Europe where the leading activities requiring rescuer-response are skiing 12 and climbing, 8 we found that the most common activity leading to medical rescue was hiking, which is generally congruent with previous research conducted on SAR epidemiology in North America.19,24,27,30,31 The leading cause for requiring rescue in AMP callouts was slips and falls (62%), which was also consistent with previous literature.6,8,19,24,31 However, non-AMP rescues exhibited the unique trend of having nontraumatic medical illnesses as the leading primary cause. This is explained by the high proportion of mental health and mild hypothermia callouts that NSR responds to, as current team guidelines (Table 1) do not have either of these reasons indicated as criteria for AMP activation. 27 It was found that traumatic injuries accounted for the majority of AMP rescues (75%) in comparison to nontraumatic medical conditions (31%), with a small proportion (6%) having concurrent traumatic and nontraumatic medical conditions. This distribution aligns with previous studies in North America19,24,27,30,31 and Europe.8,11,12
Analysis of injury/illness acuity yielded interesting results. NACA scores between AMP and non-AMP rescues differed significantly (3.1 ± 1.3 vs 1.9 ± 1.3, p < .00001), indicating that AMPs typically respond to higher acuity medical rescues. This is supported by our finding that polytrauma was the most common traumatic condition (18% of total rescues) encountered in AMP rescues, and cardiovascular conditions were the most common nontraumatic medical illnesses responded to by AMPs (8%). The injury severity seen during AMP rescues is similar to those observed in mountain rescues conducted by professional mountain rescue HEMS teams.8,9,12 In one study that analyzed 1137 alpine air rescues in Switzerland, it was found that 70% of physician-attended rescues were NACA 3. 12 Another study that analyzed 1533 rescues over 11 years conducted by the Royal Norwegian Air Force's anesthesiologist-staffed, 330-Squadron SAR helicopter service found that most patients requiring medical rescue had a NACA score of 3 or 4. 9 The higher prevalence of NACA 7 scores in non-AMP rescues can be explained by NSR's involvement in body recoveries and missing person searches. In these callouts, the subject is either known or presumed deceased thus AMP activation is not indicated.
In prehospital trauma settings, it is generally accepted that under-triage should be ≤ 5% and over-triage should range from 25% to 35% to ensure optimal resource utilization and medical care. 32 Thus, the amount of over-triage (33%) and under-triage (10%) observed within the AMP program suggests that NSR Guidelines (Table 1) generally function well but could be modified to yield slightly increased AMP activation on callouts. 32 Additional engagement and consultation with search managers to gather pertinent medical information relevant to AMP activation could potentially lead to less under-triage.
Medications were used in 40% of AMP calls, with the most common medications given being analgesics (47% of all medications), followed by antiemetics (16%). Prior research also indicates that analgesia is the most common reason for medication administration by mountain rescue teams in Europe; however, its use was more frequent (53%–76% of all rescued patients) than in our study.6,12 Similar to European mountain rescue, the most common analgesics used were fentanyl and ketamine. 12
The most common procedures performed by AMPs were focused on patient evacuation and packaging, with extremity immobilization and spinal immobilization being the most frequent (Table 4). This is consistent with a North American study that found that extremity immobilization was the most common procedure performed by SAR responders on medical rescues. 30 Critical interventions (airways, cardiopulmonary resuscitation, and tube thoracostomies) were much less frequent, being performed on 3% of total AMP rescues. This can be compared to the findings of Pietsch et al, 12 which found that onsite emergency medical interventions (cardiopulmonary resuscitation, ventilation, rapid sequence induction, endotracheal intubation, chest tube insertion) had to be performed by physicians on 8% of mountain rescues in Switzerland. Advanced medical decisions were made in approximately one-third of AMP rescues (37%), with AMPs primarily making logistical decisions regarding appropriate patient evacuation mode, packaging, and selection of appropriate higher-level-of-care facility for transport. The medication usage, procedures, and decision-making highlight that the main role AMPs serve in medical rescues is to triage and prepare patients for safe and timely evacuation while coordinating appropriate transport to the hospital where they can receive definitive care.
Implications for SAR in North America
In BC, a large proportion of wilderness medical response occurs in mountainous terrain and patients often require care beyond the level of basic first aid. 27 The benefit of organized HEMS staffed with advanced medical personnel on improving medical care in mountain rescue6,10,12 and patient outcomes 33 has been well established in Europe.
Government designated professional HEMS organizations in Canada, such as BCEHS, have limitations that prevent response to wilderness/mountainous terrain. 4 These organizations do not conduct Class D helicopter operations that are necessary on many wilderness calls, and their guidelines prohibit medical personnel from conducting rescues in hazardous wilderness environments.4,5,16 Other government organizations such as Parks Canada and the CAF can conduct technical rescues and may perform some advanced medical care, but these organizations are primarily activated for incidents in national parks23,24 or non-GSAR incidents, respectively.21,22 Pay-for-service HEMS staffed with advanced medical personnel capable of technical rescues have been established in BC.25,26 These are few in number, not formally tasked by requesting government agencies to perform SAR operations and wilderness medical rescues, 18 and their call volumes and rescue details are not publicly available and thus unknown.
Eighty-six percent of AMP rescues utilized helicopters, and more than 60% of all AMP rescues involved Class D helicopter operations, enabling timely delivery of advanced medical care to patients who would otherwise be unreachable by BCEHS and would likely face prolonged wait times before reaching advanced level care. Thus, with adequate medical capabilities and access/egress proficiencies, SAR teams have the potential to fill the gap in prehospital advanced medical care that currently exists in British Columbia.
SAR teams in BC and elsewhere may consider developing or bolstering their advanced medical response programs based on the NSR model using physicians, nurses, and paramedics to respond to sicker patients. The medications and procedures most commonly used are familiar to emergency, anesthesia, and critical care physicians and nurses, as well as paramedics with advanced care training or higher. These providers would be most suited to fill medical roles on SAR teams. Anecdotally, the medical care provided by NSR AMPs during medical rescues decreases the stress felt by nonmedical NSR teammates, contributing to a calmer, smoother, and safer rescue operation. The guidelines for activation we defined in our study led to a reasonable level of under and over-triage, suggesting they were effective at targeting appropriate callouts for AMPs to attend, and these could be a framework for teams without call-selection criteria in place. The data in our study can be used to target the training of both general SAR members and AMPs for the most common injuries and illnesses.
Limitations
Hospital records were not used in this study, so diagnoses were based on the provisional diagnosis the attending AMP made during each rescue. Thus, our findings do not provide insight into the final patient outcomes and may have led to an under or over-estimation of the mortality/morbidity of rescues. Data for some patients was incomplete, and memory recall was used to supplement data in incident reports through unstructured interviews of the AMPs involved in the rescues.
Conclusions
This study quantifies the medical care provided by the NSR AMP program through an analysis of 5 years of data. The program serves to expedite advanced medical care to those injured and ill in the austere wilderness environments served by NSR, reducing patient suffering with timely analgesia and potentially decreasing morbidity and mortality. Other SAR teams in BC and elsewhere may consider developing or bolstering their medical response capabilities based on this model. Ongoing monitoring of the AMP program, continued application of evidence-based guidelines, and collaboration between different organizations may continue to improve wilderness medical response.
Supplemental Material
sj-pdf-1-wem-10.1177_10806032241282963 - Supplemental material for Emergency Medical Care Provided by North Shore Rescue Advanced Medical Providers
Supplemental material, sj-pdf-1-wem-10.1177_10806032241282963 for Emergency Medical Care Provided by North Shore Rescue Advanced Medical Providers by Foster T. Wynne, ASc, Matthew Turnock, MSS, MSc, MD, FRCPC, Michael Crickmer, BA, Bed, BMBS, FRCPC, and Alec H. Ritchie, BSc, MD, FCFP(EM) in Wilderness & Environmental Medicine
Supplemental Material
sj-pdf-2-wem-10.1177_10806032241282963 - Supplemental material for Emergency Medical Care Provided by North Shore Rescue Advanced Medical Providers
Supplemental material, sj-pdf-2-wem-10.1177_10806032241282963 for Emergency Medical Care Provided by North Shore Rescue Advanced Medical Providers by Foster T. Wynne, ASc, Matthew Turnock, MSS, MSc, MD, FRCPC, Michael Crickmer, BA, Bed, BMBS, FRCPC, and Alec H. Ritchie, BSc, MD, FCFP(EM) in Wilderness & Environmental Medicine
Footnotes
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.