
Abstract
Cigarette smoking has remained as the leading preventable cause of disease and premature death in the United States. It can lead to many adverse health consequences such as lung cancer, cardiovascular diseases, and respiratory diseases.1–3 In the United States alone, in 2015, more than 16 million individuals lived with a smoking-related disease. According to the estimates given by the 2014 Surgeon General’s report, the annual number of smoking-attributable deaths is around 480,000 and has stayed above 400,000 for more than a decade. 4 Besides mortality, smoking imposes a substantial financial burden on society. Smoking-attributable economic costs resulting from loss of productivity, premature deaths, and direct medical cost added up to around $300 billion over the 2009 to 2012 period.4,5 To private employers in the United States, a smoking employee costs an extra $5,816 per year, considering excess absenteeism, presenteeism, and lost productivity due to smoking breaks, excess health care costs, and pension benefits. 6
The primary focus of tobacco control policies in the United States has been to reduce the number of smokers. Reducing smoking prevalence can be achieved either by encouraging smokers to quit or by preventing nonsmokers from taking up the habit. Smoking cessation interventions aim at the first goal while smoking initiation interventions target the latter. Cessation programs can be divided into two categories: pharmacological and nonpharmacological interventions. Pharmacological interventions are those in which smokers take prescribed drugs to help with their nicotine withdrawal syndromes. Popular treatments include nicotine-replacement treatment, bupropion, and varenicline.7,8 Nonpharmacological interventions usually involve motivational interviews and counseling as well as cognitive behavioral therapy.9,10 Scholars have identified a few barriers for successful nonpharmacological interventions, including lack of social support, cultural norms, and stressful working/living situations.11,12 Initiation/prevention programs aimed at reducing the risk of youth becoming smokers. Some popular programs include cigarette taxation, mass media campaigns, and school-based education programs.13–16 Studies show that smoking initiation occurs during teenage and young-adulthood years, but is very rare after age 24 years.17,18 As a result, smoking initiation programs mainly target teenagers at school.
Smoking prevalence in the United States in 2015, after 50 years of smoking control efforts, has decreased to 15.1% from 43% in 1964. 19 To accelerate the eradication of the smoking epidemic, more efficient ways to implement smoking interventions are needed. Previous studies reveal that initiation and cessation programs are implemented and evaluated independently. Few studies look at the combined impact of multiple interventions targeting both initiation and cessation. The right combination of interventions could accelerate the process of reducing smoking prevalence while allocating limited resources efficiently. However, given the constant change of the environment in which these policies will act, there is a need to anticipate those changes and propose interventions that will adapt over time to this dynamic environment.
Optimization techniques, such as Optimal Control, can be useful in deriving appropriate solutions to this dynamic problem. Optimal control theory deals with problems of finding the paths of control variables that satisfy certain optimality criterion. In the context of dynamic models, the solutions represent a path for the control variables over time. Some scholars have applied optimal control theory to investigate empirical policies. For example, Juusola and Brandeau used optimal control to determine the best mix of investment in HIV treatment and prevention given a fixed budget. Their model maximizes the net present quality-adjusted life years. 20 Similarly, Basu and Kiernan investigated how financial incentives motivate health behavior changes by optimizing marginal return on investments. 21 When we deal with smoking policies, we can figure out the best combination of initiation and cessation programs over time to minimize prevalence given a budget constraint. To the best of our knowledge, we are the first study to adopt optimal control techniques to address the problem of reducing smoking prevalence over time while subjected to a budget constraint.
The organization of this article is as follows. First, we propose an optimal control dynamic model of ordinary differential equations (ODEs) and solve it analytically. Second, we identify and discuss an initiation and a cessation intervention to use as controls in the model. We then parameterize the model and solve it numerically for optimal trajectories. Finally, we present and discuss our results.
Methods
Theoretical Model
Based on previous work,22,23 we employ the following expression to represent the path of smoking prevalence over time:

where S(t) stands for the number of smokers in the population at time t, I(t) is the number of new smokers at time t, and
The original model has S and I as number of people while

where

is the time-variant smoking prevalence and

is the initiation rate. Because we assume M to be constant,

We can write the transformed Equation (1) as

Empirical policies are generally designed with a proposed goal and a budget constraint. To incorporate these characteristics, our model aims to minimize the overall toll of smoking prevalence over time, subject to a budget constraint. In order to construct a performance measure that takes both factors into account, we assign weights to these two aspects.
After defining our performance measure, we add some constraints to our model. Besides Equation (2), we have two more equations:
Now we are ready to write our problem in the mathematical form:
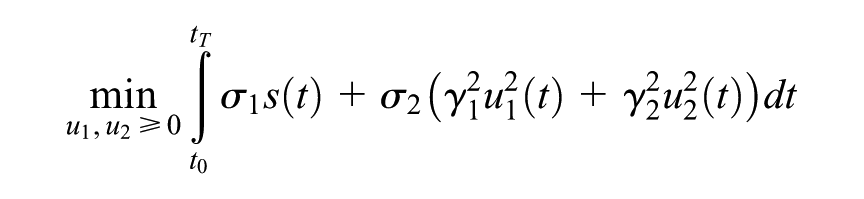
subject to
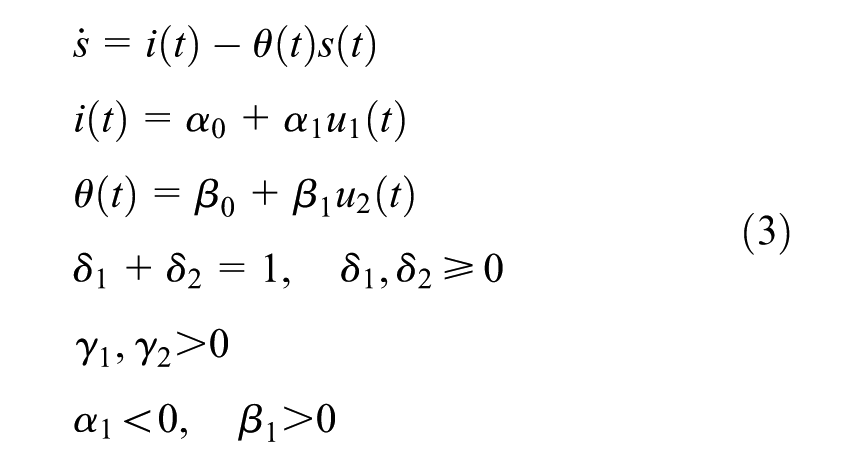
We can combine the first three constraints into one:

We choose to use the quadratic form for cost to penalize for extreme values. It is also a conventional form to represent cost in optimal control problems 24 . Then we can simplify the above problem into:

subject to

We obtain the augmented integrand function as

Using the Euler-Lagrange equation, 24 we derive the following set of necessary conditions for the optimal solution:
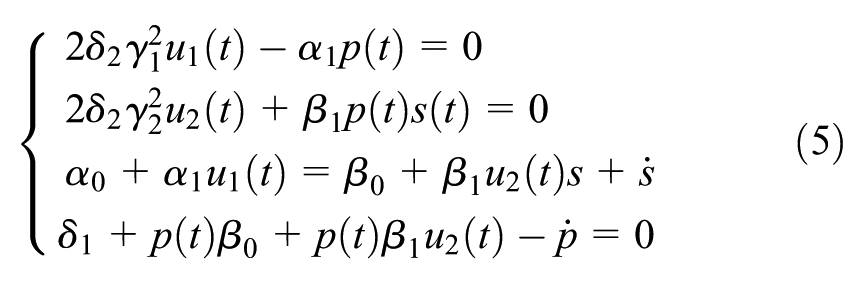
The first two constraints give us the value of
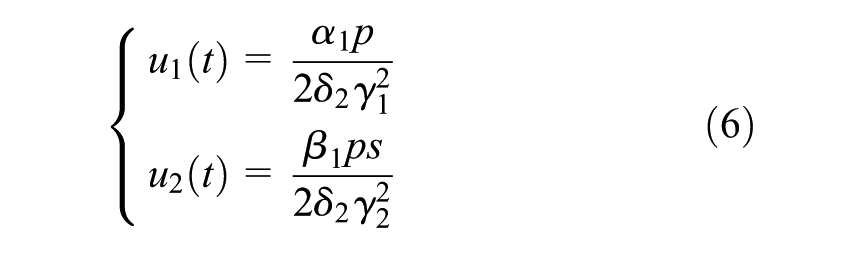
plugging these values back into the last two ODE constraints, we have
The time-variant optimal control problem we start with now becomes a set of ODE equations with initial and parameter values. One qualitative analysis we can conduct here is to compare if we should invest more in initiation intervention or cessation intervention, aka comparing
Here we have

is the optimal proportion of the budget that should be spent on initiation intervention versus cessation intervention.
Numerical Simulations
Here we consider one initiation intervention and one cessation intervention in our model to illustrate the optimal path of
To parameterize our simulation example, we use the 2014 estimates from the National Health Interview Survey (NHIS; 16.8% smoking prevalence and 0.35% initiation rate). Here we define the initiation rate as the 18 to 24 prevalence taken as a proportion of the entire adult population. We use the permanent cessation rate (net of relapses) of 4.5% estimated by Mendez et al. 23 As our policy example, we use cost and effectiveness values from the 12+12 weeks of varenicline treatment for smoking cessation and the US truth campaign for smoking prevention. In our analysis, one intervention unit covers 1 million individuals. This unit size is arbitrary and can be scaled up or down.
The values of
Last, we determine the values of
Simulations
Smoking Initiation Intervention
The truth campaign is a national youth smoking prevention campaign launched by the American Legacy Foundation starting from 2000. The truth campaign is a national tobacco counter-marketing campaign targeted primarily 12- to 17-year-olds. The campaign sent its antismoking message by TV commercials, advertisements, promotional items, street marketing, and a website. 25 Studies evaluating the US truth campaign found that 22% of the overall decline in youth smoking that occurred between 1999 and 2002 can be attributed to the campaign. In addition, the campaign was estimated to prevent 300,000 youth from smoking by 2002. 26 The total cost including travel costs is approximately 324 million dollars in 2002. Using 2014 US dollars, we estimated the per person cost to be 179 dollars.
Smoking Cessation Intervention
Among available smoking cessation alternatives, varenicline treatment, commonly branded as Chantix in the United States, is viewed by many as the most effective smoking cessation aid. 27 A randomized, double-blind trial published in 2006 recruited 1210 adult smokers to receive a 12+12 weeks of varenicline treatment. These smokers were assessed after 28 weeks where 603 patients were randomized to varenicline maintenance and 607 randomized to placebo. Researchers found that the 1-year abstinence estimate for the 12+12 weeks of varenicline treatment is 27.7%, compared with the 9.3% with placebo treatment. In addition, the average cost of the course of varenicline treatment was estimated at $603.89 in 2010. Knight and colleagues estimated the treatment cost as the sum of the initial 12 weeks of costs (covering one physician visit and 12 weeks of varenicline) and a further 12 weeks of maintenance therapy (another physician visit and 12 weeks of varenicline) for successful quitters. 28
Table 1 shows all the parameter values in our simulation example.
Parameter Values in the Simulation Example

Results
The figures show results obtained by employing the parameters derived from the NHIS data. Figure 1 shows the projected path of smoking prevalence without any intervention (status-quo path) over the next 30 years versus the projected trajectory derived from an optimal combination of initiation and cessation interventions over the same time period (optimal path).

Smoking prevalence among adults (≥18) in the United States from the National Health and Interview Survey (NHIS).
Figure 1 confirms that the numeric simulation is consistent with our theoretical results. With interventions, smoking prevalence decreases to 6.43% in 30 years versus the status quo of 8.54%. Figure 2 shows how the units of optimal interventions change over the 30-year span. The upper graph in Figure 2 shows the optimal units of initiation intervention over time while the lower one presents the optimal cessation units. We can see that both curves are monotonically increasing functions. In addition, both curves are convex. Convexity implies that as time goes on, the increases in units for both interventions accelerates.

Optimal intervention units over time, initiation versus cessation.
Figure 3 shows the optimal cost ratio over time to achieve allocative efficiency. Based on our earlier analysis, if

Optimal cost ratio between initiation and cessation.

Optimal cost versus alternative cost over time.
Discussion
This study establishes an optimal control model to investigate the best combination of smoking interventions to minimize smoking prevalence over 30 years while satisfying a budget constraint. By solving the model analytically using the Euler-Lagrange equation, we obtain a set of necessary conditions in forms of ODE. In addition, allocative efficiency is revealed in forms of the ratio between

The numerical simulations, based on interventions from the US truth campaign and the 12+12 weeks varenicline treatment combined with demographic data from NHIS and NSDUH, offer a few important observations. First, this simulation example verifies our theoretical results. With optimal interventions, smoking prevalence is reduced to 6.43% in 30 years compared to the original 8.54% while satisfying the budget constraint of 1 billion US dollars over 30 years.
Next, we observe the optimal trajectories of intervention units.
This study shows that optimal control methods can help us determine more efficient ways to address the smoking problem. The general framework established here can be applied to other problems in future research. Additionally, more features can be added when evaluating specific interventions. However, out study presents certain limitations. First, we employ a linear model of prevalence and constant policy effectiveness values. Linear ODEs are proven to be reasonable formulations for predicting smoking prevalence both domestically and globally. However, as prevalence declines, nonlinear effects might become more important in describing the system’s dynamics. Another limitation is that our formulation considers prevalence as a surrogate of population health effects, thus ignoring the timing differences between initiation and cessation related health benefits. Despite these limitations, our work presents a meaningful framework to analyze the issue of efficient allocation in tobacco control.