
Abstract
Approximately 100,000 persons in the United States undergo colorectal cancer (CRC) resection each year, intended to cure the malignancy. 1 Over one million patients are survivors of this procedure, and thus are candidates for post-resection surveillance. 2 Strategies are aimed at detecting adenomatous (conventional and serrated) polyps in the colon or extraluminal (metastatic) disease. 3 At 1 year post-resection, several approaches are endorsed by professional organizations; all include optical colonoscopy (OC) at 1 year, and guidelines for imaging studies vary. 4 If recommended, these take the form of computed tomography (CT) of the chest, abdomen, and pelvis annually or semiannually for up to 5 years.
Computed tomography colonography (CTC), also known as “virtual colonoscopy,” combines CT scanning with image reconstruction software that generates a high-quality visualization of the entire colorectum. In essence it recapitulates the abdominal and pelvic CT while also providing a virtual image of the bowel lumen. This suggests that CTC might substitute for CT + OC in the surveillance setting. For this reason, we conducted a multi-institutional prospective trial comparing CTC (including standard surveillance CT) to OC in 231 patients 1 year after colonic resection. 5 Patients underwent both procedures on a single outpatient visit, so that performance characteristics of CTC could be determined in a cohort wherein all subjects had the “gold standard” test. In addition, we cataloged all components of both procedures at the primary institution, in order to generate accurate costs of CTC and OC. In this article, we report, from a health care provider perspective, performance characteristics of the surveillance tests and cost to detect actionable colonic polyps (or “yield”) at 1 year post-resection.
Methods
Model
We constructed a simple decision tree to reflect the clinical problem (Figure 1). The decision is whether to perform CTC, and proceed to OC if an actionable polyp is detected, or to perform OC alone. In clinical practice, actionable polyps are defined as lesions of ≥6 mm detected on CTC, which would require OC and polypectomy. It is important to note that CTC cannot reliably differentiate between adenomatous polyps (conventional or serrated), the precursors of CRC versus hyperplastic polyps that have little or no malignant potential. The two branches of the decision node in Figure 1 reflect the problem.

Yield problem decision model.
The upper branch, CTC, leads to a chance node: either an actionable polyp is seen on the radiological test or no lesion is detected. Each branch of the chance node leads to a second uncertainty. The upper branch, denoted “Positive CTC,” leads to OC, which then divides denoting the presence or absence of an actionable polyp. Finding a polyp on OC after CTC reflects a “true positive” surveillance test, whereas “Negative” signifies a “false positive” CTC.
The lower branch of the CTC strategy, denoted “Negative CTC,” leads directly to the final chance node, “Adenoma” or “Negative.” In this yield model, a negative CTC leads to observation. If the test actually has missed an actionable polyp, that is a “false negative,” the deleterious outcome of the model. Otherwise the CTC is a “true negative,” a successful screen.
The lower branch of the decision node, OC, leads directly to the definitive chance node. OC is defined as the gold standard test: either an actionable polyp is detected or is not detected. This is reflected by the two branches at the lower right of the decision tree in Figure 1.
The objective of the problem is to minimize false negative CTCs, or maximize yield, at an acceptable cost of the surveillance procedures.
Clinical Data Collection
Five US academic medical centers contributed patients to the study. Eligible subjects were adult men and women with CRC, stages 0 to III at diagnosis, with uncomplicated colonic resection, referred for surveillance procedures between 9 and 16 months after surgery. 5 CTC was performed first, and then OC on the same day. In the event that a lesion was detected on CTC but not found on the initial OC, a study coordinator informed the endoscopist who reexamined the relevant colonic segment. This enhanced colonoscopy, an approach used in other CTC studies,6,7 was taken as the gold standard. Polyps underwent histological analysis by pathologists at the study institutions, and lesions were matched between CTC and OC to determine performance characteristic.
Data Used in the Analysis
Table 1 contains baseline and range data, taken from the clinical trial. 5 Per-patient data were collected from the trial; subsequent decisions are made based on whether any polyp is detected, not based on how many lesions are seen. We considered two action thresholds for polyps: 6 mm and 10 mm. For polyps ≥6 mm the prevalence was 36/231 patients. Sensitivity for the lower action threshold was 0.500 (95% confidence interval [CI] = 0.323–0.677); specificity 0.918 (95% CI = 0.877–0.959). Ten of the 231 patients had an actionable polyp ≥10 mm. At a threshold of ≥10 mm, sensitivity increased to 0.600 (95% CI = 0.246–0.954). Specificity was 0.973 (95% CI = 0.949–0.997).
Data Used in the Analysis

CI, confidence interval; CTC, computed tomographic colonography; OC, optical colonoscopy.
A study coordinator examined the charts and clinical items used for each patient seen at the lead study site. CTC demonstrated little variability, in terms of equipment and supplies, and in time for professional review (including scanning for extraluminal disease). Average costs were $155 for CTC (range $140 to $185). OC costs depended on whether biopsies were taken; OC without biopsy averaged $675 (95% CI = $659 to $691). OC with biopsy consumes more time and generates pathology costs, and thus averaged $996 (95% CI = $897 to $1,115).
Values of efficacy parameters used for sensitivity analysis are shown in Table 2. In addition to the range estimates from the clinical study, a few published reports present sensitivity and specificity of CTC in the surveillance setting. Kim and colleagues demonstrated sensitivity for adenomatous polyps of 0.800 (95% CI = 0.686–0.881) and specificity of 0.931 (95% CI = 0.904–0.952) in a series of 548 patients with 12% demonstrating polyps. 8 Amitai and colleagues achieved 100% per patient sensitivity and 71% specificity for polyps >5 mm in a small single-institution study of patients referred by medical oncologists for evaluation. 9 Prevalence of polyps was 50%. A recent meta-analysis of CTC for surveillance focuses on anastomotic recurrence and second (metachronous) colon cancers; unfortunately polyp detection is not discussed in the review. 10 A meta-analysis of CTC in the screening setting reported consensus sensitivity of 0.70 and specificity of 0.93 for actionable polyps ≥6 mm. 11
Data From Other Studies: Polyps ≥6 mm

No confidence intervals provided.
Meta-analysis consensus estimates; various prevalences.
For an alternative approach to the cost structure we utilized Medicare reimbursement data from Pyenson 12 updated to reflect 2017 regional payments. CTC reimbursement is set at $288, OC without biopsy averages $882, and OC with biopsy $1,230.
Results
Baseline Case
Figure 2 shows the decision tree folded back using baseline data from Table 1 for the detection of actionable polyps ≥6 mm. At a prevalence of 15.6% reported in the trial, CTC would lead to positive findings in 14.7% of patients. Of these 52.9% would have an adenoma confirmed on OC. Patients having a negative CTC would experience a false negative proportion of 0.091. Thus, the overall yield of CTC_S (CTC followed by OC) is 0.078, for an overall cost per patient of $279. Taking OC as the gold standard, its yield is simply the prevalence in this cohort: 0.156. Cost of the OC strategy would average $725 per patient.

Baseline analysis: 6 mm polyp.
Figure 3 replicates the model with baseline data for the detection of actionable polyps ≥10 mm. At the trial prevalence of 4.3%, CTC would appear positive in 5.2% of patients. Half of the positive CTCs would be true adenomas. False negatives would occur in 1.8%. The yield of CTC_S in polyps ≥10 mm is 0.026, for an overall cost per patient of $198. Cost of the OC cohort would average $689.
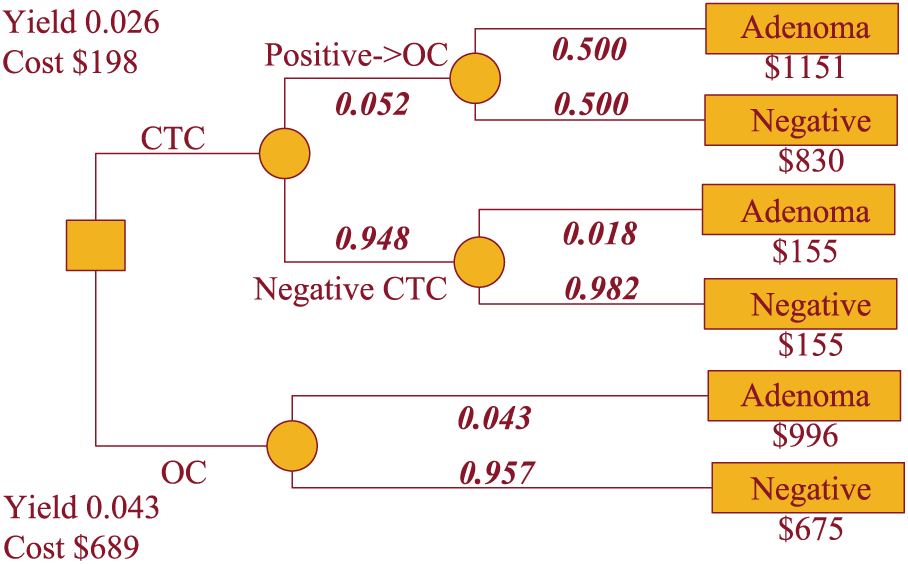
Baseline analysis: 10 mm polyp.
Cost-effectiveness calculations compare the baseline costs and yields for the two polyp size models. For the detection of actionable polyps ≥6 mm, the cost differential is $725 − $279, or $446. The yield differential is 0.156 − 0.078, or 0.078. Marginal cost to detect one more polyp at 1 year is $446/0.078, or $5725. For actionable polyps ≥10 mm the incremental cost-effectiveness ratio (ICER) is $491/0.017, or $28,350 to detect an additional larger polyp.
Another way to think of yield in this model is the number of actionable lesions missed by CTC_S. In Figures 2 and 3, the chance of a missed polyp is the product of the probability of a negative CTC and the posterior probability of an adenoma in that case. Multiplying 0.853 by 0.091 would lead to 779 missed polyps per 10,000 individuals tested in the ≥6 mm scenario. For actionable polyps ≥10 mm the corresponding value is 0.948 × 0.019, or 173 per 10,000 individuals.
Sensitivity Analysis
Figure 4 shows a graph of the marginal cost to detect an additional lesion ≥6 mm, through the range of prevalence from 0.05 through 0.5, holding the performance characteristics of CTC constant. As the likelihood of an actionable polyp increases, the OC strategy becomes progressively cheaper relative to CTC_S.
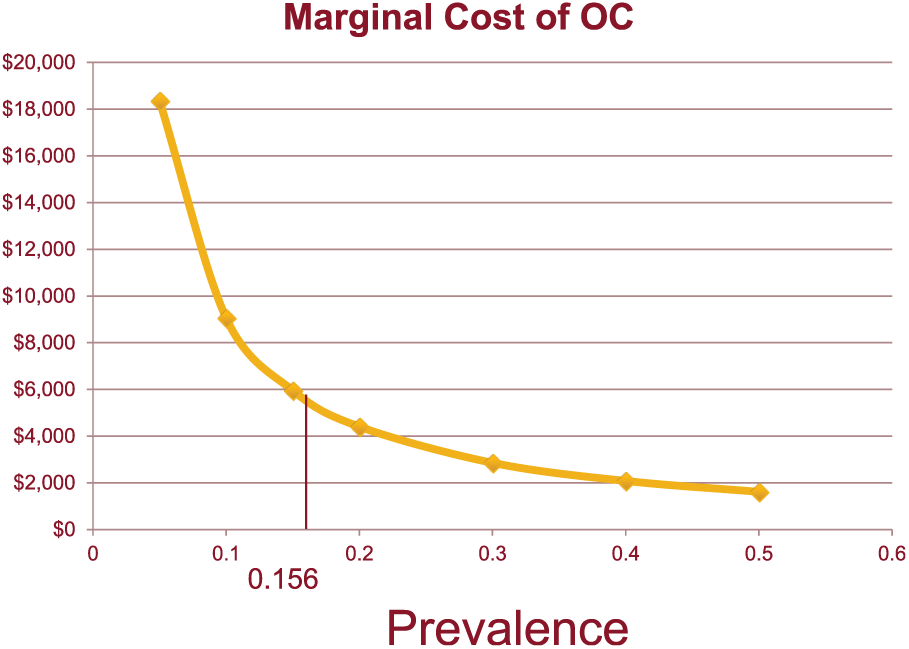
Sensitivity analysis: prevalence of actionable polyps ≥6 mm.
The Mulhall meta-analysis presented sensitivity and specificity values for actionable polyps ≥6 mm that were extremely close to ours. When sensitivity and specificity values from the Kim study are used, the ICER for OC rises to $12,200 per actionable polyp detected at the baseline prevalence, and CTC_S would miss 335 lesions. As the prevalence rises, the ICER for OC drops steeply, to $6,900 at a prevalence of 0.25 and $2,500 at 0.5 (compared to $3,500 and $1,600 using values from the present study).
Using regional Medicare costs, CTC_S costs $445 per case when detecting polyps ≥6 mm, whereas the OC strategy costs $936, for a cost to detect an additional polyp of $6,300. For polyps ≥10 mm, the ICER is $32,000. These are of the same order as the base case.
Discussion
This analysis is based on our study of CTC and OC in patients 1 year after surgical resection of colorectal cancer. We are modeling the long-term follow-up of this clinical problem, to include frequency of surveillance and detection of extraluminal lesions and the downstream health and utility consequences of missing adenomas. 13 Nevertheless, some insights can be gleaned from the 1-year analysis.
The cost-effectiveness metric, “cost to detect an additional polyp,” is nonstandard. There are no appropriate league tables to which we can compare our results to other medical procedures. However, the notion of “cost per event,” which we define in this article as “yield,” is arising in other areas. Dennis and associates conducted a trial of intermittent pneumatic compression to reduce deep vein thrombosis in poststroke patients. They found that the direct cost of preventing a deep vein thrombosis was £1,282 per event. 14 Zelman and colleagues recently examined the value of loop-mediated isothermal amplification for malaria detection in Indonesia, and reported an ICER of $5,900 per additional malarial infection detected. 15 Both these assessments were considered cost-effective by the authors.
We too believe that our yield metric is appropriate for modeling an intermediate endpoint. Is OC worth $5,000 to $6,500 to detect an additional polyp of 6 mm or greater? The ICER is on the order of the reports described above. Is missing 780 polyps per 10,000 surveyed too many? The literature is silent about what size a polyp must be to mandate action. A general consensus exists that polyps greater than 10 mm need to be found; in our study, the cost to detect an additional large polyp with OC is $28,350 compared to CTC_S. This suggests that CTC, which would miss 173 large polyps per 10,000, has a possible role in patients undergoing surveillance. For 6 mm polyps the marginal cost-effectiveness of OC is lower (i.e., better). Any improvement in the sensitivity of CTC would raise the ICER for OC, and thus improve the perceived value of CTC_S.
Another limitation is that we took component costs from a single institution, and used relative value units as the basis for physician costs (the largest contributor to case-by-case variation). However, using Medicare reimbursement as a proxy for costs led to similar results in our analysis.
Collecting costs and cataloging the components of procedures was straightforward in this clinical trial. By doing so we avoided a common problem in cost-effectiveness analysis: finding values relevant to the study under consideration. We suggest that building a cost analysis into clinical protocols is worthwhile, especially if giving thought to performing cost-effectiveness calculations after the trial results are in.
Although long-term modeling remains to be done in this problem, we conclude that a strategy of CTC at 1 year post colon cancer resection, to be followed by OC if positive, has a role in surveillance and for the detection of polyps ≥10 mm may be cost-effective relative to diagnostic procedures in other medical domains.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Financial support for this study was provided in part by Grants CA155347 and CA006297 from the National Institutes of Health. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Authors’ Note
Presented in part at the 39th Annual North American Meeting of the Society for Medicine Decision Making, October 2017.