
Abstract
How do individuals form new health beliefs and act in the context of unprecedented uncertainty? Drawing on a unique data set of registered California voters collected a month into stay-at-home orders that allows for an individual-level analysis, we examine the impact of political worldviews on trust in public health institutions and beliefs about the threat of COVID-19, effective methods for preventing the disease, and leaving home during the pandemic. Although all measures of political worldviews are strongly associated with trust in public health institutions and perceptions of threat, beliefs about effective prevention measures, and behavior, we find that Trump approval is particularly associated with COVID-19 risk perception and beliefs, beyond political party affiliation or life circumstances that shape exposure to COVID-19. We discuss the theoretical implications of these findings for understanding how political worldviews bear on embodied practices and shape the relationship between beliefs and action in unsettled times.
Introduction
The COVID-19 pandemic emerged in the United States at a moment of extremely high levels of political polarization on the one hand and extremely low levels of trust in government institutions on the other (Citrin and Stoker 2018; Iyengar et al. 2019). Against this backdrop, elected officials and public health agencies asked Americans to adopt a set of health behaviors and practices, such as frequent handwashing and social distancing, to limit transmission of the virus (Centers for Disease Control [CDC] 2020b). To stem the spread of infection, states and local counties across the nation ordered the closure of schools and businesses and permitted only those employed in “essential services” (e.g., medical, some retail, critical infrastructure, and emergency services) to leave their homes for work. These actions and orders were unprecedented in how they required individuals to alter their everyday behaviors and routines to reduce the spread of the disease and protect themselves and public health. However, the public’s compliance with these social distancing rules has been uneven, with some individuals challenging the orders and others praising them as necessary for reducing the spread of the virus (Luna and Willon 2020).
Because the evidence about the nature of the novel coronavirus and the risks it poses is developing, the pandemic has also created many opportunities for speculation and misinformation. Debate about the extent of the risk posed by COVID-19 and the correct way to address the pandemic has raged among elected officials and public media figures alike. Most notably, President Donald Trump has frequently suggested that the virus, and the extent of its harm, has been exaggerated by political liberals and other opponents, and he supported lifting stay-at-home policies (Baker 2020). Indeed, misinformation about the pandemic, including guidance on preventive actions to stem transmission of COVID-19, has been driven primarily by President Trump’s public statements and Twitter posts (Stohlberg and Weiland 2020). Against this backdrop, individuals have had to continually make small and large decisions about their basic daily practices—how frequently to wash their hands, how to treat packages, how often to leave their residences, whether to wear a mask or gloves when outside. These decisions about actions related to health are made in a profoundly unsettled time. Government-mandated closures unmoored people from institutions and routines, social norms regarding acceptable courses of action were unclear and evolving, and there was a lack of previous similar experiences or moral intuitions to draw on to shape courses of action. In this article, we ask how people formed their beliefs about COVID-19 and acted in the context of such uncertainty. In particular, we ask how the polarized political context and the politicized nature of COVID-19 public discourse has shaped Americans’ COVID-19-relevant beliefs and everyday actions.
Understanding how politics shape health behaviors and risk perception is especially pressing when we consider that the pandemic emerged among anxieties about the trustworthiness of government institutions. The country’s public health authority—the Centers for Disease Control and Prevention—has issued guidance on behaviors, but their authority is not sufficient to coordinate behavior nationally. The proliferation of COVID-19 misinformation—including false cures and conspiracy theories about the true origins of the virus—from varied sources has further complicated the issue (Frenkel, Alba, and Zhong 2020; Wemple 2020), forcing many to decide what information can be deemed reliable. Trust in the authority of different sources of COVID-19 information is segmented by political party, with Republicans stating that they are more likely to follow Trump’s presidential briefings on the pandemic and less likely to trust medical scientists for COVID-19 information than are Democrats (Funk, Kennedy, and Johnson 2020; Mitchell et al. 2020). In effect, existing political polarization, and attitudes about Trump in particular, seems to play a large role in shaping the public’s trust in health authorities and understanding of COVID-19 more generally.
In this article, we examine the extent of the relationship between political worldviews—as assessed by political party, political ideology, and Trump approval—and trust in public health institutions and COVID-19-related health beliefs and behaviors by drawing on a unique data set of Californians collected in the middle of April 2020, a relatively early phase of the COVID-19 pandemic in the United States. During this time, state governors grappled with whether and how long to call for stay-at-home orders (Sergent, Petras, and Bravo 2020), and the CDC revised its recommendations on behaviors such as face coverings and social distancing, inviting speculation and scorn from President Trump (CDC 2020b). We examine (a) the extent to which political worldviews are associated with trust in a range of public health institutions, such as the CDC and the World Health Organization (WHO), with respect to COVID-19; (b) how political worldviews are associated with beliefs about appropriate health practices in response to COVID-19; and (c) whether political worldviews predict who is more likely to leave home for work regardless of economic necessity.
We find that health beliefs and practices are developed in connection to political worldviews, which we argue serve as powerful lenses through which individuals navigate the current pandemic. Not only do political worldviews shape trust in public health institutions, such as the CDC, they also drive perceptions of threat and of what types of measures are more effective at preventing COVID-19 as well as behavior. For example, political conservatives (whether Republicans, ideological conservatives, or Trump approvers) are more likely to believe in the effectiveness of vitamins and less likely to believe in staying at home for preventing COVID-19 than political liberals. Political conservatives are also more likely to report leaving home to go work, net of controls for socioeconomic status and work industry. Our findings also indicate that Trump approval has an effect on COVID-19 beliefs beyond political party. Thus, to the best of our knowledge, this is the first article to examine the extent to which political worldviews—and Trump approval in particular—are important to pandemic beliefs and behaviors using individual-level data that account for variation in life experiences that produce unequal exposure to COVID-19.
The results support Swidler’s (1986:278) contention that in unsettled times of social transformation, “explicitly articulated cultural models, such as ideologies, play a powerful role in organizing social life”; in this case, political worldviews are central to the organization of social life in the pandemic. As such, in this article, we make three theoretical contributions to sociologists’ understanding of the formation of new health beliefs and behaviors. First, we extend the work on the role of politics in shaping embodied practices by illustrating how existing political worldviews coordinate responses to new health risks amid uncertainty and the absence of coordinated organizational and institutional support. Second, given the timing of our data, we develop the temporal aspect of Swidler’s (1986) insight by illustrating the swift alignment between political worldviews and health beliefs and practices. Finally, by illustrating the distinctive role of Trump approval, we suggest that the combination of distrust in government institutions and dominance of traditional and social media channels is particularly important in shaping the formation of novel health beliefs and practices.
We first review the literature on health and political ideology in settled times. We also discuss the literature on Trumpism and how the nature of the Trump presidency may shed light on the relationship between political worldviews and COVID-19 health beliefs and behaviors. After elaborating on our findings, we consider the theoretical implications of our research and indicate avenues for future research.
Political Worldviews, Confidence in Health Institutions, and Health Beliefs
In settled times, trust in government institutions is critical to understanding political behavior and collective action (Nye, Zelikow, and King 1997). Trust in public health institutions is similarly important because confidence is positively associated with health behaviors, such as vaccinations (including for seasonal influenza), use of medication, and regular doctor’s visits (Jackson et al. 2019). As scientific entities, public health institutions should, in theory, be seen as separate from politics, but survey data show that partisanship can structure views on public health institutions. In 2015, for instance, just 57 percent of Republicans saw the CDC favorably compared to 77 percent of Democrats (Baumgaertner, Carlisle, and Justwan 2018; Pew Research Center 2015). A 2011 report also showed significantly more Democrats than Republicans trusting the WHO (Baum 2011).
Still, other research suggests that these partisan sentiments toward the CDC before the pandemic may have been changing. The CDC enjoyed fairly strong public support in the years leading up to the pandemic (Jackson et al. 2019), and Republican support for the CDC has even grown over time. According to a poll from late March 2020, 79 percent of the public views the CDC favorably, with slightly more Republicans (84 percent) than Democrats (77 percent) reporting having a favorable view of the organization (Pew Research Center 2020). These findings suggest that CDC health recommendations might have been heeded by the American public in the early period of the pandemic when there was enormous medical and scientific uncertainty. 1
Sentiments about the CDC notwithstanding, previous work indicates that Americans mainly turn to their physicians, social networks, and online sources for health advice (Redmond et al. 2010), in part because they have come to see physical health and well-being as less a matter of collective responsibility and more a matter of personal responsibility (Larsen 2012). In fact, for both conservatives and liberals, there is a growing sense that government health advice is flawed and subject to bias from corporate interests or partisan values (Baumgaertner et al. 2018). As such, individuals are now accustomed to taking charge of their personal health by adopting lifestyle approaches (e.g., through diet or exercise or taking vitamins and supplements) to minimize the risk of illness and optimize their personal health (Crawford 1980; Lupton 2012).
Yet these individualist strategies can sometimes be in direct opposition to recommendations from public health authorities, and this is especially evident in the pattern of vaccine refusal, which is related to deep skepticism of pharmaceutical companies and the Food and Drug Administration (Reich 2016, 2020; Salmon et al. 2015). Indeed, vaccination is a state-mandated health behavior supported by strong scientific consensus, yet uptake and trust of vaccines has declined over time (Salmon et al. 2015). Negative attitudes about vaccines are a product of both lack of information or misinformation (Joslyn and Sylvester 2017) and profound distrust of experts and regulatory bodies (Reich 2016). Liberals are generally more provaccine than conservatives (Baumgaertner et al. 2018; Rabinowitz et al. 2016), a pattern driven by distrust in government medical experts among conservatives (Baumgaertner et al. 2018). Looking back at the novel H1N1 influenza (also called the swine flu) pandemic of 2009, politics also played a role in the public’s willingness to be vaccinated against this disease. A 2009 Pew Research poll found that 41 percent of Republican respondents and 60 percent of Democrats said they would be willing to get the H1N1 vaccine (Pew Research Center 2009). In effect, despite an individualist turn to health and well-being in America, partisanship still matters when it comes to certain health issues and public confidence in the federal government to deal with a public health crisis (Mesch and Schwirian 2014).
When scientific guidance is unclear, previous research has found that individuals fall back on political worldviews to make sense of this information and determine how to respond (McCright and Dunlap 2011; McCright et al. 2013). Political liberals and conservatives are equally likely to disregard dissonant scientific messages, suggesting that neither group has a monopoly on science skepticism and that group membership and ideology are powerful lenses through which scientific messages (including messages about health) are interpreted (Nisbet, Cooper, and Garrett 2015). Consequently, dissonant science messages rarely change minds; rather, they increase distrust in science and the institutions that produce it or rely on it for policymaking (Hart and Nisbet 2011; Nisbet et al. 2015). This is because political ideology conditions how individuals process information (Kahan 2013) and perceive risks (Kahan et al. 2010). People process scientific facts in reference to their membership within cultural or ideological groups (Kahan 2013; Kahan et al. 2010; Kahan, Jenkins-Smith, and Braman 2011).
And although ideology influences the receipt of science-based messages for both liberals and conservatives, general confidence in science has declined more steeply for the latter than for the former (Gauchat 2012). Gauchat (2012) and Mooney (2005) argue that the Reagan administration ushered in this skepticism toward science among conservatives and that the most precipitous decline in confidence in science occurred during the 2001–2009 Bush administrations. Because conservative ideology incorporates an antielitist form of antiintellectualism and populism (Merkley 2020; Motta 2017; Oliver and Rahn 2016), among conservatives, science is seen as an institution that justifies regulatory interference by elites, thereby curbing capitalist expansion and individual freedoms (Blank and Shaw 2015; Gauchat 2012). Even in settled times, politics shape health behaviors and risk perceptions. We expect this effect to be even stronger in the context of widespread disruption to routines and institutions, coupled with politically driven anxieties about the trustworthiness of government institutions.
The Trump Presidency as a Unique Dimension of Political Worldviews
Given the research on science and politics, we know that party affiliation serves as a powerful driver of risk beliefs (Blank and Shaw 2015; Gauchat 2012; Motta 2017; Rabinowitz et al. 2016), yet there are important nuances worth highlighting, especially in the current Trump era. During this time, Republicans more generally have become ever more the partisan loyalists, even if it is at odds with their ideological position, and many have looked to Trump for cues on beliefs and behavior (Barber and Pope 2019). One recent study even showed that Republicans became less supportive of childhood vaccination after being exposed to Trump’s antivaccination views expressed on Twitter (Hornsey et al. 2020).
The Trump presidency has also ushered in a dimension of political worldviews that can be thought of as somewhat distinct from ideological conservatism and the Republican party, in particular due to his vocal distrust and active undermining of government bureaucracies and norms. As president, Trump appears to have only amplified existing levels of distrust of government experts and science among Republicans and conservatives (Hornsey et al. 2020; Oliver and Rahn 2016). Another relatively unique aspect of the Trump presidency relevant to understanding how Trump approval might shape COVID-19-related beliefs and behaviors is the extent of dominance of Trump’s media presence. Whether in mainstream outlets, social media, or ideologically committed outlets, Trump enjoys and cultivates an enormous amount of coverage. Both the constant information from Trump on Twitter and the rebroadcasting of that information from various sources amplify the extent of his messaging.
Trump’s decisions about governance, his influence over the federal pandemic response, and his comments undermining the seriousness of the pandemic are unprecedented for the leader of a country facing a major health crisis. In his press conference and Twitter communications, Trump has been openly hostile to public health authorities and experts, including those from the CDC and in his own COVID-19 task force (Baker 2020). Throughout the pandemic, Trump has also been extremely critical of the WHO and in May announced that he was pulling U.S. funding from the organization (Joseph 2020).
There is evidence that Trump’s positions have created fractures within his Republican base. For example, political writers report that Republicans are leaving the party as a result of Trump administration policies and Trump’s public and private conduct (Blake 2019; Karmack, Podkul, and Zeppos 2018). His administration’s handling of the pandemic also appears to have deepened this fracture within the party given that some Republicans have chastised his actions (Karmack 2020). This suggests a need to study Trump approval in addition to just ideology or partisanship.
In sum, we see three dimensions of politics at play with respect to attitudes and behavior around COVID-19: party affiliation, political ideology, and degree of approval of Trump’s job as president. Although these dimensions overlap, each provides nuanced information on how politics are associated with COVID-19 beliefs and behaviors.
We posit the following hypotheses:
Hypothesis 1: More conservative political worldviews (Republican, ideologically conservative, and pro-Trump) are associated with less trust in public health institutions.
Hypothesis 1a: More Trump approval among those who identify as Republicans is associated with less trust in public health institutions.
Hypothesis 2a: Net of controls for risk of COVID-19, having more conservative political worldviews is associated with perceiving less threat of getting sick with COVID-19.
Hypothesis 2a.1: More Trump approval among those who identify as Republicans is associated with perceiving less threat of getting sick with COVID-19.
Hypothesis 2b: Net of controls for risk of COVID-19, having more conservative political worldviews is associated with perceiving public-health-related prevention methods as less effective.
Hypothesis 2b.1: More Trump approval among those who identify as Republicans is associated with perceiving public-health-related prevention methods as less effective.
Hypothesis 3: Among individuals who report leaving home for work, net of controls, having more conservative political worldviews is associated with leaving home for work more frequently.
Hypothesis 3b: More Trump approval among those who identify as Republicans is associated with leaving the home for work more frequently.
Data
Data for this study come from a survey of 8,800 registered voters in California from April 16 to April 20, 2020, administered by the Institute of Governmental Studies in conjunction with the California Institute of Health Equity and Action. By the date the survey started, 27,677 people in California (663,000 nationally) were confirmed COVID-19 cases, and 956 people in California (29,200 nationally) had died from the disease. In California, Governor Gavin Newson (Democrat) imposed stay-at-home restrictions on March 19, 2020; it was the country’s first statewide stay-at-home order. It required all residents to stay home except to go to an essential job or shop for essential needs (California State Government 2020). All school districts across the state were closed. County officials immediately met to put safeguards into place. Our data were collected four weeks after this point, after Governor Newson had indicated that the stay-at-home order might remain in effect through mid-June (CalMatters 2020; Lin 2020). At that point, there were not yet mass demonstrations against stay-at-home orders, either in California or elsewhere in the United States. The CDC had issued recommendations about wearing cloth face masks on April 3, 2020 (Dwyer and Aubrey 2020), but at the point when the data were collected, wearing face masks was not yet a matter of political contention. For example, it was not until April 28 that Vice President Pence visited the Mayo Clinic without wearing a face mask, drawing praise and criticism (Liptak 2020).
The survey was administered by distributing email invitations to a stratified random sample of the state’s registered voters in an attempt to obtain a proper balance of survey respondents across major segments of the registered voter population. At the conclusion of the data-processing phase, poststratification weights were applied to align the sample to population characteristics of the state’s overall registered voter population. The sampling error associated with the results from the survey are difficult to calculate precisely due to the effects of sample stratification and the poststratification weighting. Nevertheless, it is likely that the results are subject to a sampling error of approximately ±3 percentage points at the 95 percent confidence level. All findings reported in the following are the same with and without the survey weights.
Dependent Variables
Trust in Public Health Institutions
Respondents reported the extent to which they trusted various institutions “to provide accurate information about COVID-19” using a 4-point scale (recoded as 1 = completely distrust, 2 = somewhat distrust, 3 = somewhat trust, 4 = completely trust). We summed responses to trust in public health institutions relevant to the pandemic: the CDC, the WHO, and state and local public health agencies (state and/or local health department; all items load on one dimension at .8 or higher using a polychoric factor analysis). For comparison, we also examined trust in “scientific experts (for example researchers in the University of California system, Stanford, Harvard),” “my personal physician/health care provider,” and “community organizations, including faith-based organization or church.”
Health Beliefs
Perceived Threat of Getting COVID-19
Respondents reported their perceptions of the threat of getting sick from COVID-19 in three questions: the extent to which COVID-19 was a threat to their personal or family health on a 3-point scale (recoded as 1= no threat, 2 = a minor threat, 3 = a major threat), the degree to which they perceived getting sick with COVID-19 to be a serious problem on a 4-point scale (recoded as 1 = no problem at all, 2 = not much of a problem, 3 = somewhat serious problem, 4 = very serious problem), and how concerned they were that they would “get the coronavirus and require hospitalization” on a 4-point scale (recoded as 1 = not at all concerned, 2 = not too concerned, 3 = somewhat concerned, 4 = very concerned). The responses to these three questions were summed to create a measure of perceived health threat of COVID-19 (all items load on one dimension at .76 or higher using a polychoric factor analysis).
Efficacy of Prevention Methods
Respondents assessed the efficacy of the following methods for preventing the contraction of COVID-19 using a 3-point response scale (recoded as 1 = not effective at all, 2 = somewhat effective, and 3 = extremely effective): “staying at home as much as possible,” “wearing a mask,” “staying 6 feet away from other people,” “washing hands regularly,” “wearing gloves,” “taking vitamins,” and “eating a healthy diet.” We create a scale of perceived efficacy of public health recommendations by summing the first four of these (staying home, wearing a mask, staying 6 feet away, and washing hands), which are the most publicized public health recommendations (all items load on one dimension at .67 or higher using a polychoric factor analysis). We create a scale of individualist preventive measures by summing the final two of these (taking vitamins and eating a healthy diet; both load on one dimension at .78 using a polychoric factor analysis). 2 We do not include wearing gloves in either scale because it did not load strongly onto either of these dimensions.
Frequency of Leaving the House for Work
Respondents were asked how many times in the past week they left the house for work during shelter-in-place with eight response options, from 0 to 7 or more.
Independent Variables
Political Party Affiliation
Respondents reported whether they “generally speaking, in politics . . . think of [themselves] as: Democrat, Republican, Independent, Something else.” We used this to create dummy variables for each of the response answers.
Political Ideology
Respondents reported their political views on a 5-point scale (recoded as 1 = very liberal, 2 = somewhat liberal, 3 = moderate, 4 = somewhat conservative, 5 = very conservative).
Trump Approval
Respondents answered whether they “approve or disapprove of the way Donald Trump is handling his job as president” using a 5-point scale (recoded as 1 = disapprove strongly, 2 = disapprove somewhat, 3 = neither approve nor disapprove, 4 = approve somewhat, 5 = approve strongly).
Controls
COVID-19 Risk
A series of variables assessed respondents’ relative risk of contracting COVID-19 and the life circumstances that might affect how serious of a threat COVID-19 would be to them or their families. We include these variables as controls in models when theoretically relevant to the dependent variable. We used a binary variable for risk to immediate family (“Some of my immediate family members have to work outside the home and, in some cases, their jobs involve regular contact with other people”). Respondents reported how many months over the last year they had health insurance using a 3-point scale (1 = less than 6 months, 2 = 6–11 months, 3 = all 12 months), which we use to assess how great of a perceived problem contracting COVID-19 might be to the respondent. A binary variable captured whether the respondent lived with anyone over 65 years old; we include this to capture living with someone at greater risk from COVID-19. In the analysis of the perceptions of the relative efficacy of various prevention practices, we control for perceived threat of COVID-19 using two variables described previously as dependent variables (perceiving getting sick with COVID-19 to be a major threat to one’s personal or family health and concern about getting COVID-19 and needing hospitalization). We do this in case perceived COVID-19 threat alters perceptions of the relative efficacy of different prevention measures.
Work and Economic Precarity
For the analysis of frequency of leaving home for work, we include controls for industry because people working in different industries, particularly those deemed essential, had different requirements for leaving for work during this period. Respondents who reported working reported their industry as belonging to one of 20 categories. We recoded these to 10 categories (health, essential services, nonessential services, self-employed, professional, manufacturing, construction, agriculture, government [reference], and other). We include whether a respondent reported that not being able to pay for basic necessities was a problem for them as a result of the COVID-19 pandemic (4-point scale recoded as 1 = no problem at all, 2 = not much of a problem, 3 = somewhat serious problem, 4 = very serious problem). We do so to account for economic precarity (separate from income) that might drive individuals to leave the house for work more often.
Individual Characteristics
All models included controls for education, age, gender, racial identification, and income. We assess education using a dummy variable for whether the respondent had a BA degree or a higher degree compared to those who did not attend or finish college. We include dummy variables for whether a respondent is between 18 and 35 (and thus are at a statistically lower risk of getting very sick or dying from COVID-19) or over 60 years old (and thus at a statistically higher risk). We include a binary variable for whether the respondent is male (female or other gender identities are the reference category). Respondents reported their racial identification, which we converted into five binary variables (Latino/a, Black, Asian, Native American/Alaskan Native/other; identification as white is the reference). Respondents reported their approximate income using a 9-point scale from less than $20,000 to more than $200,000. We include income controls to address the fact that outcome measures, such as taking vitamins as a means to prevent COVID-19, may have class-based connotations.
Analytical Approach
We analyze the role of politics in (a) trust in medical institutions, (b) health beliefs (assessment of getting sick and efficacy of different prevention methods), and (c) the frequency of leaving the house for work during the pandemic. We conduct two types of analyses for the dependent variables trust in public health institutions and health beliefs. First, separately, we examine the relationship between the dependent variable and one of the three measures of political beliefs and affiliation (political party, ideology, and Trump approval), net of controls. We also describe the results when subsets of two and then all three political worldviews measures are included in the models. Despite the high overlap between the measures, when including all three measures in the same model, no variance inflation factor exceeds 2.9. We use the summed scales as the dependent variables and model the relationship using ordinary least squares regression (OLS). 3 The reported results are the same using ordered logistic regressions. Second, for each dependent variable, we examine the effect of Trump approval for the subset of respondents who identify as Republicans (n = 1,370). We do this to examine the unique effect of Trump approval within political party, with the assumption that those within the same political party will have more similar political beliefs than between political parties and thus provide for a more precise examination of the effect of Trump approval. For this second type of analysis, we use the individual measures instead of the summed scales and ordered logistic regressions. In these analyses, we control for living with someone exposed to others while working outside the home, health insurance, education, age, gender, racial identification, and income for all three sets of dependent variables.
We repeated these analyses with the subset of respondents who reported that they were still working during the pandemic and controlled for whether people had to leave their house for work during the pandemic (plus controls for industry and economic precarity) to examine whether the reported relationships changed for those individuals who are most personally affected and at risk. We found no differences between the effects reported in the following and the effects with this subset of respondents.
To analyze how often respondents reported leaving home for work in the past week, we use only the subset of respondents who reported leaving home for work at least once in the previous week (n = 4,067) to conduct the analysis among a pool of respondents who do leave home for work and to attempt to net out any important unobserved differences between those who can and those who cannot stay home to work. Among this subset of respondents, we examine the separate effect of each of the three political variables net of controls for perceived economic precarity, health insurance coverage, living with someone over 65, industry, education, age, gender, racial identification, and income using OLS. We include these controls to attempt to account for the fact that the amount of discretion respondents have about the choice to leave for work varies. The reported results are robust to using Poisson models. We then examine the relationship between Trump approval and the number of times participants report leaving for work separately among Republicans (n = 717).
Finally, we assess the relative contribution of trust in public health institutions to COVID-19 health beliefs and the contribution of perceptions of the efficacy of staying home to leaving home for work using mediational analyses.
All reported analyses use the survey weights for the data and list-wise deletion for missing values. The results are robust to various modeling approaches, controls, and specifications of the dependent and independent variables; any exceptions are noted in the following.
Results
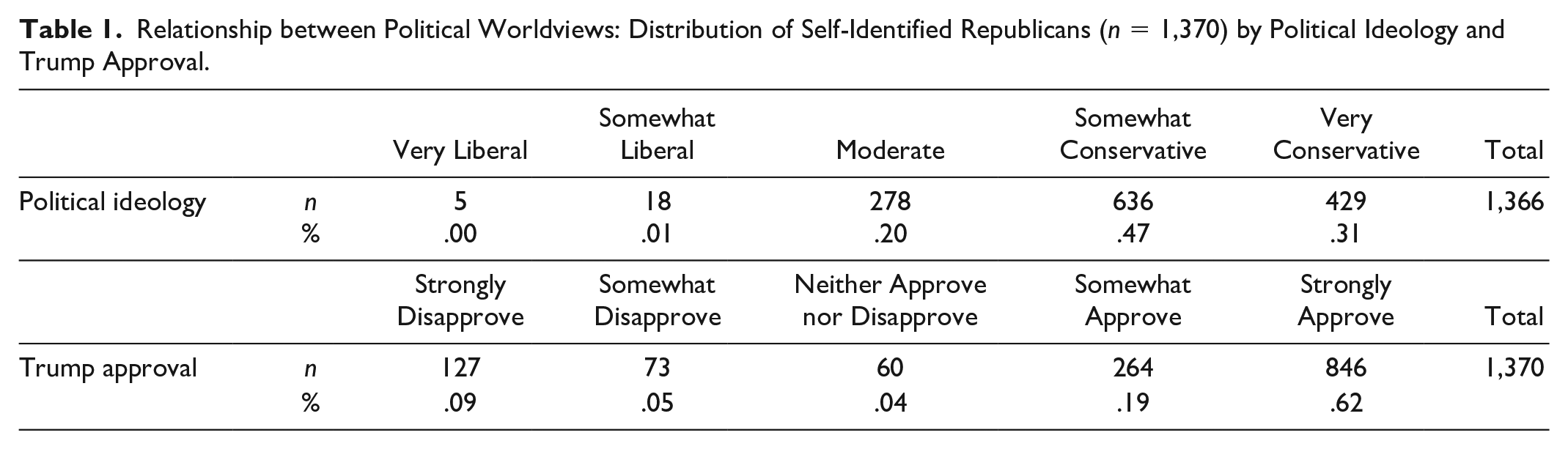
The three measures of political worldviews for this sample are related but not identical (see Table 1). In this sample, the unweighted polychoric correlation between the scale variables, political ideology and Trump approval, is .82. Thirty-one percent of Republicans identify as very conservative, and 0 percent identify as very liberal in terms of political ideology (the unweighted mean is 4.07 out of 5). Sixty-two percent of Republicans in this sample report strongly approving of the job Trump is doing as president; 9 percent report strongly disapproving of the job Trump is doing (the unweighted mean is 4.17 out of 5).
Relationship between Political Worldviews: Distribution of Self-Identified Republicans (n = 1,370) by Political Ideology and Trump Approval.
The demographic characteristics of political worldview groups (Republicans, strong political conservatives, strong Trump approvers, Democrats, strong political liberals, strong Trump disapprovers) illustrate the variation in the composition of the groups (see Appendix Table 1a). In line with other findings (Edsall 2019; Kitschelt and Rehm 2019), in this sample, politically conservative worldview groups are more male, older, less educated, and more white and generally have more income than politically liberal worldview groups. See Appendix Table 1b for descriptive statistics, both unweighted and weighted, for the key dependent variables, means by political worldview, and Appendix Table 1c for their correlations.
Trust in Public Health Institutions
In this sample as a whole, the average response to questions about trust in public health institutions was closest to the somewhat trust response option. Net of controls, in each of the three models, the measure of greater political conservatism (Republican party adherence, more conservative political beliefs, and more Trump approval) is negatively associated with trust in public health institutions for information about COVID-19 (−2.31 for Republicans compared to Democrats in the political party model, −.97 in the political ideology model, and −1.19 in the Trump approval model; standardized coefficients). When all three measures of political worldviews are included in the model, all three measures are negatively related to perceived threat of COVID-19, although identifying as Republican is no longer statistically significant (R2 = .35; ßs = −.20 for Republican, −.29 for political ideology, and −.95 for Trump approval). See Table 2.
Ordinary Least Squares Regression of Political Worldviews on Trust in Public Health Institutions for Information on COVID-19 Pandemic.

Note: Standard errors appear below standardized coefficients. All continuous predictors are mean-centered and scaled by 1 standard deviation. Models include controls (not displayed). See Appendix for full model with controls.
p < .001.
Effect of Trump Approval among Republicans: Trust in Public Health Institutions and Other Sources
To examine the effect of Trump approval within the Republican party, we examine models of Trump approval and trust in public health institutions, personal physician, and community and religious organizations for information about COVID-19 for the subset of respondents who report being Republicans. Among Republicans, 0 percent of those who strongly disapprove of Trump express the lowest level of trust in public health institutions; this percentage is 5 percent among those who strongly approve of Trump. Twenty-one percent of those who strongly disapprove of Trump express the highest level of trust in public health institutions, whereas only 3 percent of Trump approvers do so. Using ordered logistic regressions and separate models for each dependent variable, net of controls, we see that Trump approval is negatively associated with trust in the CDC, the WHO, public health departments, and scientific experts regarding information about COVID-19. There is no significant association between Trump approval and trust in one’s own physician. There is a positive association between Trump approval and trust in community or religious organizations for information about COVID-19 (see Figure 1).

Trust in sources of information about COVID-19 by Trump approval among Republicans.
Health Beliefs
Perceived Threat of Getting COVID-19
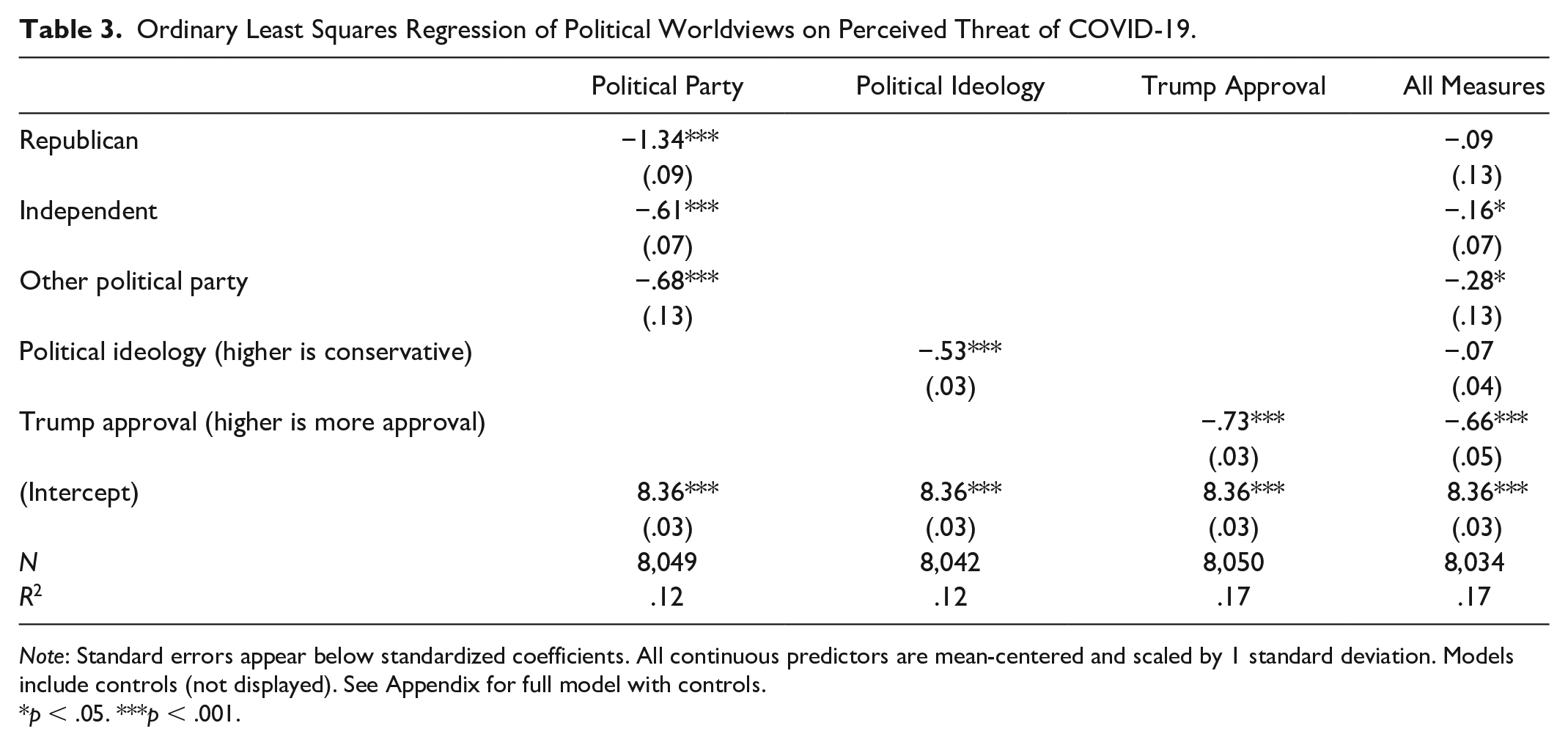
In each of the three models, the measure of greater political conservatism (Republican party, more conservative political beliefs, and stronger Trump approval) is negatively associated with perceiving COVID-19 as a threat (−1.34 for Republicans compared to Democrats in the political party model, −.53 in the political ideology model, and −.73 in the Trump approval model; standardized coefficients). When all three measures of political worldview are included in the model, all three measures are negatively related to perceived threat of COVID-19, but only Trump approval is statistically significant (R2 = .17; ß = −.66). See Table 3.
Ordinary Least Squares Regression of Political Worldviews on Perceived Threat of COVID-19.
Note: Standard errors appear below standardized coefficients. All continuous predictors are mean-centered and scaled by 1 standard deviation. Models include controls (not displayed). See Appendix for full model with controls.
p < .05. ***p < .001.
Effect of Trump Approval among Republicans: Threat of COVID-19
We examine models of Trump approval and perceived threat of COVID-19 for the subset of respondents who report being Republicans using ordered logistic regressions. Among Republicans, 7 percent of the strongest Trump approvers express the least perceived threat of COVID-19, compared to 0 percent of strong disapprovers. Twenty-eight percent of those who strongly disapprove of Trump express the highest perceived threat of COVID-19 compared to 11 percent among those who strongly approve of Trump. In separate models for each dependent variable, we see that Trump approval is negatively associated with perceptions of threat of getting COVID-19 for all three individual measures (see Figure 2).

Perceived threat of getting COVID-19 by Trump approval among Republicans.
Efficacy of Public Health and Individualist Preventive Measures
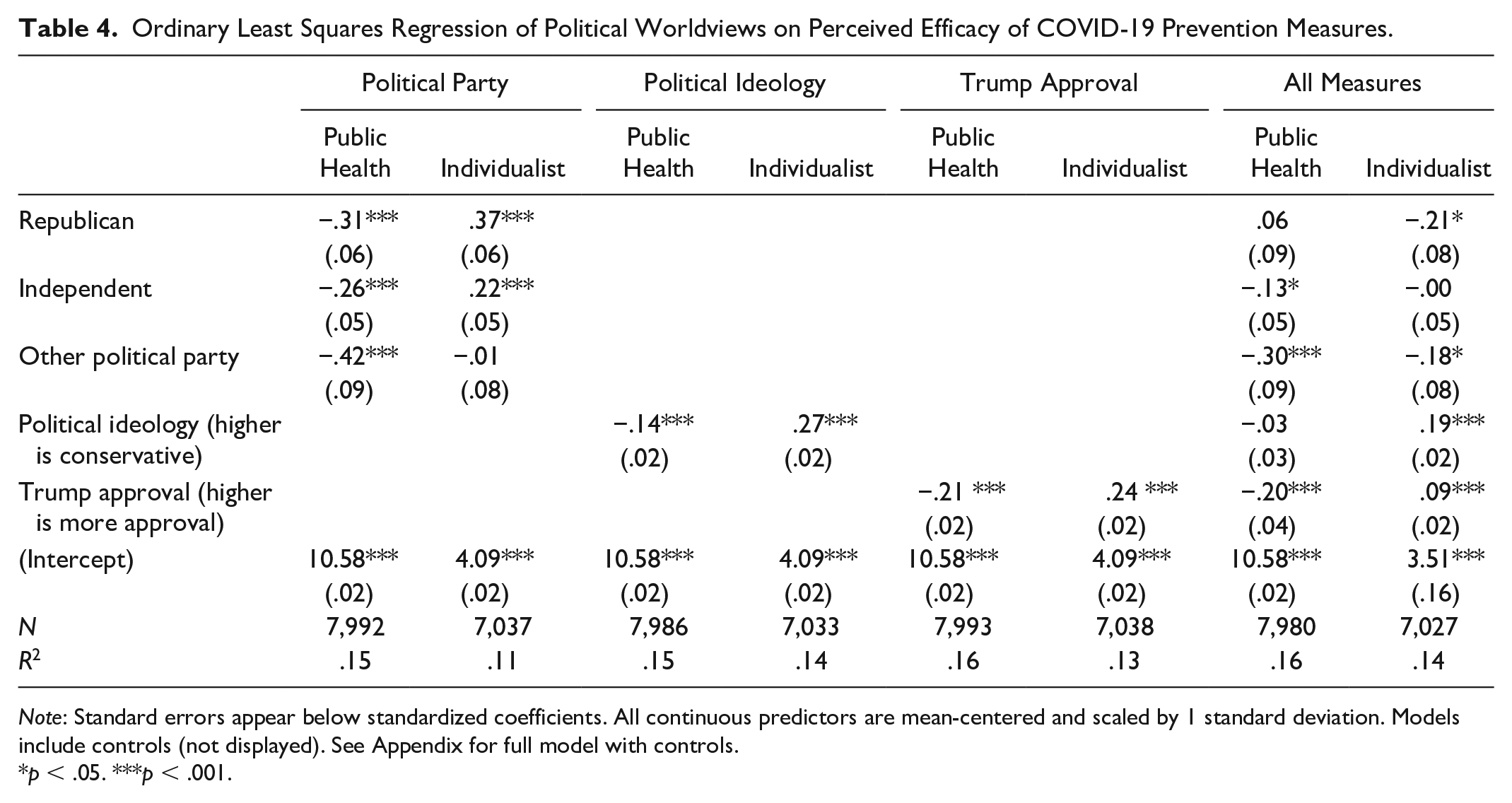
Net of controls, in each of the three models, the measure of greater political conservatism is negatively associated with believing that public health prevention measures are most effective (−.31 for Republicans compared to Democrats in the political party model, −.14 in the political ideology model, and −.20 in the Trump approval model; standardized coefficients). When examining the effect of multiple measures of political worldviews on the perceived efficacy of public-health-related prevention measures, only Trump approval is statistically significant (R2 = .16; ß = −.20). See Table 4.
Ordinary Least Squares Regression of Political Worldviews on Perceived Efficacy of COVID-19 Prevention Measures.
Note: Standard errors appear below standardized coefficients. All continuous predictors are mean-centered and scaled by 1 standard deviation. Models include controls (not displayed). See Appendix for full model with controls.
p < .05. ***p < .001.
The opposite pattern appears when examining beliefs about the efficacy of individualist preventive measures. Net of controls, in each of the three models, the measure of greater political conservatism is positively associated with believing that individualist preventive health measures are most effective (.37 for Republicans compared to Democrats in the political party model, .27 in the political ideology model, and .24 in the Trump approval model; standardized coefficients).
When all three measures are included in the model, Trump approval and identifying as an independent remain statistically significant, although the direction of the effect for being a Republican switches such that net of ideology and Trump approval, being a Republican is associated with beliefs that individual measures are less effective compared to Democrats (ß = −.21 for Republican, .19 for political ideology, and .09 for Trump approval). 4 Political ideology has the strongest association with beliefs about individualist preventive measures.
Effect of Trump Approval among Republicans: Efficacy
To examine the effect of Trump approval within the Republican party, we examine models of Trump approval and perceived efficacy of prevention measures for the subset of respondents who report being Republicans. For example, among Republicans, 13 percent of people who strongly approve of Trump believe that wearing a mask is not at all effective, 49 percent believe it is somewhat effective, and 38 percent believe it is extremely effective against COVID-19. In contrast, among those who strongly disapprove of Trump, 6 percent report that wearing a mask is not at all effective, 50 percent believe it is somewhat effective, and 45 percent believe it is extremely effective. At the same time, 29 percent of those who strongly approve of Trump believe that vitamins are extremely effective in preventing COVID-19, whereas only 19 percent of those who disapprove of Trump believe so. Using ordered logistic regressions and separate models for each dependent variable, we see that Trump approval is associated with perceiving staying at home, the most politicized public health recommendation, to be less effective and with perceiving taking vitamins and eating a healthy diet, the two individualist, nutrition-related preventive measures, to be more effective (see Figure 3). The other measures are not statistically significant.

Perceived efficacy of prevention methods by Trump approval among Republicans.
Leaving Home for Work
To provide an indication of the effect of political worldviews on pandemic-related behavior, we examine the relationship between political affiliations/beliefs and a self-reported behavior: number of times a respondent left the house for work in the past week. To compare across similar respondents, for this analysis, we use the subset of respondents who report leaving the house for work at least once during the past week (the results are robust to other ways of subsetting respondents who are working).
Net of controls for individual characteristics, perceived economic precarity, work industry, and living with someone over 65 (a measure of the health threat to one’s family), in each of the three models, the measure of greater political conservatism is positively related to leaving the house more frequently (.52 for Republicans compared to Democrats in the political party model, .29 in the political ideology model, and .25 in the Trump approval model; standardized coefficients). When all three measures are included in the model, only political ideology remains positive and statistically significant (ß = .23). Trump approval remains positive (ß = .11) but not statistically significant, and net of ideology and Trump approval, being a Republican is associated with being less likely to leave home for work (ß = −.03). See Table 5.
Ordinary Least Squares Regression of Political Worldviews on Frequency of Leaving House for Work in Past Week.

Note: Standard errors appear below standardized coefficients. All continuous predictors are mean-centered and scaled by 1 standard deviation.
p < .05. **p < .01. ***p < .001.
Effect of Trump Approval among Republicans: Leaving Home for Work
To examine the effect of Trump approval within the Republican party, we examine models of Trump approval and frequency of leaving home for work among the subset of respondents who report being Republicans. Those who strongly disapprove of Trump report leaving their house for work 3.47 times during the previous week, whereas those who strongly approve of Trump report leaving their house for work four times during the previous week. In these models, net of controls, we do not find a unique effect of Trump approval on leaving the home for work (see Figure 4).

Reports of leaving the house for work by Trump approval among Republicans.
Effects by Race and Gender
Previous work illustrates how gender and race impact risk perception in general (Finucane et al. 2000; Rivers, Arvai, and Slovic 2010), and we observe similar patterns in this data set regarding perceived risk around COVID-19. Net of controls, white men are less likely than women and racial minorities to perceive a threat of getting COVID-19. Men are also less likely to believe in the efficacy of either public health or individual preventive measures, and they leave home for work more often. Across all measures of political worldviews, Latino/as and Asians perceive COVID-19 as a greater threat; Black people perceive greater risk when political worldviews are measured using political ideology.
The effects of racial identity on the other key dependent variables are also notable. Respondents who identify as American Indian or other racial identities are less likely to trust public health institutions, net of controls, compared to people who identify as white. All racial groups perceive greater efficacy of individualist COVID-19 preventive strategies compared to whites; those who identify as Asian also perceive public health prevention strategies to be more effective compared to whites. Given the greater perceived threat among racial minorities, a heightened sense of vulnerability might lead people in these groups to perceive all preventive measures as important. The coefficients for Latino/a, black, and Asian respondents’ perceptions of the efficacy of public-health-endorsed preventive measures are all positive, although they do not differ from those of white respondents at a statistically significant level. Finally, Latino/as report leaving home for work more frequently than do whites. This is consistent with reports that racial/ethnic minorities are at a higher risk of exposure to COVID-19 because of the types of jobs they do, which are more likely to be essential (CDC 2020a). 5
Mediational Analyses
As we might expect, the beliefs and practices described previously that are so strongly associated with political worldviews are also related to one another. For example, trust in public health institutions is a significant mediator of the effect of political worldview (any of the three measures, p < .001) on the perceived efficacy of public-health-recommended prevention practices. This mediation effect is particularly strong for Trump approval, where trust in public health institutions fully mediates the relationship between Trump approval and the perceived efficacy of public health prevention practices. Trust in public health institutions, however, does not mediate the relationship between political worldview and the perceived threat of COVID-19.
We can also examine how pandemic-related health beliefs—specifically, perceptions of the efficacy of staying home for preventing COVID-19 infection—are related to pandemic-related health behaviors. Again, we see a mediation effect whereby perceptions of the efficacy of staying home partially mediates (p < .001) the effect of political worldviews on the frequency of leaving the house for work over the past week.
Discussion
Our findings illustrate the significant association between political worldviews, regardless of the measure, and Americans’ COVID-19-related health beliefs and behaviors. Republicans, ideological conservatives, and Trump supporters express less trust in public health institutions; perceive less risk of contracting COVID-19; believe individualist preventive strategies, such as vitamin use and diet, to be more effective and public health prevention measures, such as staying at home and wearing a mask, to be less effective; and leave the house more frequently than, respectively, Democrats, ideological liberals, and those who disapprove of Trump. When all three measures of political worldviews are considered simultaneously, Trump approval, net of the other measures, is most strongly associated with trust in public health institutions, perceived threat of COVID-10, and beliefs about the efficacy of public health preventive measures. Political ideology is most strongly associated with beliefs about the efficacy of individualist measures and frequency of leaving the house for work. We additionally illustrate the strong effects of Trump approval on these outcome variables among those who identify as Republicans. Indeed, political worldviews—and Trump approval in particular—are as relevant—and in some cases more relevant—to perceptions of COVID-19 risk and prevention measures, as are individuals’ life circumstances that shape their daily exposure to COVID-19.
Taking these findings into account, this article makes three important theoretical contributions. First, we show the deep-seated effects that political worldviews can have on embodied practices—daily decisions about the body and perceptions of risk—which have implications for both individual health and public health. Individual COVID-19-related behaviors have tremendous ramifications for public health because they require broad-based adoption to provide population-wide protection. When a segment of the population does not comply with public health recommendations and orders, the health of the collective suffers, as we observed with states like California that experienced a resurgence of COVID-19 infection rates (McGough 2020). Our findings here—similar to the literature on vaccine refusal—have identified a lack of trust in public health authorities as a key component explaining beliefs in health behaviors, particularly the efficacy of key prevention measures like staying at home. In contrast to a vaccination decision, which is made only periodically, COVID-19 risk rejection and refusal require constant, everyday decisions about behaviors, some of which are easily observable to those around us (e.g., leaving the house). In the context of continually changing information both about the nature of the disease and the extent of its devastation, this suggests that political worldviews are playing a far more active and sustained role in guiding everyday behavior than might be the case in periodic vaccine refusal.
The second theoretical contribution concerns the relationship between the timing of a public health threat and political alignment. Based on the timing of this data collection, we show the speed with which COVID-19 beliefs and behaviors became aligned with political worldviews. Less than a month passed between crucial, life-altering, federal, state, and local political and public health guidance about the pandemic and the collection of these data. And yet, we see here that COVID-19 orientations are profoundly associated with political worldviews. We suspect four relevant processes occurred simultaneously at this time. First, the preexisting alignment between conservative political worldviews and distrust in government institutions cast doubt on official sources of information about the pandemic, leading those with conservative political worldviews to quickly dismiss the information as false or not relevant to them. Second, the segmentation of information sources and media outlets by political worldviews—and by Trump approval in particular—created variation in exposure to certain types of COVID-19-related knowledge, leading to divergent beliefs and behaviors. We were not able to directly assess the role of media consumption given our data, but other scholars can take this issue up directly. A third process, a cognitive one, meant that novel health information was interpreted and assimilated according to existing political worldviews and, among political conservatives, discounted or considered irrelevant. Fourth, over time, there was an active interpretation of particular health practices as politically segmented due to the guidance from political and media elites, such as Trump. As an example of this last process, we have seen how some public-health-endorsed COVID-19 practices that were not initially considered political, such as wearing a face mask, became politicized over time through the symbols and actions of leaders and media. So, although in these data we did not find that beliefs in the efficacy of face masks were significantly associated with political worldviews, we would expect to see an association now. Our findings indicate that in such unsettled times, not only are cultural models critical to the formation of beliefs about and behaviors toward a novel threat, but also they guide those new beliefs and behaviors almost immediately.
Finally, we show the need to disaggregate political worldviews to better understand the dimensions of politics that are guiding these new health beliefs and practices. Although many observers have noted the way that Trump’s presidency is unique, we find that this influence is also present during a moment of profound, life-threatening crisis. Even among people who identify as Republican, strong Trump approvers are less likely to trust public health institutions (particularly the WHO) and less likely to perceive a health risk from COVID-19. Furthermore, they are significantly more likely to believe in taking vitamins and using diet to prevent COVID-19 infection—two individualist strategies with no empirical support for their effectiveness as prevention measures that have not been endorsed by public health agencies. Put differently, Republicans who express low levels of Trump approval are more likely to align their beliefs and behaviors with standard public health recommendations. One key feature of the Trump presidency is the symbolic and actual separation of the president from the institutions of governance, yet the effect of this separation is not understood similarly by all political conservatives. The particular role of Trump approval is evident here, given our findings that trust in public health institutions is a mechanism by which politics, and Trump approval in particular, is associated with COVID-19 beliefs.
Another unique feature of the Trump presidency is the extent of media coverage of his statements and those of his administration, which has politicized public health measures designed to mitigate the spread and impact of the COVID-19 pandemic. The fact that Trump approval is associated with beliefs about COVID-19 among Republicans suggests that the impact of the Trump era on political attitudes is far more important than previously recognized by social scientists. In fact, our study provides some evidence that the COVID-19 crisis is creating different belief pathways among different types of political conservatives, in particular due to trust in government institutions and through media messaging; political sociologists might investigate this division in other contexts.
Scholars might take up a number of key issues related to our findings as the pandemic evolves. Future work might assess how comprehensively political worldviews shape COVID-19-relevant behaviors across contexts (e.g., practices at work, on the street, at home), how this might change over time, and how this might vary by race and gender. This focus on time and context may help scholars better understand how particular elements of public culture become the ones that individuals draw on to formulate strategies of action. Other work might examine how experiences of the pandemic may inform and change political worldviews and alliances, for example, how the pandemic has shaped support for Trump among older voters. We expect there will be a subset of the population for whom the pandemic will leave their political worldviews untouched and may create a stronger and more lasting, domain-independent relationship to those worldviews and a subset for whom the pandemic will prove transformative in changing their political worldviews and allegiances.
Additionally, scholars might examine the extent to which our findings in California can be generalized to other regions. Given the state’s liberal political context, we might expect that the relationship between politics and COVID-19 perceptions and practices might be even stronger in conservative states. Moreover, the overlap between Trump approval and Republican party identification might be less apparent in California than in other states, making it a valuable test case for examining different dimensions of political worldviews on health beliefs and behavior. Still, California is home to prominent Republican Trump supporters like Kevin McCarthy and Devin Nunes, and it may be that conservatives here are not unlike those in other regions. National-level data sets that examine multiple forms of political beliefs and worldviews would shed more light on the issue.
Finally, as Republican governors in states such as Texas change course, from downplaying the severity of the virus to openly endorsing mask-wearing and staying at home, researchers should examine the importance of politically conservative leadership at the subnational level to COVID-19 beliefs and behaviors. Can the actions of the governor of Texas, for example, promote staying at home among political conservatives—and Trump supporters in particular—in his state, or will national-level discourse undermining prevention practices continue to drive behavior?
The COVID-19 pandemic, and the accompanying physical, economic, and social destruction, has amplified the deep divides sown during the arguably more settled moments of previous years. As politics has become an increasingly important lens through which Americans view the world, and one that shapes friendship networks, cultural beliefs, and even residential choices, we see that it has also become the most powerful lens through which to understand and process the pandemic. In short, the current politically polarized environment has influenced American health beliefs and practices even during a moment of extraordinary crisis.
Supplemental Material
Supplementary_Appendix_Pandemic_Politics_Socius – Supplemental material for Pandemic Politics: Political Worldviews and COVID-19 Beliefs and Practices in an Unsettled Time
Supplemental material, Supplementary_Appendix_Pandemic_Politics_Socius for Pandemic Politics: Political Worldviews and COVID-19 Beliefs and Practices in an Unsettled Time by Hana Shepherd, Norah MacKendrick and G. Cristina Mora in Socius
Footnotes
Authors’ Note
Please note equal authorship for all authors.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.