
Abstract
Public beliefs about the causes of good and bad health are well studied but inadequately theorized. Using nationally representative survey data and a large sample (N = 6,617), this study explores the potentially conflicting roles of system justification, politics, and personal experience. The study finds evidence for system justification, at least a contingent version that allows for self-serving biases. Multivariate regression models reveal that people believe that health reflects behavior, but those in poor health are more likely to believe that health also reflects external causes. In addition, beliefs about the causes of health have a strong political dimension, consistent with a status quo of presumed personal responsibility. Conservatives are less likely to believe health is a product of the social environment. Yet personal experiences with poor health are associated with these commitments, as revealed in multiplicative interactions. Among Republicans, experiences with poor health are positively associated with a more social view of health. Beliefs about the role of government in health follow a similar pattern. Indeed, predictions from the model indicate that differences between the political right and left deteriorate as health declines, producing majority support for government intervention in health care even among those who identify as very conservative. Just as there are no atheists in foxholes, there may be some political commitments people abandon when their health fails.
Public beliefs about the causes of good and poor health are broadly consequential. They inform health behaviors, shape how people perceive others, and inform preferences regarding health policy, including universal access to care (Li et al. 2022). Yet we understand little about how people form such views, apart from studies focused on who endorses genetic causes or studies on specific domains of health, such as public beliefs regarding mental health (Shostak et al. 2009). In deriving a more complete explanation, it is useful to study beliefs about health and health policy using the same framework as social scientists use to study beliefs about economic inequality and welfare. Beliefs about health might involve a self-serving bias, with those who enjoy better health emphasizing their own discipline in achieving it (Bénabou and Tirole 2016), but beliefs about health might also reflect system justification, as when people are motivated to believe their health is within their control regardless of how healthy they are themselves (Jost and van der Toorn 2012). This study tests this idea in nationally representative data and argues that a more social psychologically informed view of health beliefs sheds light on, among other things, tentative support for national health care.
Background
Beliefs about the causes of good and bad health sit at the intersection of beliefs about luck and merit. Americans largely accept the idea that their health is not entirely in their hands. This occasionally assumes a fatalistic tone, as when people attribute disease to genes or fate, although it is usually more measured (Phelan, Cruz-Rojas, and Reiff 2002). A considerable number of Americans believe the spread of COVID was more a matter of misfortune than whether someone was vaccinated (Seddig et al. 2022). Yet Americans also think of health in terms of merit, of people deserving the health they achieve. Obesity, for instance, is seen as largely a product of a lack of willpower (Wang and Coups 2010). The idea that health is a personal responsibility is a kind of status quo, providing the philosophical backdrop to much of public health and wellness culture.
These frames have parallels in research on beliefs about inequality. Support for welfare, for instance, is shaped by who is regarded as deserving or not, much like poor health behavior diminishes the perceived responsibility of the state in ensuring access to adequate care (Watkins-Hayes and Kovalsky 2016). The inputs to beliefs about economic inequality and health might differ but only because they reflect different achievements. Education and income, for instance, are positively associated with believing the current economic system is fair (Wodtke 2012). By the same token, good personal health is associated with believing that people are personally responsible for their health and that government support is unnecessary (Grossman 2013).
Theories for Understanding Beliefs about Inequality and Health
From these elements, social psychologists have developed two general frameworks for understanding beliefs about inequality. In both cases, beliefs are motivated but in different ways, premised either on support for the existing system or on beliefs formed from success or failure within that system. Theories that emphasize a self-serving bias begin with the idea that inequality beliefs are formed to enhance self-perceptions and rationalize outcomes (Bénabou and Tirole 2016). When someone is economically successful, it is assuring to believe their wealth reflects effort and talent. System justification theory also emphasizes motivated beliefs but begins from a different premise—that people form beliefs to support the status quo rather than to enhance the self. The theory also posits, however, that motivated beliefs can support self-respect even when they imply self-blame. According to the theory, accepting the status quo can promote self-respect because system justification is itself palliative (Jost and Hunyady 2005). System justification reduces anxiety, guilt, and cognitive dissonance among both the disadvantaged and advantaged because justification supports the idea that the system is fair, just, and legitimate. In contrast to a self-serving bias, system justification theory assumes that personal experiences need not diminish support for meritocracy. In system justification theory, there is no dissonance when faith in the justness of the system is not met with the realization of success.
There are other real parallels between beliefs about health and inequality. Both types of beliefs may be influenced by politics (e.g., Jensen and Petersen 2017). In the United States, politics informs who is regarded as deserving or undeserving of poverty. By the same token, support for Medicaid is often premised on whether people believe its recipients need health care or ought to work for it (Haeder, Sylvester, and Callaghan 2021). Drawing on a political philosophy can help to support system justification, especially when it supports the status quo. Political conservatism provides a belief system that explains social and economic outcomes in ways that legitimate the status quo, whereas liberalism is more challenging of it (Jost and Hunyady 2005). Moral justification theory further argues that liberals and conservatives have different moral bases for their beliefs (Day et al. 2014). Whereas conservatives rely on ingroup loyalty and authority, liberals rely on fairness and harm avoidance. Although casting issues in moral terms tends to entrench preexisting beliefs, there is some evidence that conservatives will shift in a more liberal direction if otherwise liberal issues are cast in a conservative moral frame (Day et al. 2014).
It is possible that the motivation behind system justification is sufficiently strong to moderate the impact of personal experiences with success or failure and, thus, to temper more plainly self-serving beliefs or political leanings. In this vein, personal experience is often decisive in shaping beliefs about economic inequality, as when economic failure diminishes support for personal causes (Wetter and Finger 2023). This has potential parallels in beliefs about health. Those in good health might be more inclined to attribute their health to effort and personal responsibility, especially if they also endorse more right-leaning politics. But they might be more swayed by setbacks, reconsidering their beliefs when they experience the “failure” of declining health. Political beliefs can thus provide a rationale for system justification, one that is diminished only when personal experience contravenes.
Testing Self-serving Beliefs and System Justification
In this study, I test system justification theory with respect to health beliefs. I also test whether system justification competes with self-serving beliefs under conditions where they are presumably in conflict. The hypotheses are as follows:
Data
Data from this study are drawn from the 2019–2020 wave of the American Health Values Survey, the second wave of a two-part series (Bye and Ghirardelli 2025). The survey was administered using an address-based sample. The data were collected using multiple modalities following an initial mail invitation asking recipients to participate in a web-based survey. A second sample was included, which combined the address-based sample with a sample from the AmeriSpeak panel, a probability-based online national survey. Survey weights were used in all the analyses to ensure representativeness. Weights were constructed based on the probability of selection and nonresponse at the interview stage. The weights were then crafted to ensure the sum approximated the U.S. population distribution by age, gender, race-ethnicity, educational attainment, and census division according to Current Population Survey data. Although well crafted, the use of weights does not produce substantially different results from unweighted analyses, especially in multivariate models. The weighted sample is younger (by about five years) and somewhat healthier, although the relationship between health and beliefs about health is nearly identical in weighted and unweighted multivariate models. There was little missing data from item nonresponse, and the analyses employ listwise deletion for the remaining missing values.
Variables
Beliefs about health
Respondents were asked a series of questions regarding their beliefs about the causes of good and poor health. They were presented with a list of “things that may affect people's health in either a positive or negative way” and were asked whether the proffered cause had “no effect,” scored as 1, or a “very strong effect,” scored as a 5. The list included access to health care, having a job, stress, quality of food available in the community, having health insurance, smoking, personal health practices, air and water quality, genetic makeup inherited from parents, community safety, housing quality, education, and the community that a person lives in. Factor analysis provided general support for a single factor, although three items were less strongly related to that single factor: smoking, personal health practices, and genetics. The question regarding genetics was dropped because it was not clearly associated with any factor. From the remaining set of items, I created two summary dimensions: support for personal causes (consisting of smoking and personal health practices) and support for external causes (consisting of the remaining items). Both dimensions are coded as the mean of the items within them.
This study also considers beliefs regarding who is responsible for addressing inequality. A subset was asked whether they agree or disagree with the following statement: “It is the obligation of the government to ensure that everyone has access to health care as fundamental right.” The outcome was scored as 1 for “agree” and 0 for “disagree” and modeled as the probability of support using logistic regression. To assess the consistency of the results relative to those found with respect to beliefs regarding socioeconomic outcomes, an additional variable was considered. A subset of respondents was asked, “Would you say that everyone has about the same opportunity to succeed in American society or that some people have less opportunity than others?” The outcome was scored as 1 for “everyone has the same opportunity” and 0 for “some people have less than others.”
Health
I employ two measures of health. Respondents were asked whether their health in general was excellent, very good, good, fair, or poor, scored directionally as poor health (e.g., 1 = excellent, 5 = poor). In addition, respondents were asked a serious of questions regarding specific health events and medical conditions (as diagnosed by a doctor), including high cholesterol; high blood pressure; heart attack; angina or coronary heart disease; stroke; any kind of diabetes or high blood sugar; cancer (other than skin cancer); emphysema, asthma, or chronic obstructive pulmonary disease; depression; and anxiety or other mental or emotional condition. The regression models include the total number of health problems, although in sensitivity analyses, I separated the mental and physical conditions.
Political orientation
Political orientation was assessed via a question regarding how respondents would describe their political views on a spectrum, as very liberal, liberal, moderate, conservative, or very conservative. When used in most regression models, the variable was scored as a continuous 1 to 5, left to right, and referred to as “politically conservative orientation” in reference to its direction. Supplementary models supported the fit of models using a continuous score relative to a categorical specification. In addition, respondents were asked their party affiliation, whether they considered themselves a Republican, Democrat, or independent.
Other variables
The models also include age, gender, race (specified as non-Hispanic white, black, Asian or Pacific Islander, Hispanic, multiple, and other), and education (specified as high school graduate, some college, or bachelor's degree or higher, all relative to less than high school).
The statistical models are all based on weighted linear regression with the exception of Table 4, which employs a categorical dependent variable and uses logistic regression. The models are additive with the exception of models that test Hypothesis 3, which involves a multiplicative interaction between poor health and political orientation, estimated to test whether poor health has a stronger relationship with policy preferences for those with a right-leaning political orientation.
Results
Table 1 presents descriptive statistics. In general, support for personal causes is greater than support for external causes, although the two types of explanation are not strictly in competition. The average support for personal causes is 4.521, whereas the average support for external causes is 4.078 (difference significant at p < .001). The correlation between the two measures is moderately positive (.287). In addition, support for government intervention in health care is high. About three-fourths agree that it is the government's obligation to guarantee health care (and only 24 percent believe that everyone in the United States has the same opportunities for upward mobility). Political moderation is frequent. About 40 percent of people indicate that they are moderate on the political spectrum.
Summary Statistics, American Health Values Survey 2019–2020.

Note: N is 6,617 for all variables except for government obligation to ensure access to care (N = 3,215) and belief in equal opportunity (N = 3,192).
Table 2 presents the first set of regression tables. Although the main results are presented as coefficients, the figures present margins to allow for easier interpretation. The first pair of models suggests that support for external causes is more elastic than support for personal causes. Poor health increases support for external causes, as does a more liberal political orientation. Political orientation has an especially strong association with beliefs about the causes of health. The expected score among those who are very liberal is 4.425, whereas among those who are very conservative, it is 3.751, approximately the same as the lowest average level of endorsement of any one item. In addition, the gap between personal and external causes grows larger with more conservative views. Among those who say they are very liberal, for instance, the difference between personal and external causes is .150, whereas among those who say they are very conservative, the difference is .654. Health itself is not associated with such a wide range in beliefs. Those who are in poor health report, on average, a score of 4.119 for the support for external causes measure, whereas those in excellent health report 4.049. But poor health is strongly implicated in support for personal causes. As health deteriorates, support for personal causes goes down, with a coefficient that is about three times the size as that for external causes. Political orientation is not associated with support for personal causes, meaning politics appears to enter on only one side of the spectrum of beliefs.
Linear Regression of Beliefs in the Causes of Health on Health and Political Orientation, American Health Values Survey 2019–2020.

Note: Standard errors are in parentheses. Reference categories are male, less than high school, and non-Hispanic white.
p < .05, **p < .01, ***p < .001.
Of note, health beliefs parallel beliefs about inequality, at least with respect to the influence of other demographic factors. Although all racial groups appear to endorse personal causes, racial minorities are more likely to endorse external causes. In addition, education is positively associated with endorsement of personal causes (but not external). In the case of race, the coefficient would be much larger were it not for the fact that the model also includes poor health and political orientation.
Table 2 also presents models with interactions between health and political orientation. For support for external causes, health has much more of an association with support among conservatives than liberals. Among those who identify as very conservative, the association is .069, whereas among those who identify as liberal (or very liberal), the association is statistically indistinguishable from zero. Marginal effects are presented in Figure 1. Among those who are more politically conservative, health has a much stronger association with the outcome. Poor health is more strongly associated with a shift toward external causes. The multiplicative interaction is not significant for personal causes, although the direction of the interaction is the same for external causes. Among conservatives, these interactions imply that poor health encourages a more balanced view of the causes of health. For instance, among those who say they are very conservative and in poor health, the difference between personal and external causes is a mere .088, less than the average difference among those who say they are very liberal (.150).
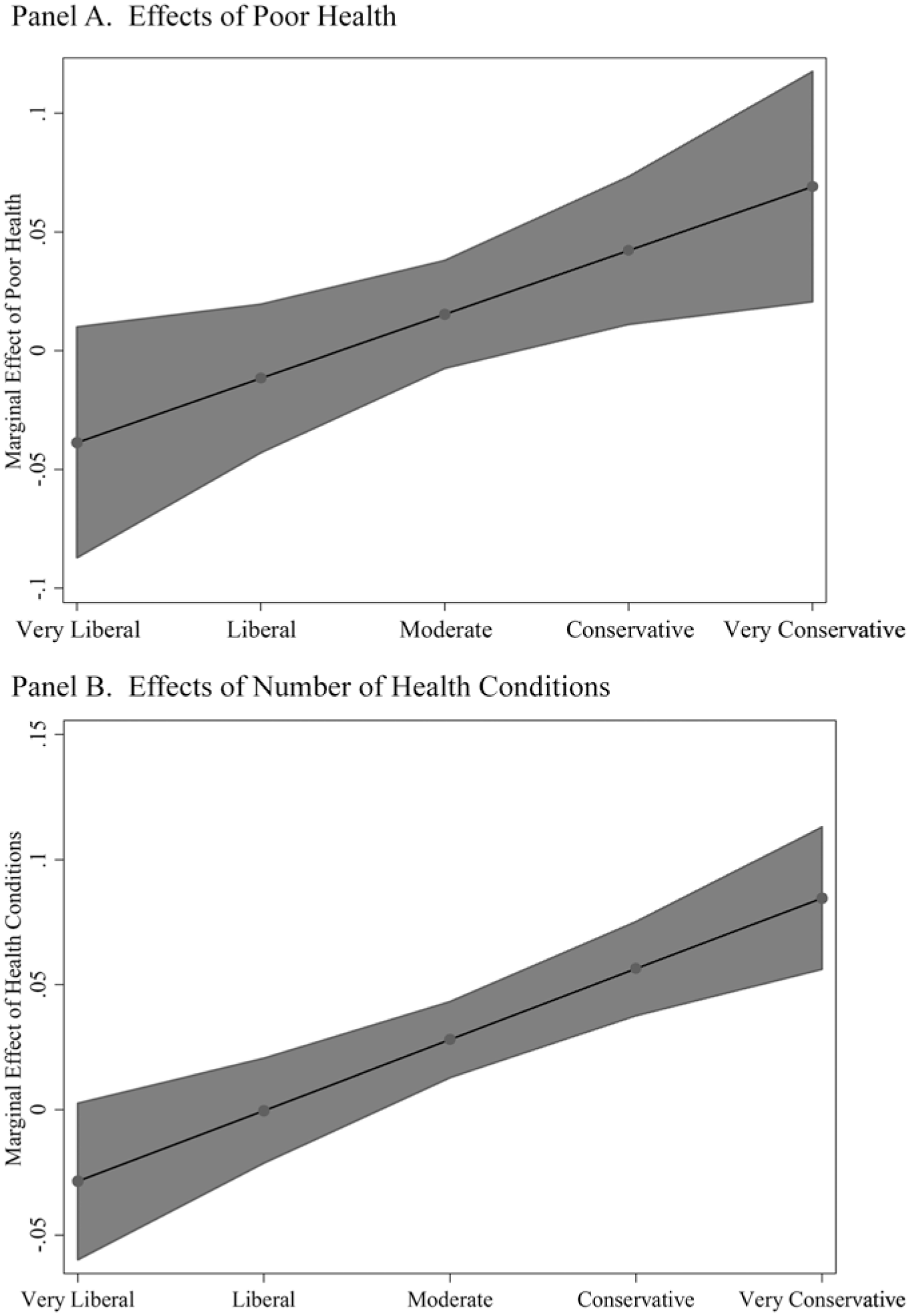
Marginal effects of health on belief in external causes by political orientation..
One potential concern in these models is that self-rated poor health confounds health with beliefs about health, producing an artificially strong relationship between self-rated health and health beliefs. There is some evidence for confounding of this sort. In research on the effects of health on personality and beliefs, economists have raised similar concerns, questioning whether physical health shocks, for instance, are as significant as mental health shocks (Bünnings, Simankova, and Tauchmann 2025). As a sensitivity test, Table 3 estimates the same models using an objective measure of health, including survey items framed specifically in terms of a diagnosis. The patterns are similar, albeit with more statistical power and a somewhat larger interaction. Among those with conservative political leanings, the total number of health problems is positively associated with support for external causes, but among liberals, the association is insignificant. The marginal effects of poor health are −.021 among Democrats (p = .266), .013 among independents (p = .514), and .072 among Republicans (p = .000). The measure is a simple sum of ten items. In another sensitivity test, I explored interactions with each item separately, testing whether mental health matters more than physical health. The models provide no evidence for a distinction. The models (not shown) revealed, for instance, that both mental health problems and high blood pressure were significantly associated with health beliefs.
Linear Regression of Beliefs in the Causes of Health on Alternative Indicators of Health and Political Orientation, American Health Values Survey 2019–2020.

Note: Standard errors are in parentheses. Reference categories are Democrat, male, less than high school, and non-Hispanic white.
p < .05, **p < .01, ***p < .001.
Political orientation is not perfectly in sync with party identification, especially in the United States. In the survey, about ten percent of Democrats identify as conservative, and 37 percent identify as moderate. It is useful to test the same interactions for political parties rather than political orientation. Table 3 presents these interactions and confirms the prior results. The group most subject to change—presuming a causal association—is conservatives. Among Republicans, the association between self-rated health and external causes is significant and positive, whereas among both Democrats and independents, the association is insignificant.
The political substrate of health beliefs is strong. Health beliefs are consequential for health policy because beliefs about the causes of poor health speak to who is responsible for ensuring better health outcomes. Table 4 presents the same model specification but explores support for the idea that the government is obligated to ensure access to care and support for the idea that everyone in the United States has the same opportunity to succeed. Personal experiences with poor health are, among conservatives, more transformative than simply changing beliefs regarding the causes of health. Among conservatives, support for the idea that the government is obligated to provide care is low, falling below 50 percent. Nonetheless, personal experiences with poor health temper this belief and, indeed, virtually eliminate the difference between liberals and conservatives. Figure 2 presents the proportion supporting a government obligation over the intersection of political orientation and health. Among conservatives, the influence of health is substantial, whereas among liberals it is not. The correlation with poor health is sufficiently strong to virtually eliminate differences between liberals, conservatives, and moderates in their support. The same interaction is not found with respect to beliefs regarding success in general, suggesting the tempering effects of health are specific to health beliefs. Conservatives are far more likely to support the idea that everyone has an equal opportunity for success in the United States, and poor health plays no role in shaping their support. Of note, however, there is an interaction between political orientation and education, as might be expected if beliefs regarding inequality are affected more by personal experiences with education than with health. Among those who say they are very conservative, a bachelor's degree increases support for equal opportunity, whereas among those who say they are very liberal, it decreases it (results not shown). Interpreting these models together suggests that the tempering influence of personal experience depends on the domain of the “success.” Research on inequality beliefs can be transposed to health beliefs, recognizing their different inputs.
Logit Regression of Beliefs about the Causes of Health on Health and Political Orientation, American Health Values Survey 2019–2020.

Note: Standard errors are in parentheses. Reference categories are male, less than high school, and non-Hispanic white.
p < .05, **p < .01, ***p < .001.

Expected probability of support for a government obligation to ensure access to health care, by political orientation and health..
Discussion
Sociologists have demonstrated that “winners” and “losers” have different beliefs regarding the causes of economic inequality and that American beliefs regarding inequality are premised on system justification (Jost and Hunyady 2005). Americans are vested in the economic status quo and see abundant opportunities for success, and sometimes these beliefs are set to the point that they are impervious to changing personal economic circumstance. The same appears true of health, at least in part. Americans recognize some social causes to poor health but endorse personal causes more. Support for the idea that health is shaped by external causes is especially weak among conservatives, and personally maintaining good health appears to further solidify the belief that health is determined by good choices and behavior. The same pattern extends to support for the role of government in improving access to care. Yet the results also suggest that experiences with poor health yield some retrenchment in system justification. Experiences with “failure” encourage the idea that health is shaped by external factors, especially among those who are most predisposed to seeing poor health as a matter of personal responsibility. Among those who already see a role for the social environment in health, personal health experiences are less transformative, suggesting a precommitment to the idea that health reflects both personal and external influences.
In this way, the results point to the importance of poor health for challenging system justification, much like downward mobility can undermine support for an economic status quo. Assuming a causal relationship, poor health changes the beliefs of political conservatives, much like downward mobility can change their beliefs regarding inequality. The association of poor health with support for external causes was more than twice as large among those who identify as very conservative relative to those who identify as moderate. The association of poor health with support for government interventions in health care is sufficiently robust to move conservatives to majority support. When in self-reported excellent health, only 23 percent of those who identify as very conservative support the role of government in ensuring access to health care, but when their health becomes poor, this support increases to 59 percent.
The importance of health in health beliefs is further illustrated by its role in collapsing political polarization. Among those in poor health, there are very few differences among liberals and conservatives in their support for a role of government in health care. Indeed, the survey question was framed in an explicitly progressive fashion, asking respondents whether they thought such a role was a “fundamental right,” precisely the kind of framing that might ordinarily cue a strong partisanship response. Even with this framing, however, differences between conservatives and liberals dissolved given that most in each group endorsed the view if their health was poor. This finding has implications for health policy because it suggests that support for the status quo in the United States, as strong as it might be, can deteriorate. In general, public support for the Affordable Care Act has crystallized along economic and political lines, although support for the act has increased over time, as more people have come to rely on its provisions (Corman and Levin 2016). Absent a strong need for care, then, the influence of political ideology is likely to be decisive, but a sense of vulnerability might be sufficient to diminish ideological opposition.
This study has several limitations. For one, the results are based on a cross-sectional survey. Most theories allow for the role of success or failure in changing beliefs, but it is possible that health beliefs shape health itself rather than the reverse, as when better health behavior is motivated by confidence that one's health will improve as a result. Reverse causality seems unlikely in this case, however, given the specific results. The present study found that those who most emphasize health behavior are also those most affected by poor health, meaning reverse causation would imply that those most convinced that their health behavior matters engage in worse health behaviors. By the same token, this study assumes that political orientation shapes beliefs, although it is possible that people grow more conservative or liberal based on changes in their health. A study of quasi-random injuries might be better able to address endogeneity of this sort.
Conclusion
In understanding beliefs regarding economic inequality, studies have often cast their findings in terms of a tug-of-war between self-serving biases and a precommitment to the status quo. In the current study, however, the status quo of health is supported by the better health of those most invested in that status quo. So long as people remain in good health, the American public is likely to prefer a limited role of government, and health will intersect with politics in ways that enhance that status quo further. In the current study, Republicans (whose beliefs appear most sensitive) report somewhat better health than Democrats. On average, about 54 percent of Republicans report excellent or very good health compared to 45 percent of Democrats. The belief that health is a personal responsibility might be sustainable only insofar as health is generally favorable in the United States and so long as those who are most invested in the status quo continue to maintain an advantage. This pattern aligns with other studies. The COVID-19 pandemic, for instance, had a scarring effect on public beliefs, increasing the fear of extreme negative shocks in the future (Kozlowski, Veldkamp, and Venkateswaran 2020). Once a shock is felt, it changes belief formation going forward, regardless of the confidence people enjoyed before. Significant reforms to the health care system might only be possible when people realize through experience and events what their ideologies and politics did not teach them before.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.