
Abstract
Introduction
Physical assessment is a fundamental component of nursing practice, yet various barriers can limit its use in clinical settings.
Objectives
To evaluate the construct validity and reliability of a culturally adapted, French-language version of the Barriers to Nurses’ Use of Physical Assessment Scale.
Methods
We conducted a cultural adaptation and validation study, using secondary data analysis. Data were collected using three cross-sectional surveys conducted among nurses working in surgical, geriatrics and rehabilitation units in French-speaking Switzerland (N = 246). Psychometric evaluations included both exploratory and confirmatory factor analyses to assess construct validity, and Cronbach's alpha was calculated to determine internal consistency.
Results
The Kaiser–Meyer–Olkin sampling adequacy value was 0.848, and Bartlett's test of sphericity was significant (p < .001), confirming the data's suitability for factor analysis. We identified a seven-factor structure (similar to the original scale) that explained 54.6% of the total variance. The 38-item scale's overall internal consistency was excellent (α = .89). However, the Speciality Area (α = .47) and Ward Culture (α = .29) subscales demonstrated lower reliability, indicating a need for further refinement.
Conclusion
The French-language version of the Barriers to Nurses’ Use of Physical Assessment Scale is a reliable, valid instrument for measuring nurses’ perceptions of the barriers to them using their physical assessment skills. Further research is recommended to improve the internal consistency of some subscales and to validate these findings across diverse clinical settings.
Patient or Public Contribution
This study did not include patient or public involvement in its design, conduct, or reporting.
Introduction
Physical assessment is a fundamental nursing skill and part of the standard nursing scope of practice (D’Amour et al., 2012). It plays a key role in safe patient care by allowing nurses to evaluate a patient's condition and detect early signs of deterioration (Wiseman et al., 2024). However, according to the World Health Organization (WHO), one in 10 patients in high-income countries experiences harm while receiving hospital care, with nearly half of these incidents being preventable (WHO, 2021). In low- and middle-income countries, unsafe healthcare practices cause 134 million adverse events each year, leading to 2.6 million deaths (WHO, 2021). Failure to recognize at-risk patients and intervene early in cases of clinical deterioration are key factors contributing to adverse patient outcomes, prolonged hospital stays and increased healthcare costs (Fernando-Canavan et al., 2021).
Research shows that nurses’ roles are critical to “rescuing” patients from life-threatening complications (Nielsen et al., 2022; Phillips et al., 2019). Higher rates of care by registered nurses (RNs) are linked to lower rates of “failure to rescue” (FTR) (Parker, 2024; Sloane et al., 2018), which refers to deaths after complications (Hall et al., 2020). Hamlin et al.'s (2023) cohort study showed that having nurses carry out systematic physical assessments could significantly reduce delays in recognizing a patient's deteriorating condition, rates of admission to intensive care units and mortality rates. Regular physical assessment is a key component of the clinical assessment process; it involves the systematic and continuous collection of patient data through the techniques of inspection, auscultation, percussion, and palpation (Fennessey & Wittmann-Price, 2011; Jarvis & Eckhardt, 2024).
However, numerous studies have shown that nurses do not regularly integrate comprehensive physical assessments into their daily practice and use only a small number of their physical assessment skills (Burdeu et al., 2021; Dalton et al., 2018; Fontenot et al., 2022; Morrell et al., 2021).
Literature Review
The literature reports that nurses recognize the value of performing physical assessments but face many challenges that hinder them from using their physical assessment skills in clinical settings (Gharaibeh et al., 2022; Rosli et al., 2023). Numerous observational studies have examined barriers to nurses using physical assessment, highlighting the lack of role models, a lack of training, a lack of self-confidence in assessment skills, reliance on other professionals and technology to determine a patient's clinical status, and a lack of support and encouragement to perform physical assessments, and even the influence of cultural differences (Douglas et al., 2014; Gharaibeh et al., 2022; Gülnar et al., 2022; Liyew et al., 2021; Osborne et al., 2015; Rosli et al., 2023; Shi et al., 2020).
Some descriptive studies carried out in Switzerland also revealed that nurses did not consistently perform physical assessments as part of their daily clinical practice due to specific barriers. These were mainly related to their nursing speciality area, the lack of nursing role models and time, and interruptions (Da Veiga Gonçalves et al., 2023; Epiney-Perruchoud, 2019; Gomes Fernandes, 2019).
Douglas et al. (2014) inductively developed and psychometrically validated the main constructs of an instrument designed to measure barriers to nurses’ use of physical assessment in acute care settings. This scale garnered significant interest and was used in numerous surveys in a variety of countries to identify obstacles to the use of physical assessments in nursing practice (Alamri & Almazan, 2018; Da Veiga Gonçalves et al., 2023; Liyew et al., 2021; Osborne et al., 2015; Turan et al., 2022).
To the best of our knowledge, the Barriers to Nurses’ Use of the Physical Assessment Scale, developed by Douglas et al. (2014), has been translated and psychometrically validated in Turkish (Gülnar et al., 2022). Gomes Fernandes and Epiney-Perruchoud translated and culturally adapted this scale in French in 2019, but did not evaluate the psychometric properties of the translated version (Epiney-Perruchoud, 2019; Gomes Fernandes, 2019). Given nurses’ crucial role in rapidly detecting deterioration in acute healthcare settings and rescuing patients from complications, barriers to nurses using physical assessments must be addressed using properly translated and psychometrically tested instruments for RNs working in French-speaking regions.
This study aimed to evaluate the construct validity and internal consistency of a culturally adapted French-language version of the Barriers to Nurses’ Use of Physical Assessment Scale, using secondary data analysis. We hypothesized that the French version would retain a multidimensional structure comparable to the original scale and demonstrate satisfactory reliability across most subscales, and that perceived barriers may vary according to nurses’ sociodemographic and professional characteristics.
Methods
Design
This study was a secondary analysis of existing data from three cross-sectional, multicenter surveys assessing Douglas et al.'s (2014) Barriers to Nurses’ Use of Physical Assessment Scale in healthcare settings in Switzerland's French-speaking regions. It specifically examined its properties of internal consistency and construct validity. This methodological study was based on the framework developed by Waltz et al. (2016) and was conducted in accordance with the COSMIN (COnsensus-based Standards for the selection of health Measurement INstruments) guidelines to ensure methodological rigor in the evaluation of the instrument's measurement properties (de Vet et al., 2011).
Study Setting, Sampling, and Data Collection
The research population consisted of nurses working in surgical and geriatrics wards of the Valais Hospital, as well as eight rehabilitation care units across the cantons of Vaud and Valais in the French-speaking part of Switzerland. The inclusion criterion required holding a Swiss nursing diploma from a specialist school, a university of applied sciences or a recognized foreign equivalent. Exclusion criteria ruled out temporary staff, pool nurses and those with less than three months of experience.
Data were collected through self-administered questionnaires, which were emailed to eligible participants and were followed by reminder emails at two, four, and eight weeks. Each questionnaire was accompanied by written information detailing the study's objectives, participation conditions and data confidentiality. Completing the questionnaire was considered as written informed consent, ensuring participant anonymity.
The data were drawn from cross-sectional multicenter surveys conducted between 2019 and 2020 by Gomes Fernandes (2019), Epiney-Perruchoud (2019), and Da Veiga Gonçalves et al. (2023), which involved nurses from the designated wards, with 66, 68, and 112 participants, respectively. The final sample for the psychometric study comprised 246 participants.
Authorization was obtained from the original instrument's authors prior to the multicenter surveys (Douglas et al., 2014). Based on Gunawan et al. (2021), our sample size of 246 is considered fair-to-good for testing the scale's psychometric properties.
Cultural Adaptation and Translation of the Barriers to Nurses’ Use of the Physical Assessment Scale Into French
Translation into French and cultural adaptations were conducted by Gomes Fernandes (2019) and Epiney-Perruchoud (2019) and guided by the 10 stages recommended by Wild et al. (2005). Two items on the scale were improved after checking their back translation against the original scale and discussing them with their author, as the differences seemed significant. After three cognitive debriefings with nursing professionals with differing levels of training, some items were reformulated more precisely; this clarified and improved their overall comprehension of the questions. A pilot test of the scale's final version was conducted with five nursing professionals with sociodemographic and professional characteristics similar to those of the eligible participants. This step allowed final adjustments to be made to the questionnaire's instructions and presentation. Finally, the French version (Supplemental File 1) underwent the same psychometric testing as the original scale (Douglas et al., 2014).
The Original Scale
The scale is composed of 38 items divided into seven subscales representing the following barriers to nursing physical assessment: Reliance on Others and Technology (nine items), Lack of Time and Interruptions (six items), Speciality Area (five items), Lack of Influence on Patient Care (four items), Lack of Nursing Role Models (four items), Ward Culture (six items), and Lack of Confidence (four items). The original study results demonstrated adequate item performance without evidence of floor or ceiling effects (Douglas et al., 2014). Respondents could respond to each item on a 5-point Likert scale ranging from 1 (completely disagree) to 5 (completely agree). Following the original study methodology, a score was calculated for each subscale. In the final original instrument, seven factors were jointly responsible for 57.7% of the variance (Douglas et al., 2014). The construction of the subscales was based on a principal component analysis (PCA) extraction in a varimax rotation after exploratory factor analysis (EFA). Reliability analysis showed the scale to be internally consistent, with Cronbach's coefficient alpha ranging from .70 to .86 for each subscale and .80 for the total 38-item scale. The correlations between these subscales ranged from .03 (Speciality Area and Lack of Influence on Patient Care) to .61 (Lack of Nursing Role Models and Ward Culture).
Statistical Analysis
Our analysis involved descriptive (absolute and relative frequencies, means and their standard deviations) and inferential statistical calculations. EFA was conducted to explore the underlying structure of the scale and identify latent constructs, followed by confirmatory factor analysis (CFA) to evaluate the fit of the proposed factor structure (de Vet et al., 2011). Prior to conducting factor analysis, the suitability of the dataset was assessed using the Kaiser–Meyer–Olkin (KMO) test, which evaluates sampling adequacy, and Bartlett's test of sphericity, which confirms that correlations between items are sufficient for factor analysis. Factors were extracted using the principal component method with varimax rotation, and those with eigenvalues > 1 were retained. The extraction of factors was guided by the theoretical framework of Douglas et al. (2014).
Internal consistency indicates the degree to which items within a scale are interrelated and measure the same underlying construct (de Vet et al., 2011). Cronbach's alpha (α) quantifies this consistency, with values ≥ .70 considered acceptable, ≥ .80 good, and ≥ .90 excellent; lower values may reflect heterogeneity among items or insufficient representation of the construct (Tavakol & Dennick, 2011).
Convergent validity was examined using two indicators: composite reliability (CR) and average variance extracted (AVE). CR values above 0.70 were considered acceptable, indicating adequate internal consistency. AVE values equal to or > 0.50 were used as a criterion for sufficient convergence, reflecting the proportion of variance explained by the latent construct relative to measurement error. Discriminant validity was assessed by comparing the AVE of each subscale with its maximum shared variance (MSV). A subscale was considered to demonstrate adequate discriminant validity when its AVE exceeded its MSV, indicating that the construct shares more variance with its own items than with other constructs in the model.
Inferential analyses included Pearson's correlation coefficient, Student's t-tests, and multivariate analysis of variance (MANOVA). Pearson's correlation (r) was used to examine associations between subscale scores and between subscale scores and continuous participant characteristics (e.g., years of experience, testing the hypothesis that greater experience is associated with lower or higher perceived barriers), with values closer to ±1 indicating stronger associations. Student's t-tests compared subscale means between two independent groups (e.g., female vs. male, bachelor's degree vs. qualification before bachelor's degree requirement), testing whether perceived barriers differed between groups. MANOVA assessed the combined effect of participants’ sociodemographic and professional characteristics on all subscale scores simultaneously, accounting for correlations among subscales, and testing the hypothesis that sociodemographic and professional factors jointly influence nurses’ perceptions of barriers.
The normality of distributions was accepted in samples larger than 30, as per the central limit theorem. Box's M test was used to analyze the homogeneity of our covariance matrix; Levene's test was used to analyze the homogeneity of individual variances. The significance level for rejecting our null hypotheses was set at α ≤ .05. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS, Version 28 for Windows) and Analysis of Moments Structures software (AMOS, Version 24).
Ethical Considerations
The original studies providing the data for this research were approved by a Swiss university hospital's Research Application Review Board (No. 2020-12). By returning their questionnaires to investigators, respondents tacitly consented to participating in those studies and agreed to the conditions of participation. Nurses’ participation in the studies was voluntary, and they were free to cease completing their questionnaires at any time. All the study methodologies were followed in accordance with their relevant guidelines and regulations.
Results
Sample Characteristics
The sample consisted of 246 sets of responses. The mean participant age was 36.9 years old, ranging from 22 to 64. The majority were female (84.1%), had a bachelor's degree (61.4%), were frontline nurses (79.7%) and worked in rehabilitation (45.5%). The average number of years of professional experience was 12.6 (SD = 11.1) (Table 1).
Participants’ Sociodemographic and Professional Characteristics (N = 246).

Abbreviations: M = mean; SD = standard deviation.
Construct Validity (EFA and CFA)
The EFA of the 38 items of the Barriers to Nurses’ Use of Physical Assessment Scale initially converged on a solution with 10 principal components, explaining 63.5% of the total variance. A seven-factor structure was subsequently extracted to align with the theoretical framework proposed by Douglas et al. (2014). The Kaiser–Meyer–Olkin (KMO) test indicated good sampling adequacy (0.848), and Bartlett's test of sphericity was significant (p ≤ .001), supporting the suitability of the data for factor analysis.
The EFA with this seven-factor structure explained 54.6% of the total variance. The first factor, Lack of Time and Interruptions, explained 21.4% of the total variance. This factor included items related to workload, frequent interruptions, and time constraints, with strong factor loadings ranging from 0.69 to 0.85. The second factor, Lack of Nursing Role Models, explained 9.6% of the variance. Items reflected the presence (or absence) of professional support, the promotion of leadership skills, and role models within nursing teams, with loadings ranging from 0.38 to 0.75. The third factor, Lack of Confidence, accounted for 7.2% of the variance. This factor included items related to nurses’ self-efficacy, such as doubts about their ability to perform physical assessments accurately and confidently. Reliance on Others and Technology emerged as the fourth factor, explaining 5.4% of the variance. Items highlighted nurses’ dependency on monitoring devices and the perception that physical assessments fall under the responsibility of other healthcare professionals. The fifth factor, Speciality Area, accounted for 4.0% of the variance. This factor included items describing how specific clinical settings influenced the use of physical assessment skills, with moderate factor loadings from 0.69 to 0.75. Lack of Influence on Patient Care emerged as the sixth factor, explaining 3.6% of the variance. This factor reflected nurses’ perceptions of their assessments’ influence on clinical decision-making and patient care outcomes. Lastly, Ward Culture accounted for 3.4% of the variance. Factors loadings > 0.30 for each component are presented in Table 2. Items were retained on their primary factor if loadings exceeded 0.40. A few items showed cross-loadings above 0.30, notably item 11, which loaded moderately on Lack of Time and Interruptions, Reliance on Others and Technology, and Speciality Area, suggesting some overlap between these constructs. For items with cross-loadings above 0.30, retention was determined by considering theoretical relevance and alignment with the original scale structure (Douglas et al., 2014). No items were removed, as cross-loadings did not compromise the interpretability of the seven-factor solution.
Rotated Component Matrix.

Note: Loadings >0.40 indicate primary loadings; * marks cross-loadings > 0.30. Negative values indicate inverse relationships.
The seven-factor structure was also tested using CFA (Figure 1). The values obtained—χ2/df = 1.701, CFI = 0.86, TLI = 0.85, RMSEA = 0.054, and RMSR = 0.07—indicated a good quality of adjustment. The CFA model implied the correlation of errors 3 and 6, 36 and 37.

Confirmatory factor analysis of the Barriers to Nurses' Use of Physical Assessment Scale adjusted to a sample of 246 respondents.
Thus, based on the values obtained in the EFA and CFA, we decided to maintain the composition of the seven subscales defined by Douglas et al. (2014).
Reliability (Internal Consistency)
The internal consistency of the seven factors varied across the scale (Table 2). Lack of Time and Interruptions and Lack of Confidence demonstrated excellent reliability (α = .84 and α = .88, respectively). Lack of Nursing Role Models and Reliance on Others and Technology showed acceptable reliability (α = .70 for both factors). Lack of Influence on Patient Care exhibited good reliability (α = .77), whereas Speciality Area and Ward Culture demonstrated poor internal consistency (α = .47 and α = .29, respectively), indicating limited coherence among the items within these factors. For Speciality Area, corrected item-total correlations ranged from 0.235 to 0.602, with item 35 showing the weakest correlation (0.235); its removal would increase Cronbach's alpha to .686. Similarly, in the Ward Culture subscale, item-total correlations ranged from 0.175 to 0.566, with most items showing acceptable correlations, except for item 4 (0.175), whose removal would raise Cronbach's alpha to .738.
The overall 38-item scale's alpha coefficient was .89.
Convergent and Discriminant Validity
The values for convergent validity were all above 0.70, indicating strong correlations between the items within the same construct. Specifically, CR values exceeded the recommended threshold of 0.70 for all subscales, while AVE values were acceptable for Lack of Time and Interruptions (0.510) and Lack of Confidence (0.654).
The subscales Lack of Confidence (AVE = 0.654; MSV = 0.347), Lack of Time and Interruptions (AVE = 0.510; MSV = 0.317), and Speciality Area (AVE = 0.345; MSV = 0.229) satisfied the criterion for discriminant validity, with AVE values exceeding the corresponding MSV values. In contrast, the subscales Ward Culture (AVE = 0.313; MSV = 0.538), Lack of Nursing Role Models (AVE = 0.408; MSV = 0.538), Lack of Influence on Patient Care (AVE = 0.381; MSV = 0.526), and Reliance on Others and Technology (AVE = 0.262; MSV = 0.395) did not meet the criterion, suggesting insufficient discriminant validity for these dimensions (Table 3).
Convergent and Discriminant Validity.
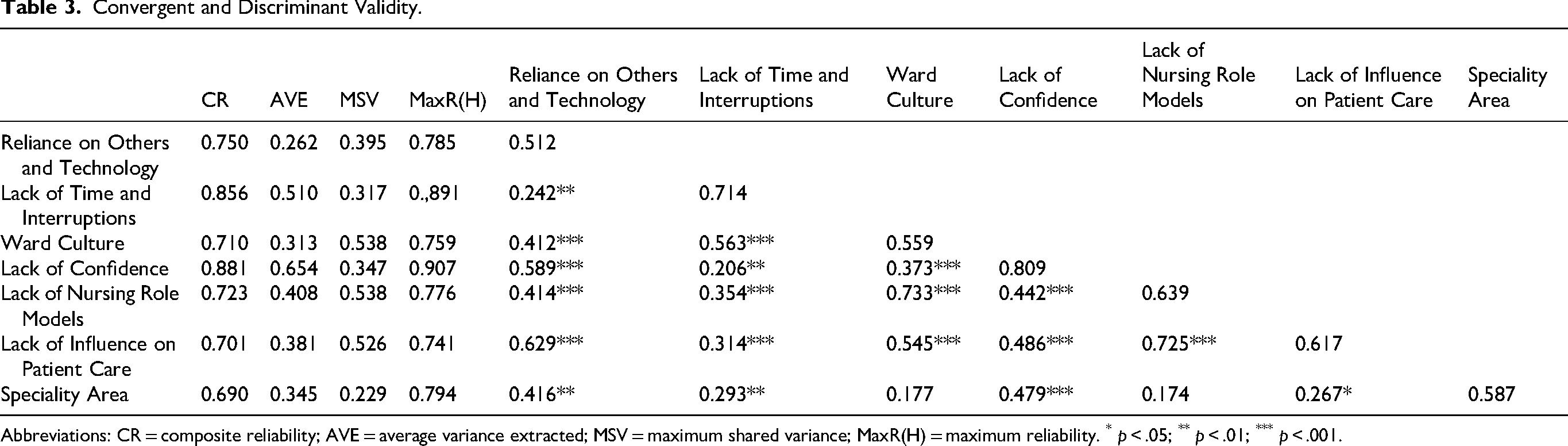
Abbreviations: CR = composite reliability; AVE = average variance extracted; MSV = maximum shared variance; MaxR(H) = maximum reliability. * p < .05; ** p < .01; *** p < .001.
Descriptive Statistics of the Subscales
Descriptive statistics of the subscales are presented in Table 4, with minimums, maximums, means and their standard deviations. The values obtained were highest in the Speciality Area (3.32) and lowest in the Reliance on Others and Technology (2.14) subscales. The difference between the means of these two subscales was statistically significant, at t(244) = −23.589, p = .001. The values of the Reliance on Others and Technology, Ward Culture, Lack of Confidence and Lack of Influence on Patient Care subscales can be considered relatively low, as they were significantly lower than the midpoint of evaluation for all the subscales, which was 3, p < .05. In contrast, the values of the Lack of Time and Interruptions, Lack of Nursing Role Models and Speciality Area subscales were significantly higher than the midpoint of evaluation for all the subscales, p < .05.
Descriptive Statistics of the Barriers to Nurses’ Use of Physical Assessment Scale Subscales.

1 = strongly disagree that this is a barrier; 5 = strongly agree that this is a barrier.
The correlation coefficients between subscales were generically significant. The highest correlation occurred between the Lack of Nursing Role Models and Ward Culture subscales (r = .573, p ≤ .001) (Table 5).
Subscale Pearson's Correlations.

p < .05; ** p < .01; *** p < .001.
Associations Between Sample Characteristics and Perceived Barriers to Physical Assessment
Table 6 illustrates the relationships between participants’ sociodemographic and professional characteristics and the barriers to conducting physical assessments. Perceptions of these barriers did not vary significantly based on nurses’ sex, as indicated by a Wilks’ lambda = 0.978, F(7, 232) = .753, p = .627.
Associations Between Sample Characteristics and Perceived Barriers to Physical Assessment.

Abbreviations: M = mean; SD = standard deviation. *p ≤ .05; **p ≤ .01; ***p ≤ .001.
However, a significant variation was observed based on the nurses’ level of training, with a Wilks’ lambda = 0.927, F(7, 232) = 2.603, p = .013. Nurses holding a bachelor's degree reported significantly higher perceived barriers in the Lack of Time and Interruptions, Ward Culture and Lack of Nursing Role Models subscales.
Overall, the perceived barriers tended to decrease as nurses’ years of professional experience grew. This decline was statistically significant for the Lack of Confidence and Lack of Nursing Role Models subscales.
Discussion
This work provides information on the construct validity and internal consistency properties of the French-language version of the Barriers to Nurses’ Use of Physical Assessment Scale. The study's results broadly aligned with those of the original instrument developed by Douglas et al. (2014) and the Turkish validation (Turan et al., 2022), highlighting both commonalities and unique contextual factors.
The characteristics of the present study's participants, such as the sex ratio, mean age, professional experience and level of education, corroborate those in the original psychometric validation study by Douglas et al. However, our sample (N = 246) was smaller than Douglas et al.'s (N = 434), which could have negatively influenced the psychometric properties (Gunawan et al., 2021). Despite this difference, post hoc power analysis indicated that our sample provided sufficient power (>0.99) to detect medium effect sizes (Cohen's d ≈ 0.5 or r ≈ .3), thereby supporting the robustness of our analyses. Moreover, while the original scale and the Turkish validation by Turan et al. (2022) (N = 380 nurses) were developed and validated with acute care nurses from a single hospital, our study included nurses from nine institutions across two cantons, with 45.5% employed in rehabilitation settings.
A factor analysis was performed to test the French-language scale's construct validity. We used the KMO test and Bartlett's test of sphericity to assess the data's suitability for factor analysis. The KMO value was 0.848, considered good, and Bartlett's test showed a significant p-value (≤ .001), meaning that the correlation was suitable for analysis (Hair et al., 2013). Both the EFA and CFA confirmed that the seven-factor structure identified by Douglas et al. (2014) was replicable in the instrument's French-language version and explained a comparable proportion of variance. Factor loading, which reflects the strength of the relationship between an item and a factor, was used as the criterion for assigning items to factors. The initial factor analysis identified 10 factors (explaining 63.5% of the variance), but a seven-factor solution was adopted to align with Douglas et al. (2014). The total variance explained (54.6%) closely mirrored that reported in the original study (57.7%), supporting the instrument's robustness and cross-cultural applicability. These findings confirm our initial hypothesis that the French version would retain a multidimensional structure comparable to the original scale. The CFA provided evidence of acceptable model fit. The fit indices in our study (e.g., RMSEA = 0.054 and CFI = 0.86) were similar to those in the original version (RMSEA = 0.05 and CFI = 0.91). The Turkish validation also reported an acceptable model fit, although with comparatively weaker indices (RMSEA = 0.065 and CFI = 0.740), suggesting that the model is generally supported but exhibits slightly reduced fit in that sample.
At the total scale level, all three versions showed good to excellent reliability, with the French-language version yielding the highest Cronbach's alpha (α = .89), followed by the Turkish (α = .822) and the original version (α = .80).
Strong internal consistency was observed in the Lack of Time and Interruptions (α = .84) and Lack of Confidence (α = .88) subscales, consistent with Douglas et al. (2014) and the existing literature on time constraints and self-efficacy being major barriers to physical assessment skills (Turan et al., 2022). The Lack of Nursing Role Models subscale showed acceptable reliability (α = .70), highlighting the roles of leadership and mentorship in promoting physical assessment skills.
Contrary to our initial hypothesis that most subscales would show satisfactory reliability, the Speciality Area (α = .47) and Ward Culture (α = .29) subscales demonstrated low reliability, in contrast to their acceptable to excellent reliability in the original version (α = .70 and .84, respectively). Although the Turkish study did not report individual subscale alphas, it noted generally low item-total correlations, suggesting similar difficulties in these dimensions.
Our item-level analyses indicated that item 35 (Speciality Area) and item 4 (Ward Culture) contributed least to their respective subscales, with “Cronbach's Alpha if Item Deleted” suggesting theoretical increases to .664 and .699. Despite this, all items were retained to preserve construct validity, as supported by CR values exceeding 0.70 and acceptable AVE for Speciality Area. Speciality Area also satisfied discriminant validity criteria (AVE > MSV), whereas Ward Culture did not fully meet this criterion (AVE < MSV), suggesting some overlap with other constructs. Moreover, its items may not be sufficiently coherent to consistently capture cultural and environmental barriers within the workplace.
Although removing items such as item 35 and item 4 could improve internal consistency, doing so might compromise the conceptual breadth and content validity of the subscales. Given their theoretical relevance and acceptable CR, all items were retained, with future studies encouraged to assess item performance and consider refinement rather than elimination.
The low reliability observed in the Speciality Area (α = .47) and Ward Culture (α = .29) subscales raises questions about the influence of context and the relevance of certain items. One possible explanation lies in the contextual differences between the original study and the present work. Douglas et al. (2014) focused on nurses from a variety of acute care wards within a single hospital in Australia, whereas the present study examined nurses across multiple institutions in two different cantons of French-speaking Switzerland, with a broader range of specialized care settings, including surgery, geriatric services and different specialized rehabilitation care institutions. These differences in the healthcare context might have contributed to the differing perceptions in the Speciality Area and Ward Culture subscales, leading to lower internal consistency. The differences in nurses’ responsibilities across different specialities may also explain the variability observed. The original study focused on acute care settings (e.g., internal medicine, surgery, and cancer services), where nurses’ roles in physical assessment may be more clearly defined. In Switzerland, however, our study included acute and intermediate settings where the emphasis on physical assessment skills may differ, contributing to the differences observed in the Speciality Area and Ward Culture subscales.
Another potential explanation is the 11-year gap between the original study and the present one. Nursing programmes increasingly integrated clinical assessment skills into their curricula during this time, and expectations that nurses should perform these assessments have evolved. The growing emphasis on evidence-based practice and interdisciplinary collaboration in healthcare systems may have influenced nurses’ perceptions of their Ward Culture and Speciality Area. Lastly, our smaller sample size (N = 246) than the original study (N = 434) may also have contributed to the differences observed in the data and the lower internal consistency of certain subscales. Convergent validity was generally supported, as CR values exceeded the recommended threshold of 0.70 for all subscales, and AVE values were acceptable for Lack of Time and Interruptions (0.510) and Lack of Confidence (0.654). However, five subscales (Reliance on Others and Technology, Ward Culture, Lack of Nursing Role Models, Lack of Influence on Patient Care, and Speciality Area) showed AVE values below 0.50, suggesting that less than half of the variance in these constructs was explained by their items. Moreover, several subscales had MSV values exceeding their AVE, notably Ward Culture, Lack of Nursing Role Models, Lack of Influence on Patient Care, and Reliance on Others and Technology, indicative of limitations in discriminant validity. These results indicate conceptual overlap among some constructs, which may reflect the interrelated nature of organizational culture, professional support, and perceived influence on care in clinical practice. Direct comparison of convergent and discriminant validity across studies is limited, as neither the original nor the Turkish validation reported indicators such as AVE or MSV.
This potential overlap is further supported by inter-factor correlations, with both our study (r = .573) and the original study (r = .61) showing the strongest association between Lack of Nursing Role Models and Ward Culture. In contrast, the Turkish validation reported the highest correlation between Lack of Time and Interruptions and Ward Culture (r = .560), highlighting the influence of context-specific factors on the relationships between barriers.
Despite differences between the French-language version of the scale's psychometric properties and those of the original, the two sample's descriptive results were similar. The three subscales with the highest values and the three with the lowest values were the same in Douglas et al.'s study among nurses in Australia and the present study among nurses in French-speaking Switzerland. The Speciality Area subscale had the highest values in both studies, highlighting the significant influence of specialized clinical environments on nurses’ use of physical assessment skills. The Lack of Nursing Role Models subscale also scored high, which could be attributable to the relatively recent integration of physical assessment into Swiss nursing education programmes in 2012 and professional practice in 2015. Nurses may still be in the process of developing their expertise, which may explain the lack of experienced mentors or role models for younger nurses. Additionally, the significant heterogeneity in training programmes due to the diverse educational backgrounds of immigrant nurses (Immonen et al., 2019) may further contribute to this issue. The Lack of Time and Interruptions subscale ranked third, reflecting the impact of strained healthcare systems characterized by hospital overcrowding and shortages of nursing staff. In contrast, the Reliance on Others and Technology, Ward Culture and Lack of Influence on Patient Care subscales scored lower, indicating that these factors are perceived as less significant barriers. These findings show that nurses perceive technology as an essential component of care, improving the accuracy and efficiency of physical assessments. This aligns with previous studies (Douglas et al., 2014; Massey et al., 2017). Moreover, the particular healthcare settings covered in our study might foster more collaborative and supportive ward cultures that emphasize interdisciplinary teamwork. Such environments could lessen perceptions that ward culture is a limiting factor, as nurses feel empowered to use their physical assessment skills and participate proactively in patient care. The nurses in our study may also have more clearly defined roles and a degree of autonomy in clinical decision-making, which reduces feelings of reliance on others and technology and strengthens their sense of having an influence over patient care outcomes (Taylor et al., 2021). Regarding our hypothesis that perceived barriers to physical assessment may vary according to nurses’ sociodemographic and professional characteristics, our findings aligned with those of Douglas et al.'s original study. Specifically, both studies revealed that the perceived barriers tended to diminish as years of professional experience increased. This decline was statistically significant for the Lack of Confidence and Lack of Nursing Role Models subscales. Such findings are supported by existing evidence: in a systematic review on the teaching and practice of physical assessment skills, lack of confidence emerged as one of the most common barriers, consistently reported by both practicing nurses and final-year nursing students (Tan et al., 2021).
In contrast to the original study, however, we found significant correlations between levels of education and perceptions about barriers to physical assessment. Nurses holding a bachelor's degree perceived significantly higher barriers in the Lack of Time and Interruptions, Ward Culture and Lack of Nursing Role Models subscales. These results may be attributed to differences in years of experience. Nurses with a bachelor's degree are typically younger, as the requirement for a bachelor's degree-level nursing education was only introduced in Switzerland in the early 2000s. They may consequently have less clinical experience, which could explain their perceptions of greater barriers (Tan et al., 2021). Paradoxically, nurses with a bachelor's degree in Switzerland have received more extensive training in physical assessment. It was expected, therefore, that they would perceive fewer barriers to its use. This unexpected finding underscores how the influence of limited professional experience may shape perceptions about obstacles to better clinical practices, despite the advantages of an advanced nursing education (Tan et al., 2021). These findings may also reflect the growing concern in Switzerland regarding the teaching of physical assessment at the bachelor's degree level, where practical training opportunities in clinical settings remain limited. Such educational specificities may restrict the generalizability of our findings to other countries.
Strengths and Limitations
This methodological study revealed that the French-language version of the Barriers to Nurses’ Use of Physical Assessment Scale was broadly psychometrically reliable and valid. The findings are particularly relevant as the adapted scale is already widely used in clinical settings across French-speaking Switzerland. By evaluating its construct validity and internal consistency, the study provides added value for clinical practice, offering evidence to support the use of a psychometrically robust instrument for assessing barriers to nurses’ use of physical assessment and to guide the implementation of strategies that enhance their clinical practice.
Furthermore, our French-language instrument was grounded in the robust theoretical framework developed by Douglas et al. (2014), which had demonstrated solid validity and reliability in previous testing.
The study incorporated a sufficiently large sample of RNs from Switzerland's French-speaking regions, although it was smaller than Douglas et al.'s (2014) original sample. The demographic distribution of our participants reflected the reality of the nursing profession in Switzerland today, with more women and a well-balanced representation in terms of age and years of professional experience (Merçay et al., 2021). A primary limitation is that the processes of translation, back-translation, and cultural adaptation are not presented in the present article, as they were completed in previous studies (Epiney-Perruchoud, 2019; Gomes Fernandes, 2019). Consequently, this study focuses specifically on the assessment of construct validity and internal consistency. Moreover, the Content Validity Index (CVI) was not assessed, as this evaluation requires primary data collection and was not feasible with the available secondary data. This step had also not been performed in previous studies. Nevertheless, the widespread clinical use of the adapted scale supports its perceived content relevance among healthcare professionals.
A further limitation concerns the Speciality Area and Ward Culture subscales, which showed low internal consistency despite an acceptable factor analysis. Further studies with larger, more diverse populations could enhance the instrument's psychometric properties.
Generalizing these findings to all the hospitals in French-speaking Switzerland should be done cautiously, and direct comparisons with the original study should be interpreted with care due to differences between European and Australian healthcare systems. Although the original Barriers to Nurses’ Use of Physical Assessment Scale was validated in acute care settings, 45.5% of our participants were from rehabilitation settings. While the sample included a substantial proportion of nurses working in acute care, the presence of nearly half from rehabilitation contexts may influence the generalizability of the findings. This is particularly relevant given that the Speciality Area (α = .47) and Ward Culture (α = .29) subscales showed poor internal consistency, and several subscales exhibited suboptimal convergent and discriminant validity (e.g., AVE < 0.50 and MSV > AVE). These findings suggest that certain items may not fully capture the intended constructs in the French-speaking context or may be affected by cross-loadings and contextual differences between clinical settings. Since participation was voluntary, there is a potential selection bias, as nurses who were particularly concerned about the barriers to performing physical assessments may have been more inclined to respond. Moreover, the self-reported nature of the data may introduce response bias, affecting the reliability of certain findings. Finally, the floor effect observed in the Barriers to Nurses’ Use of Physical Assessment Scale may also have influenced our statistical results.
Implications for Practice
The validated French-language version of the Barriers to Nurses’ Use of Physical Assessment Scale provides researchers and practitioners with a reliable tool for assessing the challenges faced by nurses who wish to use their physical assessment skills in French-speaking healthcare settings. By identifying specific obstacles, this instrument could be used to support the development of targeted interventions aimed at enhancing nurses’ confidence, fostering more role models and improving occupational environments so that they facilitate the systematic use of physical assessment skills. From a clinical perspective, addressing these barriers is crucial to improving the early detection of patient deterioration, enhancing patient safety and optimizing the quality of nursing care. These findings may have implications for nursing education. By identifying perceived barriers to physical assessment, educators can target specific areas in the curriculum and clinical training to strengthen nurses’ skills, confidence, and routine use of systematic physical assessments. Although the instrument demonstrates satisfactory structural validity and internal consistency across several subscales, its clinical application should be tailored to the specific characteristics of each practice environment and supplemented with context-specific feedback to maximize its utility in enhancing nursing practice.
Refinement of the Speciality Area and Ward Culture subscales is needed to more accurately capture how these factors influence nurses’ use of physical assessment skills. The initial step should involve reviewing existing items to identify those with low factor loadings, high cross-loadings, or weak item-total correlations, which may compromise internal consistency or construct validity. Identified items could then be revised, reworded, or removed, with subsequent factor analysis to confirm the stability of the seven-factor structure. Following item reduction, additional items could be introduced to better represent each construct, improve reliability, and reflect the diverse roles and responsibilities of nurses across different healthcare contexts. Pilot testing should ensure consistent interpretation of items. Future research should adopt this iterative approach—combining item revision, item-reduction strategies, and selective item addition—to enhance the psychometric properties and validity of the scale in French-speaking healthcare environments.
Future research should also expand sample sizes and assess the scale's applicability across a broader range of clinical environments, including primary care. Recruiting larger, more diverse samples from various clinical settings and geographical regions will also help determine how nurses’ perceptions evolve with increased professional experience and the ongoing integration of physical assessment training in Swiss nursing education.
Qualitative studies exploring nurses’ experiences of and perspectives on physical assessment would complement these findings by offering a more nuanced understanding of the contextual and cultural factors influencing their practice. Furthermore, experimental research could provide deeper insights into the effectiveness of specific strategies aimed at reducing barriers and promoting physical assessment skills among nurses. By implementing controlled interventions, such studies could evaluate the impact of targeted training programmes, mentorship initiatives and organizational modifications on nurses’ clinical practices.
Conclusion
This study evaluated the construct validity and internal consistency of the French-language version of the Barriers to Nurses’ Use of Physical Assessment Scale. The instrument's psychometric evaluation showed it to be a reliable and valid means of assessing how nurses perceived barriers to them using physical assessment in French-speaking Switzerland. The findings emphasized that although perceived barriers such as time constraints and a lack of role models remained prevalent, variations in reliability across subscales suggested that further refinements may be necessary to address certain psychometric limitations and enhance the instrument's applicability in other clinical settings.
After using this instrument, healthcare institutions will be able to implement targeted interventions to improve nurses’ physical assessment skills, ultimately contributing to better patient outcomes. Further research is recommended to confirm these findings with larger samples and to explore strategies for overcoming identified barriers in clinical practice.
Supplemental Material
sj-docx-1-son-10.1177_23779608261431639 - Supplemental material for Cultural Adaptation and Psychometric Validation of the French-Language “Barriers to Nurses’ Use of Physical Assessment Scale”
Supplemental material, sj-docx-1-son-10.1177_23779608261431639 for Cultural Adaptation and Psychometric Validation of the French-Language “Barriers to Nurses’ Use of Physical Assessment Scale” by Filipa Pereira, Lorena Da Veiga Gonçalves, Ricardo Salgado, Catherine Bolduc and Henk Verloo in SAGE Open Nursing
Footnotes
Acknowledgments
The authors would like to acknowledge Sara Gomes Fernandes and Maude Epiney-Perruchoud for their invaluable contribution in providing the data used for this study. The statistics were checked by an expert statistician prior to submission: Boris Wernli: boris.wernli@unil.ch.
Ethical Considerations
This work used data from original studies approved by a Swiss university hospital's Research Application Review Board (No. 2020-12).
Consent to Participate
Data for this work came from three prior studies. By returning the completed questionnaire to investigators, respondents provided their tacit consent to participate in the studies and agreed to their participation conditions. Participants were informed of their rights, including the right to withdraw from the study at any time without any consequences.
Author Contributions
FP, LVG, and HV: Made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data. FP, LVG, RS, CB, and HV: Involved in drafting the manuscript or revising it critically for important intellectual content. FP, LVG, RS, CB, and HV: Given final approval of the version to be published. Each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content. FP and HV: Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the study's findings are available from the corresponding author upon reasonable request.
Permission to Reproduce Material From Other Sources
The data used in this work were obtained from previously conducted research studies, and permission for their use was secured from their respective authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.