
Abstract
Introduction
Professional socialization is a critical process that influences hospital nurses’ professional identity, competence, and ethical standards, ultimately impacting the quality of patient care.
Objective
This study aimed to translate the Professional Socialization Scale (PSS) for Hospital Nurses into Persian and evaluate its psychometric properties among Iranian nurses.
Methods
A cross-sectional methodological study was conducted in two phases: translation and psychometric evaluation. A stratified sample of 511 nurses from both public and private hospitals in Kermanshah City, Iran, participated in the study. The scale was translated into Persian using the Douglas and Craig model, and its content and face validity were assessed. Construct validity was evaluated through exploratory factor analysis (EFA) and confirmatory factor analysis (CFA). The internal consistency of the scale was assessed using Cronbach's alpha and McDonald's omega coefficients, while test–retest reliability was evaluated using the intraclass correlation coefficient (ICC).
Results
The PSS scale maintained the meaning of the original English version and was clear and understandable for hospital nurses. In qualitative face validity, one item changed slightly and all items were retained in the quantitative face validity assessment. Each item's content validity ratio ranges from 0.71 to 1, the Item content validity index ranges from 0.79 to 1, while the Scale-level Content Validity Index was 0.89. The EFA and CFA confirmed a four-factor structure of the Persian version of the scale, with 21 items explaining 67.72% of the total variance. The model fit indices indicated excellent model fit. The scale demonstrated acceptable internal consistency (Cronbach's alpha = 0.908, McDonald's omega = 0.904) and test–retest reliability (ICC = 0.908).
Conclusion
The Persian version of the PSS for Hospital Nurses is a valid and reliable instrument. Nursing managers should facilitate the professional socialization process for nurses. This scale can be used to assess the socialization of nurses and guide their career development.
Introduction
Nurses, as integral pillars of healthcare systems, play an indispensable role in promoting and maintaining public health (Flaubert et al., 2021). Their role continues to expand across diverse care settings (Weber et al., 2022). Contemporary advancements in science and technology (Isidori et al., 2022), coupled with demographic shifts and increasing care complexity, have elevated the significance of nursing. Among the factors shaping professional identity, professional socialization is paramount in enhancing the quality of care delivery, patient satisfaction, and cost-effectiveness within modern healthcare systems (Moradi et al., 2017).
Professional socialization is a process of internalizing and developing a professional identity through the acquisition of knowledge, skills, attitudes, beliefs, values, norms, and ethical standards, enabling individuals to fulfill their professional roles (Shahr et al., 2019). In nursing, professional socialization is indispensable, transforming novice nurses into competent practitioners (Darban & Safarzai, 2020; Salisu et al., 2019). This process not only elevates the nursing profession from a traditional to a scientific discipline but also enhances nurses’ motivation and job satisfaction (Seyed et al., 2020). Consequently, professional socialization can serve as a valuable indicator of a nurse's preparedness and capability to assume their professional responsibilities (Moon & Chang, 2023; Rakkarn et al., 2023).
Effective professional socialization necessitates a comprehensive approach, including structured educational programs, exemplary role models, supportive clinical environments, practical experiences, and constructive feedback (Seyed et al., 2020). Professional nurses play a pivotal role in this process, acting as role models and creating conducive learning environments for learners and novice nurses (Mafumo et al., 2022). A qualitative study by Zarshenas et al. highlighted the significance of a sense of belonging and professional identity in the socialization of nurses in Iran (Zarshenas et al., 2014). To optimize patient care and satisfaction, nursing managers must identify and address barriers to professional socialization (Darban & Safarzai, 2020). Developing standardized tools to assess professional socialization from multiple perspectives is crucial for a comprehensive understanding of this complex process.
Review of Literature
Extensive literature reviews have revealed a dearth of instruments designed to assess professional socialization specifically among practicing nurses. Existing tools primarily target nursing students, such as the instrument developed by Du Toit (1995), which evaluates the level of professional socialization among nursing students. This study, conducted at two universities in Australia, demonstrated that nursing students at these universities exhibit a high level of professional socialization. Additionally, Brown et al. (2013) introduced a 7-dimensional framework to assess the role of clinical teachers in facilitating nursing students’ professional socialization. Their findings emphasize the critical role of clinical teachers in this process. Kim & Shin (2020), drawing on Meleis et al.'s transition theory (Meleis et al., 2000), proposed a theoretical framework highlighting the significance of clinical adaptation in fostering professional socialization among nursing students. This adaptation is achieved through enhancing the clinical learning environment and promoting the development of clinical practice competencies.
Despite these advancements, a comprehensive instrument tailored to assess professional socialization among hospital nurses remains elusive. To address this gap, Moon & Chang (2023) developed the Professional Socialization Scale (PSS) for hospital nurses in South Korea. The PSS comprises 21 items across four factors: Ethical Practice and Reflection, Perception of Respect and Recognition, Clinical Competency Based on Leadership, and Desires and Motivation for Professional Development. By capturing diverse facets of professional socialization, the PSS can serve as a valuable tool for assessing and promoting the professional development of hospital nurses (Moon & Chang, 2023).
While the concept of professional socialization among nurses has garnered increasing attention in Iran in recent years, empirical research in this area remains limited. For instance, a study conducted by Tahmasbi et al. (2017) on 600 Iranian nurses revealed a high level of professional socialization. While the researcher-developed questionnaire used in the study by Tahmasbi et al. was applied within the Iranian context, its development and psychometric properties were not fully articulated. This omission necessitates a cautious interpretation of the findings, as the instrument's validity and reliability remain somewhat unclear (Tahmasbi et al., 2017). In contrast, the Korean PSS (Moon & Chang, 2023) offers a more contemporary and multifaceted perspective on professional socialization compared to previously developed tools in this domain.
The PSS's four-factor structure, encompassing leadership and motivation, aligns with the evolving role of nurses in modern healthcare, including the Iranian system. These factors capture critical dimensions of nursing practice that resonates with the challenges and opportunities faced by nurses today. Furthermore, the PSS demonstrates significant relationships with nurses’ professional values, professionalism, satisfaction, quality of life, stress, and burden. This suggests its potential to identify specific areas for intervention and improvement.
Given the pressing concerns surrounding nurse retention and job satisfaction in Iran, a robust and contextually relevant tool for assessing professional socialization is crucial. The PSS, with its comprehensive design and demonstrated psychometric rigor, holds promise for accurately gauging this construct. By providing insights into nurses’ professional development, it can inform targeted educational programs, particularly those emphasizing leadership and ethical practice. Ultimately, this enhanced understanding can contribute to improved patient care quality by fostering a stronger sense of professional identity among Iranian nurses.
Therefore, the development of a Persian version of the Korean PSS for Iranian hospital nurses is warranted. This adaptation aims to address the limitations of previous instruments by offering a modern, reliable, and culturally sensitive measure of professional socialization. Such an adaptation not only supports the professional growth of Iranian nurses but also contributes to the broader advancement of nursing practice, education, and research, both within Iran and globally. Consequently, this study focuses on the translation, cultural adaptation, and psychometric validation of the PSS for use among Iranian hospital nurses, ensuring its appropriateness and soundness within this specific context.
Method
Study Design
This cross-sectional methodological study, conducted between March and September 2024, aimed to evaluate the psychometric properties of the Persian version of the PSS among hospital nurses. The study involved a two-stage process. The first stage was the translation of the PSS into Persian. The second stage involved a cross-sectional survey to assess the reliability and validity of the Persian PSS.
Setting and Participants
This research involved 511 nursing professionals, including staff nurses and chief nurses working in both public and private hospitals within Kermanshah City, located in western Iran. Participants were selected stratified sampling based on predefined inclusion criteria. To carry out the sampling, first, according to the sample size and the number of nurses working in each of the hospitals of Kermanshah City, the quota of each hospital was determined, and based on that, random sampling was done from clinical nurses working in the departments in different shifts.
To ascertain an appropriate sample size, a power analysis was conducted. A widely accepted guideline for factor analysis posits a minimum of 5–10 participants per questionnaire item (Bujang et al., 2012; Kyriazos, 2018). Additionally, sample sizes of 50, 100, 200, 300, 500, and 1000 are considered very poor, poor, fair, good, very good, and excellent, respectively (Comrey & Lee, 2013). For Exploratory Factor Analysis (EFA), a sample size ranging from approximately 100–250 participants is recommended. It is generally recommended to have a sample size of more than 200 participants for the Confirmatory Factor Analysis (CFA) stage (Marsh et al., 1988; Steenkamp & Maydeu-Olivares, 2023).
Given that the PSS comprises 21 items, a minimum sample size of 105–210 participants is suggested. To bolster the robustness of the analysis, it is advisable to surpass this minimum threshold. Consequently, 511 nurses were randomly assigned to two subsamples: 200 for EFA and 311 for CFA. This sample size is deemed adequate for a scale with robust psychometric properties.
Participants were included based on their expressed interest, satisfaction, and more than 12 months of work experience. Questionnaires with over 10% missing data were excluded (Nulty, 2008). Of the 610 surveys distributed, 545 were returned. After excluding 34 incomplete surveys, the final sample size for analysis comprised 511 nurses.
The Translation Process
Measurement Instrument
The PSS, developed by Moon and Chang in 2023, is a 21-item instrument assessing four dimensions of professional socialization: ethical practice and reflection, perception of respect and recognition, clinical competency based on leadership, and desires and motivation for professional development. Respondents rate each item on a 6-point Likert scale (1 = strongly disagree to 6 = strongly agree). Higher scores indicate a greater perceived level of professional socialization. The PSS has demonstrated strong reliability, with a Cronbach's alpha of 0.95 and a test–retest reliability intraclass correlation coefficient (ICC) of 0.90 (Moon & Chang, 2023).
Prior to the translation process, permission to use the PSS was obtained from the original authors. The translation and cultural adaptation of the PSS from its original language to Persian were conducted collaboratively and iteratively, adhering to the methodological guidelines outlined by Douglas and Craig (Douglas & Craig, 2007).
The translation process involved several stages: (1) Pretranslation (establishing equivalence), (2) Initial translation, (3) Pretesting, (4) Review, and (5) Administration. The Persian version was subsequently submitted to the original scale developer for final approval before its administration.
A multidisciplinary team of 10 experts, including a psychologist, five nursing PhDs, and four experienced staff nurses, was assembled to establish conceptual equivalence during the pretranslation stage. The team focused on ensuring category, functional, and construct equivalence across cultures. Category equivalence refers to the similarity of categories used to describe phenomena, while functional equivalence assesses the instrument's cross-cultural functioning. Construct equivalence ensures the underlying meaning or concept is consistently understood across different cultural groups. Through collaborative discussions, the team made minor linguistic adjustments to specific subscale items. Following the establishment of item equivalence, two experienced translators independently translated the questionnaire into Persian. Subsequently, an expert panel reviewed the translations to ensure accurate and culturally appropriate rendering of each item's meaning. A separate group of researchers, who were not involved in the initial translation, conducted a pretest to assess the clarity, relevance, and cultural appropriateness of the translated items within the Iranian healthcare context. A final review meeting was convened, bringing together translators, the expert panel, and the authors to finalize the Persian version of the PSS. The goal was to ensure that each item accurately conveyed its intended meaning. Following the review, a pilot test was conducted with 15 nurse volunteers who were not part of the study sample (face validity). This pilot test aimed to assess the clarity and comprehensibility of the final Persian version of the PSS.
Personal Information Form
The personal information form used in this study was designed to collect the demographic and clinical characteristics of the participating nurses. This form included questions regarding age, gender, clinical experience, educational background, Ward, Work Shift, and marital status. The data collected through this form provided essential context for analyzing the psychometric properties of the PSS and understanding the sample characteristics.
The Psychometric Evaluation Phase
The psychometric evaluation phase focused on assessing the validity (face, content, and construct) and reliability (internal consistency and stability) of the Persian version of the PSS.
Face Validity Assessment
A qualitative approach was employed to assess the instrument's understandability, clarity, and relevance. A panel of 15 nurses with varying levels of clinical experience (four with less than 2 years, four with 2–6 years, four with 6–10 years, and three with over 10 years) evaluated the items (Taghizadeh et al., 2017). Additionally, a quantitative approach was used to assess item importance. Each panel member rated the importance of each item on a 5-point Likert scale. Items with an impact score exceeding 1.5 were retained for further analysis (Mohammadbeigi et al., 2015).
Content Validity Assessment
Both qualitative and quantitative methods were employed to assess content validity. For qualitative content validity, a panel of 13 experts, including nursing faculty, nursing managers, and experienced clinical nurses, evaluated the scale's items for grammatical accuracy, word choice, item placement, clarity, scoring, and cultural relevance to Iran. The Content Validity Ratio (CVR) and Content Validity Index (CVI) were used to quantitatively assess the scale's content validity.
The same 13 experts were invited to evaluate the necessity of the instrument's items using a 3-point Likert scale labeled “Essential,” “Useful but not essential,” and “Unessential” for the calculation of the CVR. They were also asked to comment on item wording, and the items were revised based on their feedback. Their rating scores were used to calculate CVR using Lawshe's method (Lawshe, 1975). With 13 experts, the minimum acceptable CVR value was set at 0.54.
The CVI was used to evaluate the relevance of the PSS items at both the individual item level (Item CVI [I-CVI]) and the overall scale level (Scale-level CVI [S-CVI]). To assess item relevance, 12 experts rated each item on a 4-point Likert scale (1 = not relevant to 4 = highly relevant). The accepted CVI value is 0.78 or higher for individual items and ideally 0.90 or higher for the overall scale (Polit et al., 2007).
Construct Validity Assessment
To assess the construct validity of the Persian version of the PSS, both EFA and CFA were employed. These are primary methods for examining construct validity (Mokkink et al., 2012). Considering translating the tool into Persian and using it in a different cultural context than the original version, as well as uncovering hidden variables based on Iranian society's culture, we first conducted an EFA followed by a CFA (Sharif-Nia & Hanifi, 2023).
Out of 511 total participants, due to the importance of separating the samples in each of the construct validation stages (Kyriazos, 2018; White, 2022) a subset of 200 was chosen for EFA, and the remaining 311 were used for CFA.
Before conducting factor analysis, the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy and Bartlett's test of sphericity were performed. A KMO value above 0.7 and a significant Bartlett's test (p < .05) indicate the suitability of the data for factor analysis (Henson & Roberts, 2006).
Exploratory factor analysis with Varimax rotation was employed to identify the factor structure of the scale. The total variance explained should exceed 40%, and eigenvalues should be greater than 1 (Boateng et al., 2018; Carpenter, 2018). Additionally, factor loadings should exceed 0.5 to ensure optimal construct representation (Jalali et al., 2024b; Wolf et al., 2013).
Confirmatory factor analysis is often used in cultural adaptation studies as it is well-suited for testing specific hypotheses about the instrument's structure (Polit, 2015). In this study, CFA with maximum likelihood estimation was performed. The following fit indices were used to assess the model's goodness of fit: χ2/df < 3, CFI > 0.9, TLI > 0.9, IFI > 0.9, and RMSEA < 0.1 (Hu & Bentler, 1999; Jalali et al., 2024a; RB, 2010).
Reliability Assessment
To assess reliability, the test–retest method was employed to evaluate stability. This method involves administering the instrument twice to the same sample group (Polit and Beck, 2010) with a time interval of at least 10–14 days (Terwee et al., 2007). The sample size of 50–100 participants is considered adequate for this test (PROMIS, 2016). The ICC was used to interpret the results, with values below 0.5 indicating poor reliability, 0.5–0.75 moderate, 0.75–0.9 good, and above 0.9 excellent (Koo & Li, 2016).
To assess internal consistency, Cronbach's alpha and McDonald's omega coefficients were calculated. Values greater than 0.70 for both coefficients indicate acceptable internal consistency (McNeish, 2018; Thorpe). Additionally, item-total correlations were examined to assess the suitability of each item. Correlation coefficients above 0.20 were considered acceptable (Kline, 1986).
Data Collection
After obtaining the necessary permissions from hospitals, the researcher employed stratified sampling to select participants who met the study's inclusion criteria. Following a clear explanation of the study's objectives and obtaining informed consent, questionnaires were distributed in sealed envelopes at nursing stations during various shifts. Participants completed the questionnaires independently at home or in designated rest areas to ensure self-reporting and minimize potential bias. Participation was voluntary, and 511 complete questionnaires were included in the analysis. All questionnaires were filled out on paper.
Data Analysis
SPSS version 27 and LISREL version 8 were used for data analysis. Descriptive statistics were employed to summarize demographic data. The Waltz and Bausell index was used to assess quantitative content validity (Polit et al., 2007). Exploratory and confirmatory factor analyses were conducted to evaluate construct validity. A p-value of less than .05 was considered statistically significant. Cronbach's alpha and test–retest reliability were used to assess the instrument's reliability. Internal consistency was evaluated using the Cronbach's alpha and McDonald's omega coefficient.
Ethical Considerations
This study received ethical approval from the Ethics Committee of Kermanshah University of Medical Sciences (Ethics code:
Results
Descriptive Results
A total of 200 nurses participated in the EFA phase, with a mean age of 32.65 years (SD = 6.58), ranging from 23 to 60 years. The sample comprised 39.5% males, 48.5% unmarried individuals, and 84.5% bachelor's degree holders (Table 1).
Demographic Characteristics of Participants in the Study.

For the CFA, 311 nurses were included. The mean age was 32.76 years (SD = 6.12), ranging from 23 to 60 years. The sample consisted of 42.8% males, 49.8% unmarried individuals, and 85.5% bachelor's degree holders (Table 1).
Face Validity Assessment
One item was revised based on qualitative feedback regarding understandability and clarity. Additionally, all items achieved an impact score greater than 1.5 in the quantitative assessment, indicating acceptable face validity for all 21 items of the PSS.
Content Validity Assessment
Qualitative content analysis identified the need for modifications in items 9, 11, and 16 (e.g., clarifying “leadership” and “professional respect” in Persian) to improve clarity and comprehensibility. Minor adjustments to items resolved ambiguities identified in pretesting, aligning the adapted version functionally with the original scale. After expert review and revisions, these items were deemed suitable. The quantitative content validity was assessed using the CVR, which yielded a value of 0.88, falling within the acceptable range of 0.71 to 1. Furthermore, all item CVI values exceeded 0.79, and the S-CVI was 0.89, indicating acceptable content validity for all 21 items of the scale.
Construct Validity
Exploratory Factor Analysis using Maximum Likelihood estimation with Varimax rotation was conducted (Table 2). The KMO measure of sampling adequacy was 0.908, and Bartlett's test of sphericity was significant (χ² = 2745.445, df = 210, p < .0001), indicating suitability for factor analysis. The EFA revealed a four-factor structure with eigenvalues greater than 1.0, explaining 67.72% of the total variance. All items had factor loadings above 0.50, supporting the adequacy of the factor structure. The scree plot further confirmed the four-factor structure of the PSS (Figure 1).
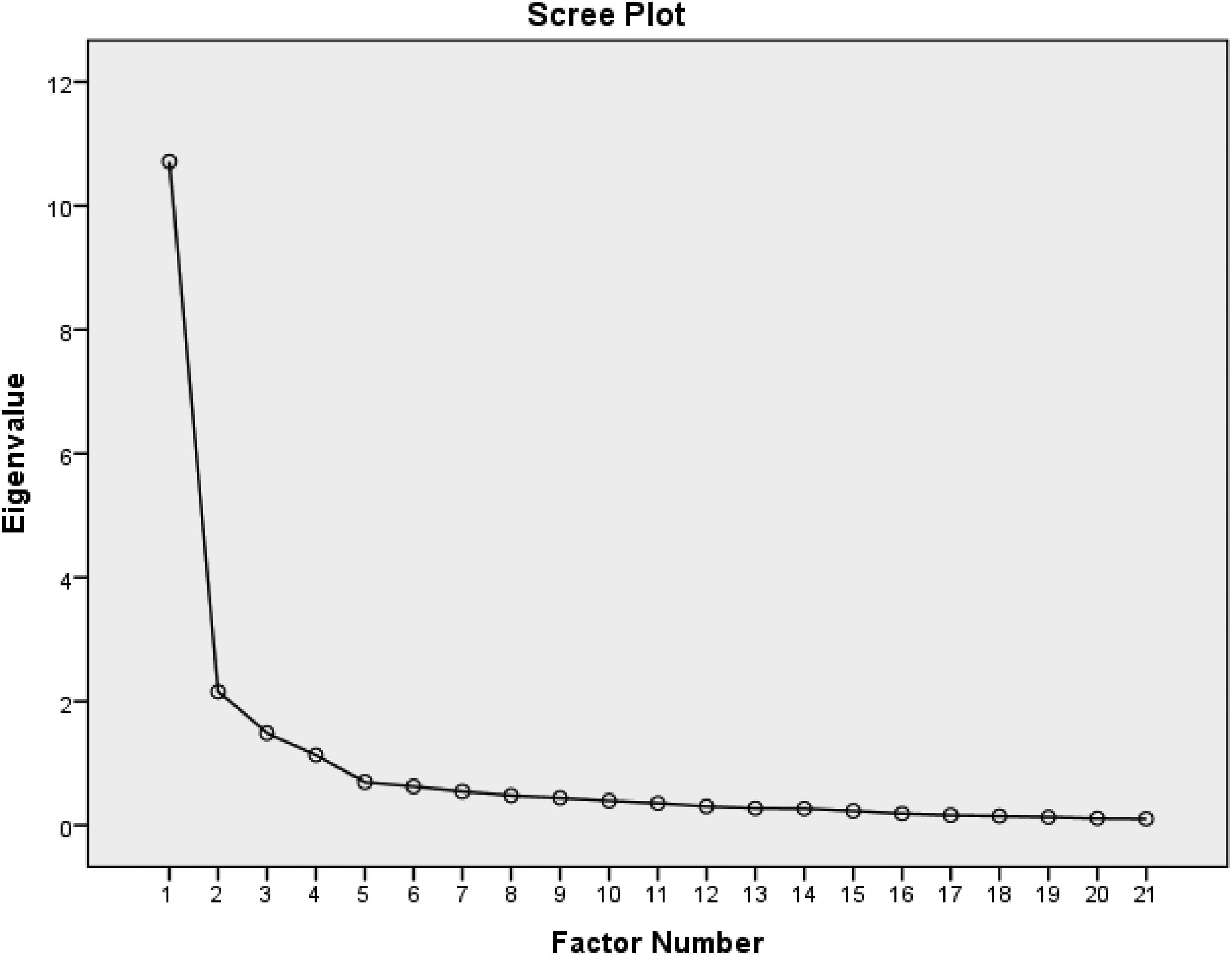
Scree plot of the extracted components of the Professional Socialization Scale.
Pattern Matrix of Exploratory Factor Analysis (Final Stage) (N = 200).
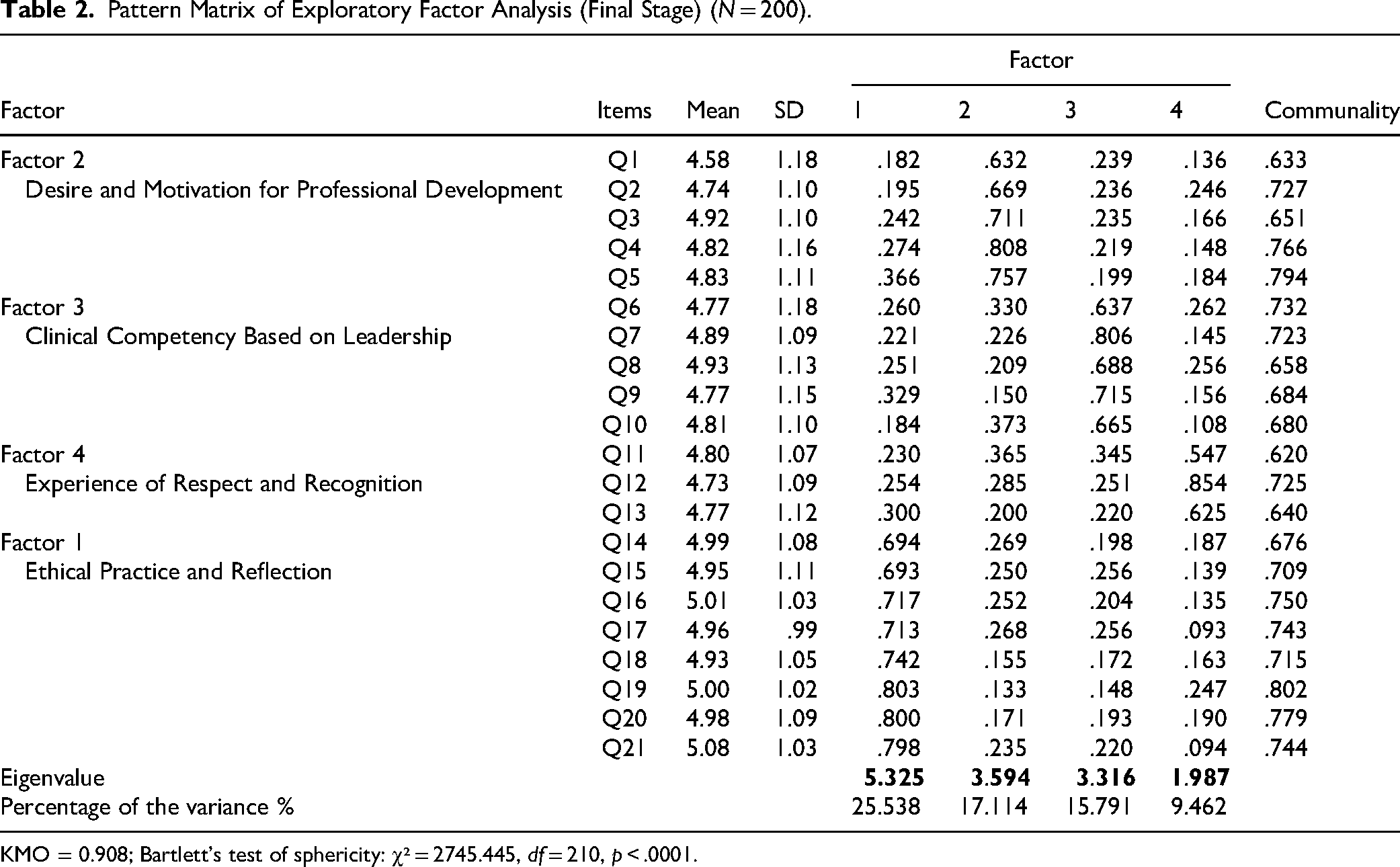
KMO = 0.908; Bartlett's test of sphericity: χ² = 2745.445, df = 210, p < .0001.
Confirmatory Factor Analysis confirmed the four-factor structure of the 21-item PSS. Fit indices, including χ²/df = 2.95, RMSEA = 0.079, NNFI/TLI = 0.91, CFI = 0.90, GFI = 0.91, and SRMR = 0.05, indicated a reasonable model fit. Figure 2 depicts the path diagram and factor loadings from the CFA. Pearson's correlation analysis revealed significant and positive relationships between the subscales and the overall scale, as shown in Table 3. All first- and second-order factor loadings were statistically significant at the 95% confidence level (|λ| > 1.96). Table 4 presents the Lambda coefficient, indicating the strength of factor loadings associated with a given factor.

Final measurement model of the Professional Socialization Scale from confirmatory factor analysis (N = 311).
The Correlation of the Professional Socialization Scale and Subscales (N = 311).

* Professional Socialization Scale; **p < .01.
T-Value, Pearson Correlation Coefficient, Factor Loadings, Macdonald's ω, and Cronbach's Alpha of the Professional Socialization Scale and Subscales (N = 311).

**p < .01; ***p < .001.
The calculated values for all factor loadings of the first and second orders are greater than 1.96 and are therefore significant at the 95% confidence level.
The specific value, denoted by the Lambda coefficient (λ), is calculated from the sum of the factor loadings related to all the variables of that factor.
Pearson correlation coefficient.
Reliability Tests
Internal Consistency
The Cronbach's alpha coefficient for the overall scale was 0.908, indicating excellent internal consistency. For the individual factors, Cronbach's alpha ranged from 0.696 to 0.852, demonstrating acceptable reliability for all factors (Table 4). Similarly, McDonald's omega coefficient for the total scale was 0.904, and for the four factors ranged from 0.697 to 0.850, further supporting the scale's reliability. These findings collectively demonstrate the scale's strong internal consistency. Additionally, item-total correlation coefficients ranged from 0.588 to 0.742 (Supplementary Table 1).
Test–Retest Reliability
The ICC for the total scale score was 0.908 (95% CI: 0.892–0.922), indicating high test–retest reliability (Table 4).
Discussion
The present study aimed to culturally adapt and validate the PSS developed by Moon and Chang in 2023 (Moon & Chang, 2023) for use in the Iranian context. The adapted PSS comprised four subscales: Ethical Practice and Reflection (eight items), Desire and Motivation for Professional Development (five items), Clinical Competency Based on Leadership (five items), and Experience of Respect and Recognition (three items). The rigorous translation process, including pretranslation equivalence checks and iterative reviews by a multidisciplinary team, ensured linguistic and cultural alignment. These steps contributed to the high face validity scores (impact score >1.5 for all items), reflecting the clarity and relevance of the adapted items. Content validity was assessed using the CVR and S-CVI. The CVR and S-CVI values for the adapted PSS were 0.88 and 0.89, respectively. These findings, combined with the original study's I-CVI of 0.78 and S-CVI of 0.91, provide strong evidence for the content validity of the PSS in both the original and adapted versions. The PSS demonstrates its ability to accurately measure professional socialization among nurses.
In this study, the four-factor model explained 67.72% of the total variance, indicating a strong model fit. These findings are comparable to those of Moon & Chang (2023), who reported a 67.12% explained variance for their original PSS. The similarity in explained variance across both cultures suggests that the PSS effectively measures the construct of professional socialization in both Iranian and South Korean nursing contexts.
The “Ethical Practice and Reflection” (EP) component emerged as the most influential factor, accounting for 25.53% of the total variance explained. This finding aligns with Moon and Chang's study (Moon & Chang, 2023), where the EP component also contributed the highest percentage (50.03%) to the overall variance. The prominence of the EP component underscores the critical role of ethical considerations in professional socialization among nurses. The eight items within the EP component emphasize: respecting patient dignity and empathy, adopting ethical behaviors and attitudes in nursing roles, making evidence-based judgments, creating a safe environment for nursing practices, supporting colleagues and sharing knowledge and skills, and reflecting on nursing activities. These items are directly relevant to the daily practice of clinical nurses. Adherence to ethical principles is fundamental to nursing care, reflecting respect for patient dignity (Casey et al., 2019; Soltaninejad et al., 2023). Ethical behavior among nurses has been linked to improved clinical service quality and patient satisfaction (Feizi et al., 2024). Effective teamwork and communication are essential for nurses to fulfill their professional responsibilities and deliver quality care (Mahmood et al., 2021). Reflection, teamwork, and information sharing facilitate professional socialization, encouraging nurses to engage with their work environment and participate in interpersonal communication (Molavynejad et al., 2024; Moradi et al., 2017; Salisu et al., 2019).
The “Desire and Motivation for Professional Development” (DM) component accounted for 17.11% of the total variance, ranking second in importance for assessing professional socialization among nurses. This component comprises five items that focus on the willingness to acquire new knowledge and skills, and the motivation to apply these in clinical practice. Lifelong learning and the acquisition of new roles are essential aspects of professional socialization (Dinmohammadi et al., 2013; Ghaderpanah et al., 2024). Intrinsic motivation and passion are crucial drivers of lifelong learning and the adoption of new roles, facilitating the successful navigation of challenges and the socialization process (Salisu et al., 2019).
The “Clinical Competency Based on Leadership” (CL) component contributed 15.79% to the total variance explained. This component assessed nurses’ sensitivity to patient needs, adherence to professional standards, creativity in care planning and implementation, and active participation in workplace improvement. Clinical competence in nursing is underpinned not only by technical skills but also by leadership abilities (Mrayyan et al., 2023). Leadership qualities such as anticipating patient needs, creativity, innovation, and a focus on human needs can significantly impact patient outcomes (Scully, 2015). Clinical leader nurses play a crucial role in the successful implementation of care programs, driving positive changes and improvements in care practices (Swinton & Haverkamp, 2023). The CL component is integral to professional socialization, and its enhancement contributes to improved quality of care.
The “Experience of Respect and Recognition” (RR) component, accounting for 9.46% of the total variance, assessed the extent to which nurses feel valued and respected as professionals. This component underscores the importance of social respect and recognition in shaping a nurse's professional identity. Nurses, given their critical role in patient care, require social acceptance and respect. Positive feedback and recognition from patients and the public enhance nurses’ motivation, job satisfaction, and sense of professional belonging (Amaniyan, Nobahar & Raiesdana, 2021; Drennan & Ross, 2019; Jalalodini & Heidary, 2024; 27(90)). Conversely, a lack of respect and recognition can contribute to nurse burnout and turnover. Social respect for nurses strengthens their professional identity and plays a crucial role in professional socialization, contributing to nurse retention and improved quality of care (Amaniyan et al., 2021).
Confirmatory factor analysis was conducted to validate the hypothesized four-factor structure. The results of the CFA supported the proposed model, with each item loading onto its respective factor. Goodness-of-fit indices indicated an adequate fit for the model. The results of the CFA are consistent with those reported by Moon and Chang (χ² = 460.33, χ²/df = 2.52, TLI = 0.94, CFI = 0.95, SRMR = 0.04, RMSEA = 0.06) (Moon & Chang, 2023), suggesting a good fit between the items and the latent factors (Ebadi et al., 2017).
The internal consistency reliability of the scale was assessed using Cronbach's alpha, ICC, and McDonald's omega. The obtained values of 0.908, 0.908 (CI: .892–.92), and 0.904, respectively, indicate acceptable levels of internal consistency. These findings are consistent with those reported by Moon & Chang (2023), who reported Cronbach's alpha and ICC values ranging from 0.84 to 0.90 and 0.77 to 0.81, respectively, for each factor. The high reliability coefficients suggest that the Persian version of the PSS is a reliable instrument for measuring professional socialization among nurses.
The PSS is a self-report instrument designed to assess the process of professional socialization among clinical nurses. It captures both individual perceptions of professional socialization values and norms and aspects related to interactions with colleagues and daily clinical practice.
Limitations
This study employed a cross-sectional design of nurses from a single university in western Iran to investigate the psychometric properties of the Persian version of the PSS. The measurement model was derived from the data, limiting the generalizability of the findings. While the content and structural validity of the PSS were assessed, criterion-related validity, including concurrent and predictive validity, was not examined. Future research should explore the applicability of the PSS across diverse cultural contexts and countries to further validate and adapt the instrument for measuring professional socialization among a broader range of nurses.
Implications for Practice
By utilizing this scale, nursing managers can support continuous professional development programs, thereby acknowledging and valuing nurses’ roles. This strategy can help alleviate issues such as secondary traumatic stress and burnout by fostering a supportive work environment that prioritizes ongoing education and ethical practices.
Conclusion
This study successfully validated the PSS as a reliable and valid instrument for assessing professional socialization among Iranian nurses. The PSS provides a comprehensive measure of key dimensions of professional socialization, including ethical practice, motivation for professional development, clinical leadership, and respect and recognition. The findings of this study have significant implications for nursing education, practice, and research. The PSS can be used to identify areas for improvement in nursing education and training programs. Furthermore, it can be employed to assess the effectiveness of interventions aimed at enhancing professional socialization. By understanding the factors that contribute to professional socialization, healthcare organizations can implement strategies to support nurses’ professional development and improve patient care.
Supplemental Material
sj-docx-1-son-10.1177_23779608251345276 - Supplemental material for Psychometric Evaluation of the Persian Version of the Professional Socialization Scale for Hospital Nurses: A Methodological Study
Supplemental material, sj-docx-1-son-10.1177_23779608251345276 for Psychometric Evaluation of the Persian Version of the Professional Socialization Scale for Hospital Nurses: A Methodological Study by Amir Jalali, Azam Sharifi, Ali Akbar Vaisi Raygani, Faezeh Ghesmati, Amirhossein Naghibzadeh, Nazanin Mardani Taghvostani and Khalil Moradi in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251345276 - Supplemental material for Psychometric Evaluation of the Persian Version of the Professional Socialization Scale for Hospital Nurses: A Methodological Study
Supplemental material, sj-docx-2-son-10.1177_23779608251345276 for Psychometric Evaluation of the Persian Version of the Professional Socialization Scale for Hospital Nurses: A Methodological Study by Amir Jalali, Azam Sharifi, Ali Akbar Vaisi Raygani, Faezeh Ghesmati, Amirhossein Naghibzadeh, Nazanin Mardani Taghvostani and Khalil Moradi in SAGE Open Nursing
Footnotes
Acknowledgements
The authors thank the faculty members of the Student Research Committee of Kermanshah University of Medical Sciences. This research project has been registered with code 4020237 at Kermanshah University of Medical Sciences, Iran.
Consent for Publication
All participants were informed about the study process and its objectives, and written informed consent was obtained from them.
Authors’ Contributions
All authors participated and approved the study design. Khalil Moradi, Azam Sharifi, Ali Akbar Vaisi Raygani, and Amir Jalali contributed to designing the study. Faezeh Ghesmati, Amirhossein Naghibzadeh, and Nazanin Mardani Taghvostani collected the data, and data analyses were done by Amir Jalali and Khalil Moradi. The final report and article were written by Khalil Moradi, Azam Sharifi, Ali Akbar Vaisi Raygani, Amir Jalali, Faezeh Ghesmati, Amirhossein Naghibzadeh, and Nazanin Mardani Taghvostani, and all authors read and approved the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets used in the study are available from the corresponding author on reasonable request.
Data Availability
The datasets used for the present analysis may be made available upon reasonable request by contacting the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.