
Abstract
Background
Diabetes health literacy (DHL) and self-care behavior play an important role in avoiding and controlling complications of diabetes mellitus and are positively associated with good glycemic control and quality of life improvement. However, we lack evidence describing their magnitude in the East Arsi zone of the Oromia regional state of Ethiopia.
Objectives
This study was aimed to assess the magnitude of DHL, self-care behavior, and associated factors among adult diabetes patients attending follow-up care at selected public hospitals in the East Arsi zone, Oromia, Ethiopia, 2025.
Methods
An institutional based cross-sectional study was employed in five public hospitals found in the East Arsi zone. A total of 468 participants were included using a simple random sampling technique. Data were collected using a structured questionnaire and analyzed using binary logistic regression to assess associations between dependent and independent variables.
Result
More than half of the study participants (57.7%) exhibited low DHL, while 55.6% demonstrated poor self-care behavior. Significant factors associated with low DHL included being male, low education level, residing in rural areas, lack of diabetes education attendance, poor self-care behavior, and receiving diabetes information from only one source. Additionally, younger individuals, those living in rural areas, lack of exposure to diabetes education, and lower monthly incomes were significantly linked to poor diabetes self-care behavior.
Conclusion
These findings highlight the urgent need for targeted educational and behavioral interventions, particularly among rural residents, males, individuals with low income, low education, and those lacking exposure to diabetes education, to enhance DHL and improve self-care practices.
Introduction
Diabetes mellitus (DM) is a prevalent chronic illness characterized by elevated blood glucose levels due to insufficient insulin production or resistance (Yu et al., 2022). Type 1 diabetes is diagnosed in childhood and involves an autoimmune response, while type 2 is more common in adults and linked to lifestyle factors (Federation, 2021; Ling et al., 2024).
Diabetes has become a global public health crisis, affecting both developed and developing countries (Kumar et al., 2024). The International Diabetes Federation predicts 783 million people will have diabetes globally by 2045, affecting 40.7 million people in sub-Saharan Africa (Kumar et al., 2024; Mercer et al., 2019). In Ethiopia, approximately 1.3 million individuals are affected, with a prevalence rate of 3.2%, making DM one of the country's four priority noncommunicable diseases (Ababa, 2018). Rapid urbanization, population aging, sedentary lifestyles, and unhealthy diets are key contributors to the increasing burden (Ayele et al., 2012; King et al., 1998).
Diabetes imposes a heavy health burden due to its complications and associated disabilities (Dedefo et al., 2020; Zheng et al., 2018). For this matter, effective diabetes control relies on health literacy and patient involvement in self-care behaviors like medication, diet, blood sugar monitoring, exercise, risk reduction, problem-solving, and coping strategies (Care et al., 2021; Jannoo & Khan, 2019). Since approximately 98% of diabetes management depends on the patient's own efforts, health literacy becomes a vital determinant of successful control (Jannoo & Khan, 2019).
Literature Review
Health literacy is personal characteristics and social resources that enable individuals and communities to access, understand, evaluate, and use information to make informed health-related decisions (Kindig et al., 2004; Mogessie et al., 2022). Diabetes health literacy (DHL) involves comprehending appointment instructions, educational materials, and medication labels (Mogessie et al., 2022; Nutbeam, 2000a). Adequate health literacy facilitates self-care behaviors, which develop gradually through learning and adaptation (Shrivastava et al., 2013). Empirical evidence indicates a strong positive association between DHL and self-care performance higher literacy levels correlates with improved self-management and glycemic outcomes (Chahardah-Cherik et al., 2018; Marciano et al., 2019a; Protheroe et al., 2017; Shieh & Halstead, 2009).
Conversely, limited health literacy has been linked to poor diabetes knowledge, suboptimal self-care, and adverse health outcomes, including diminished quality of life (Gomes et al., 2020; Tsai et al., 2010). Poor adherence to self-care behaviors can lead to uncontrolled blood glucose and severe complications (Kassahun et al., 2016). Studies conducted in Ethiopia and Uganda have reported varying levels of self-care, highlighting the continued need for context-specific interventions in resource-limited settings (Kiruyi et al., 2023).
Low DHL often manifests as difficulty following medical instructions, low engagement in care, and psychological distress (Kolb et al., 2014; Mehzabin et al., 2019). Although prevalence estimates of low DHL range from 7.3% to 9.7% globally, some Asian countries report much higher rates of 71.7% to 82% (Abdullah et al., 2019). In Ethiopia, health literacy deficits affect 30.3% in Bale and 26.3% in Gondar (Mogessie et al., 2022) contributing to increased healthcare costs that account for 3% to 5% of total national health expenditure (Association, 2021).
Despite efforts to enhance patient education and promote health literacy, outcomes remain suboptimal due to poor utilization of available tools and sociodemographic barriers such as low education, advanced age, and poverty (Association, 2021; Wallace, 2010). Given Ethiopia's generally low literacy rate, assessing DHL is crucial for developing effective diabetes education strategies (Feleke et al., 2013). Other countries have recognized the negative consequences of limited health literacy and have implemented tailored interventions (Pleasant et al., 2015).
Effective diabetes control requires a multidimensional approach to prevent long-term complications (Misra et al., 2019). Since patients must continuously process and act upon complex health information, health literacy plays a central role in successful self-care (Ratzan & Parker, 2000).
In this study, the variables are framed within Nutbeam's Health Literacy Framework and the ADCES7 Self-Care Behaviors Framework. Nutbeam's model defines health literacy as a combination of functional, interactive, and critical components that shape individuals’ capabilities to access, comprehend, and utilize health information, thereby promoting better health outcomes (Nutbeam, 2000b). The ADCES7 framework specifies seven crucial self-care behaviors—healthy eating, physical activity, monitoring, medication adherence, problem-solving, risk reduction, and effective coping that are vital for successful diabetes management. By integrating DHL with self-care behaviors according to these frameworks, the study offers an in-depth perspective on how patients’ literacy levels are connected to specific actions that enhance diabetes control (Care et al., 2021b).
Although the link between DHL and self-care behaviors is well established, limited evidence exists from southeast Ethiopia, where sociocultural and resource factors may uniquely affect these outcomes. Therefore, this study aims to assess the level of DHL and self-care behaviors among adult diabetes patients receiving follow-up care at public hospitals in the Arsi zone, Oromia region, Ethiopia. The specific aims are: (1) To assess the level of DHL among adult diabetes patients attending follow-up clinics at public hospitals in the Arsi zone; (2) to determine the level of diabetes self-care behaviors among these patients based on the ADCES7 self-care domains; (3) to examine the association between DHL and self-care behaviors among adult diabetes patients; and (4) to identify sociodemographic and clinical factors associated with DHL and self-care behaviors.
Methods and Materials
Study Area and Period
The study was conducted from January 20 to February 20, 2025, in five public hospitals of the East Arsi zone, Oromia region (Asela, Abomsa, Bekoji, Kersa, and Robe Didaa). East Arsi spans 19,825 km2 with Asela as its capital, located 168 km south of Addis Ababa. The zone has an estimated population of 3.9 million and 1,621 adult diabetes patients attend monthly follow-up care in the zone's hospitals (Challa et al., 2019).
Study Design and Population
An institutional-based cross-sectional study was conducted among adult diabetes patients in selected public hospitals of the East Arsi zone. The study population included all adult patients attending follow-up care during the data collection period, with systematically selected individuals as the study units.
Inclusion and Exclusion Criteria
Adults aged 18 years and above who had diabetes for at least 6 months were included in this study. Patients who were severely ill, had hearing or visual impairments, or were unwilling to participate were excluded.
Sample Size Determination
The sample size was determined using a single population proportion formula with 95% confidence, 5% margin of error, and a design effect of 1.5. Based on previous studies, the estimated proportions were 30.3% for high DHL and 49.1% for poor self-care (Kassahun et al., 2016; Mogessie et al., 2022), yielding initial sample sizes of 487 and 576. The larger size (576) was adjusted for the finite population of 1,621, resulting in 425, and with a 10% nonresponse allowance, the final sample size was 468.
Sampling Technique
In the East Arsi zone, 10 public hospitals were identified, from which five (Asela Referral Hospital, Abomsa Primary Hospital, Bekoji Hospital, Kersa Primary Hospital, and Robe Dida’a General Hospital) were selected through a simple random sampling procedure (lottery method). For each selected facility, the total number of adult diabetes patients enrolled for follow-up care was obtained from patient records and the Health Management and Information System, along with their respective monthly follow-up counts.
Across these hospitals, Asela Referral Hospital had 696 monthly follow-up patients with 201 proportionally allocated samples; Abomsa Primary Hospital had 304 monthly follow-up patients with 88 samples; Bekoji Hospital had 88 monthly follow-up patients with 25 samples; Kersa Primary Hospital had 204 monthly follow-up patients with 59 samples; and Robe Dida’a General Hospital had 329 monthly follow-up patients with 95 proportionally allocated samples.
To ensure that the sample accurately reflected the distribution of patients with diabetes in the selected hospitals, the total study sample was proportionally allocated based on the number of monthly follow-up of adult diabetes patients in each facility. Finally, participant selection for interviews was carried out over the course of 1 month using systematic random sampling across the five hospitals based on total diabetic population (N) of 1,621 and a final sample size (n) of 468, the sampling interval was calculated as K = 3. Consequently, every third patient attending their scheduled follow-up appointment was selected for the study, following a randomly chosen starting point determined through a lottery method.
Study Variable
DHL and self-care behavior are both dependent variables where independent variables are sociodemographic factors (age, sex, religion, marital status, education, occupation, income, residency), psychosocial and resource factors (social support, information source, access to glucometer), and clinical factors (duration of diabetes, family history, fasting blood glucose level).
Operational Definition of Variables
DHL was measured using a 15-item tool with 5-point Likert scale (Nigussie et al., 2024). The mean score was calculated and then converted percentage (5 points as 100%) to determine the level of DHL. High DHL is defined as an assessment score of 75% or above, while low DHL is a score of 74% or below (Mogessie et al., 2022; Nigussie et al., 2024; Tefera et al., 2020). Self-care behavior was measured across six components of the Summary of Diabetes Self-Care Activities (SDSCA) tool (Toobert et al., 2000). Participants reported how many days in the previous week they have engaged in the self-care activity. The score was categorized as “good” (≥3 days) or “poor” (<3 days) based on the overall mean score (Wolderufael & Dereje, 2021).
Data Collection Tools and Procedure
Data were collected using a semistructured questionnaire adapted from previous studies, covering seven sections: sociodemographic factors, clinical factors, information access, diabetes knowledge (Fitzgerald et al., 2016), DHL (Lee et al., 2018), summary of diabetes self-care activities (Toobert et al., 2000), and Oslo Social Support Scale (Kocalevent et al., 2018). The questionnaire was validated using ratings by a panel of experts with interrater agreement of 0.82 for diabetes knowledge, 0.80 for DHL, 0.76 for SDSCA, and 0.78 for Oslo Social Support Scale. Nevertheless, due to resource limitations the researchers could not undertake a cultural adaptation procedure for these instruments beyond the translation work. Data were collected over 1 month through face-to-face interviews by five BSc nurses and two MSc supervisors trained in DHL and self-care. Eligible patients who consented were interviewed uniformly, with additional support provided when needed to ensure understanding.
Data Quality Control
The questionnaire was adapted from previous studies and translated into Afan Oromo and Amharic by two language experts, followed by back-translation into English to ensure both linguistic accuracy and conceptual equivalence. To enhance data quality, the instrument was pretested on 5% of the sample at Huruta Hospital, and its content validity was evaluated by subject-matter experts. The internal consistency of the instrument was assessed using Cronbach's alpha, yielding a value of .79, which indicates good reliability. Furthermore, data collectors and supervisors underwent comprehensive 2-day training covering the study objectives, interview techniques, and confidentiality procedures to ensure standardized and high-quality data collection.
Data Processing and Analysis
Data were entered and cleaned using EpiData 4.7 and analyzed with SPSS 27. Descriptive statistics were computed, and associations between independent and dependent variables were assessed using binary and multivariable logistic regression, reporting adjusted odds ratios (AORs) with 95% confidence interval (CI). The final model demonstrated an acceptable fit, as evidenced by the Hosmer–Lemeshow goodness-of-fit test (P = .72), a Nagelkerke R2 value of 0.56, and an area under curve of 0.84. Additionally, multicollinearity diagnostics using the variance inflation factor indicated acceptable values, ranging from 1.62 to 4.28.
Results
Sociodemographic Characteristics of Participants
A total of 468 adult diabetes patients participated in the study, yielding a 100% response rate. As shown in Table 1, most participants were male and the majority were aged 65 years and above. Nearly two-thirds were married and resided in rural areas. One-quarter had no formal education, while approximately one-fifth had attained college-level education or higher. Merchants, government employees, and housewives constituted the largest occupational groups.
Sociodemographic Characteristics of Diabetes Patients Attending Follow-Up Care at Public Hospitals in East Arsi Zone, Oromia Region, Ethiopia 2025 (n = 468).

Note. NGO = nongovernmental organization, ETB = Ethiopian Birr.
Wakefeta, juba.
Clinical and Behavioral Characteristics of the Study Participants
Type 2 diabetes accounted for the majority of cases, and more than half of the respondents reported a family history of the disease (Table 2). Over half experienced diabetes-related complications, most commonly hypertension. Insulin therapy was the predominant treatment modality. More than one-third of patients exhibited uncontrolled fasting blood glucose levels. Cigarette smoking was reported by nearly one-third of participants, and about one-third had lived with diabetes for fewer than 5 years.
Diabetes-Related Clinical and Behavioral Characteristics of Diabetes Patients Attending Follow-Up Care at Selected Public Hospitals in East Arsi Zone, Oromia Region, Ethiopia 2025 (n = 468).

Note. FBS = fasting blood sugar; DM = diabetes mellitus; OHA = oral hypoglycemic agent.
Information Access and Social Support
A considerable proportion of participants relied on a single source of diabetes information, and many reported limited social support. Approximately one-third described receiving insufficient concern from others during moments of personal difficulty. Overall, 34.6% of respondents had poor social support (Figure 1).
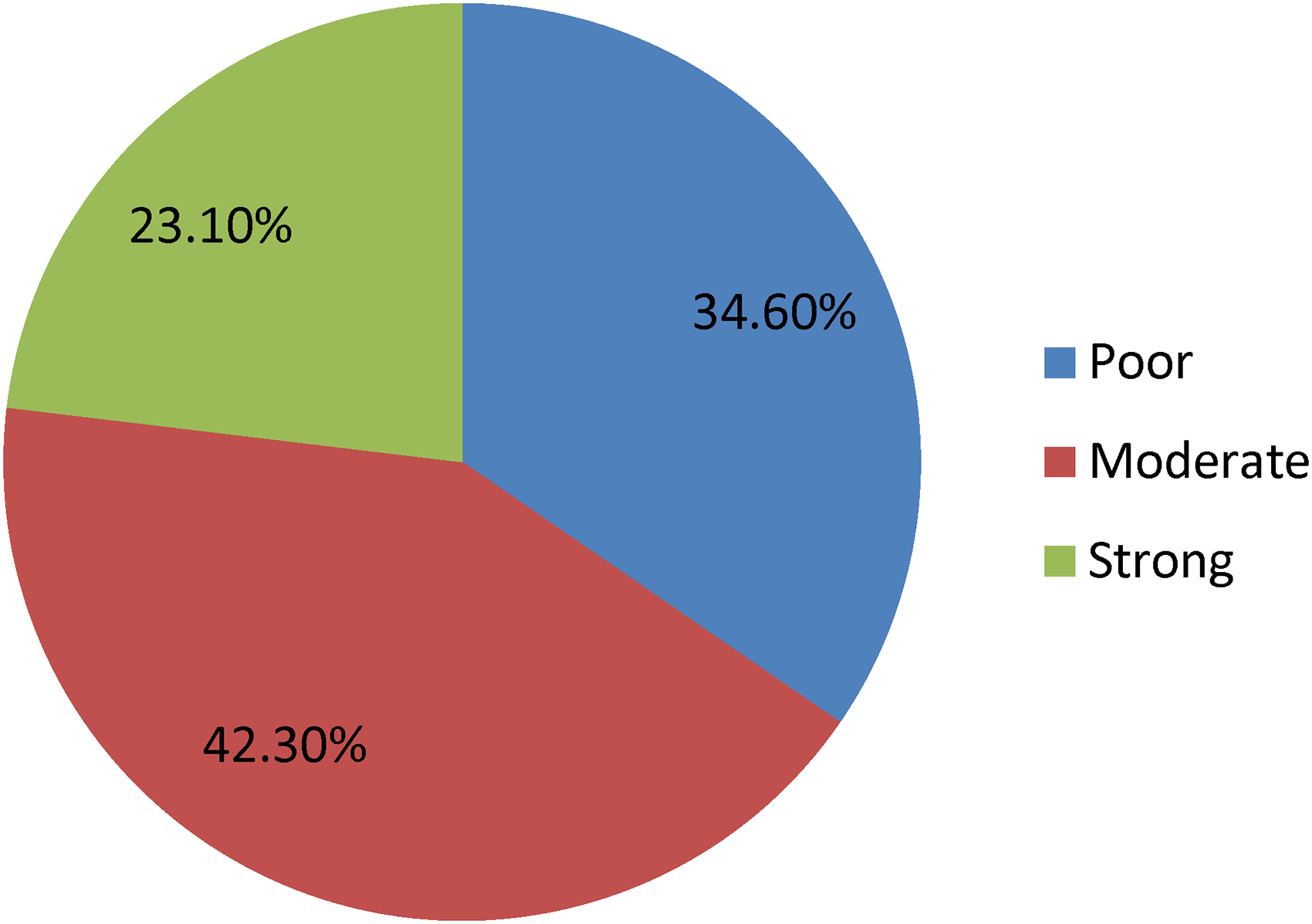
Status of social support for diabetes patients who attending follow-up care at selected public hospitals, East Arsi zone, Oromia, Ethiopia, 2025.
Diabetes Health Literacy
More than half of participants demonstrated low DHL (57.7%; Figure 2); notably, over one-third did not know the normal blood glucose range, and some expressed uncertainty regarding timing of medication doses or frequency of glucose monitoring. Nearly one-third reported difficulty comprehending education materials, and only a very small proportion routinely asked health professionals questions related to their condition. Detailed item responses are summarized in Table 3.

Status of diabetes health literacy for adult diabetes patient attending follow-up care at public hospitals, East Arsi zone, Oromia, Ethiopia, 2025 (n = 468).
Diabetes Health Literacy of Diabetes Patients Attending Follow-Up Care at Selected Public Hospitals in East Arsi Zone, Oromia Region, Ethiopia 2025 (n = 468).

Factors Associated With DHL
Multivariable logistic regression identified sex, education level, and residence, exposure to diabetes education, information sources, and self-care behavior as independent predictors of DHL (Table 4). Male patients were less likely to have high DHL (AOR = 0.60; 95% CI: 0.40–0.91). Individuals unable to read and write were less likely to have high literacy levels compared with those with college education or above (AOR = 0.52; 95% CI: 0.28–0.95). Rural residents were more likely to exhibit low health literacy (AOR = 1.62; 95% CI: 1.06–2.49). Patients who had never attended diabetes education sessions were more likely to have low literacy (AOR = 1.59; 95% CI: 1.00–2.51). Reliance on a single information source was associated with a lower likelihood of high literacy (AOR = 0.63; 95% CI: 0.41–0.96). Furthermore, participants with poor self-care practices were less likely to have high DHL (AOR = 0.56; 95% CI: 0.12–0.87).
Factors Associated With Diabetes Health Literacy for the Patient Attending Diabetes Follow-Up Care at Selected Public Hospitals, East Arsi Zone, 2025 (n = 468).

Note. COR = crude odds ratio; AOR = adjusted odds ratio; CI = confidence interval; 1 = reference.
*Significant at P-value <.05.
Diabetes Self-Care Behavior
More than half of the respondents (55.6%) had poor overall self-care behavior (Figure 3). The majority reported poor dietary habits, low levels of physical activity, and infrequent blood glucose monitoring. Nearly one-third smoked at least one cigarette in the previous week.

Status of diabetes self-care behavior for adult diabetes patient attending follow-up care at public hospitals, East Arsi zone, Oromia, Ethiopia, 2025 (n = 468).
Factors Associated With Diabetes Self-Care Behavior
In multivariable analysis (Table 5), age, residence, diabetes education, and monthly income were significant predictors of self-care behavior. Respondents aged 18–30 years were more likely to have poor self-care behavior compared with those aged ≥65 years (AOR = 3.40; 95% CI: 1.41–11.22). Rural residents were less likely to practice good self-care (AOR = 0.49; 95% CI: 0.32–0.76). Participants with no exposure to diabetes education were more likely to demonstrate poor self-care (AOR = 1.80; 95% CI: 1.11–2.90). Monthly income under ETB1,000 (AOR = 0.23; 95% CI: 0.09–0.59) and ETB1,001–2,000 (AOR = 0.53; 95% CI: 0.14–0.87) was associated with a lower likelihood of good self-care compared to those earning more than ETB5,000.
Factors Associated With Self-Care Behavior of Diabetes Patients Attending Follow-Up Care in East Arsi Zone of Selected Public Hospitals, 2025 (n = 468).

Note. COR = crude odds ratio; AOR = adjusted odds ratio; CI = confidence interval; 1 = reference.
*Significant at P-value <.05.
Discussion
This study examined the levels of DHL and self-care and their associated factors among adults with diabetes in public hospitals in the East Arsi zone, Oromia region. In this study, 57.7% of participants had low DHL and 55.6% demonstrated poor self-care behavior. Low DHL was linked to being male, having lower education, rural residence, limited health information, lack of diabetes education, and poor self-care. Poor self-care, in turn, was associated with younger age, rural residence, low income, and not receiving diabetes education. These findings highlight substantial gaps in both DHL and self-care, emphasizing the need for targeted education and system-level interventions.
Diabetes management relies heavily on patients’ active engagement, which is largely determined by their DHL: the ability to access, understand, evaluate, and use diabetes-related information (Alidosti & Tavassoli, 2019; Singh & Aiken, 2017). Effective self-care behaviors, including maintaining a proper diet, foot care, medication adherence, regular blood glucose monitoring, physical activity, and avoiding smoking, are key indicators of diabetes self-care and overall disease management (Care et al., 2021; Jannoo & Khan, 2019).
In this study, 57.7% of participants had low DHL. This prevalence is higher than reported in the European Health Literacy Survey (Sørensen et al., 2015), Saudi Arabia, and the United States (ALSharit & Alhalal, 2022; Ratzan & Parker, 2000) but lower than that in South Korea (Jeong & Kim, 2016). These differences may reflect variations in measurement tools, scoring methods, sample characteristics, study settings, healthcare system emphasis on diabetes education, and broader socioeconomic and cultural contexts.
The proportion of participants with high DHL (42.3%) was lower than findings from China (52.9%), Israel (69%), and Singapore (80.5%; Doubova et al., 2019; Mohammadi et al., 2015) but higher than studies from Mexico (17.6%), Iran (18.2%), and Kigali, Rwanda (14.3%; ALSharit & Alhalal, 2022; Al-Maskari et al., 2013; Doubova et al., 2019; Mohammadi et al., 2015; Mukanoheli, 2019). Differences may arise from variations in the study context, tools used to assess DHL, and the level of structured diabetes education across settings.
Compared with previous Ethiopian studies, the proportion with high DHL in the present study was higher than Bale (41.8%), Debre Berhan (49.1%), and Gondar (26.3%; Nigussie et al., 2024; Mogessie et al., 2022; Tefera et al., 2020). These variations may relate to differences in the proportion of participants with low educational status, sample size differences, and slight modifications to data collection instruments across studies.
Male gender in this study was significantly associated with low-level DHL. This finding is consistent with study done in Iran, China, and Rwanda (Mohammadi et al., 2015; Mukanoheli, 2019; Zhao et al., 2021), and while it is inverse with that of study conducted at Gonder (Tefera et al., 2020). These discrepancies may relate to sociocultural differences, gendered health-seeking behaviors, and variations in study settings.
Educational status showed a significant association with DHL. Participants with lower educational attainment had lower DHL, consistent with findings from Iran, China, Rwanda, Gondar, and Bale (Mohammadi et al., 2015; Mukanoheli, 2019; Nigussie et al., 2024; Tefera et al., 2020; Zhao et al., 2021). Higher education may enhance the ability to interpret health information and access diverse information sources or may be mediated by health literacy in doing so. Previous studies have indicated that health literacy mediates the relationship between socioeconomic position including educational status and health-related outcomes, health behaviors, and use of preventive services (Friis et al., 2016; Lastrucci et al., 2019; Stormacq et al., 2019). This implies the need for further study to determine whether DHL mediates the relationship between educational status and utilization of health information, diabetes self-care behaviors, and diabetes-related health outcomes.
Rural residence was associated with lower DHL, similar to findings from Gondar (Tefera et al., 2020). Limited access to health information and poor socioeconomic position including fewer educational opportunities in rural settings may contribute to this pattern. Previous studies have described that place of residence potentially acts as a proxy for socioeconomic position to predict health literacy (Aljassim & Ostini, 2020; Bíró et al., 2021). Thus, rurality in our study might have acted as a proxy for socioeconomic positions such as educational status in predicting lower DHL.
Exposure to diabetes education was positively associated with higher DHL, aligning with findings from Malaysia (Abdullah et al., 2020). Other previous studies have described that health literacy as predictor of diabetes knowledge with the latter mediating the relationship between the former and both self-care behaviors and glycemic control (de Carvalho et al., 2025; Marciano et al., 2019b). Thus, participants with higher health literacy in our study might have displayed better diabetes knowledge. However, since mediation analysis was beyond the scope of our study, we recommend future studies to carry out this work.
Having multiple sources of diabetes information was positively associated with higher DHL, consistent with findings from Bale (Mogessie et al., 2022). Access to diverse information sources may enhance diabetes knowledge, self-care behaviors, and glycemic control through improved DHL. Nevertheless, the trust in the source and the quality and clarity of the information are important to avoid confusion and misunderstanding (Inoue et al., 2013; Lee & Lin, 2011). Therefore, nurses as frontline health professionals should make sure that patient with diabetes access trusted, clear, and quality source of information.
Participants with poor self-care practices were significantly less likely to have high DHL. This finding aligns with previous research (Chahardah-Cherik et al., 2018; Marciano et al., 2019a) showing that higher DHL improves adherence to key self-care behaviors such as dietary management, physical activity, medication adherence, and blood glucose monitoring by enhancing patients’ ability to access, interpret, and effectively use diabetes-related information. Though conducting a path analysis was beyond the scope of our study, the link between health literacy and diabetes self-care behaviors might have been mediated by other variables not measured in this study. Previous studies have explained that motivations and self-efficacy (Lee et al., 2016; Nam & Yoon, 2024), empowerment (Shin & Lee, 2018), knowledge and patient activation (Kim, 2021), and patient engagement (Cengiz et al., 2022) mediate the relationship between health literacy and diabetes self-care behaviors. Thus, while cautioning readers to understand our study findings within this limit, we suggest future studies to conduct structural equation modeling to clarify the pathways linking health literacy and diabetes self-care behaviors. No significant association was observed between DHL and age or family history of diabetes, consistent with studies from northeast Iran (Doubova et al., 2019; Mohammadi et al., 2015) and Bale (Mogessie et al., 2022).
The proportion of participants with good diabetes self-care practice in this study was 44.4%, which is higher than findings from Malawi, Mexico, and Uganda (Banda et al., 2019; Baquedano et al., 2010; Kiruyi et al., 2023), but lower than results from Tigray, Nekemte, Jimma, and Nazila (Chinnappan et al., 2020; Dedefo et al., 2019; Kassahun et al., 2016; Molalign Takele et al., 2021). These variations may reflect differences in study design, sample size, and population characteristics, particularly in institution-based studies. It is similar to reports from Debre Berhan (Gebre et al., 2020) likely due to the use of comparable measurement tools and criteria for assessing diabetes self-care practices.
This study demonstrated that 67% of participants failed to meet recommended dietary practices in the preceding 7 days, with only 33% achieving appropriate dietary adherence. This proportion is substantially lower than adherence rates reported in Sri Lanka, Bangladesh, and Nigeria (Ariyo et al., 2023; Paudel et al., 2022; Saumika et al., 2019) and several regions of Ethiopia, including Tigray, northeast Ethiopia, and Nekemte (Dedefo et al., 2019; Gebre et al., 2020; Molalign Takele et al., 2021). The markedly reduced adherence observed in this population may be attributable to structural and contextual determinants such as food insecurity, economic limitations, and prevailing sociocultural dietary norms. Methodological differences across studies such as variations in measurement tools, recall periods, and potential recall or social desirability bias may also influence the observed discrepancies. These findings highlight critical gaps in dietary self-management and underscore the need for targeted, context-specific nutritional interventions to improve diabetes care outcomes.
Only 20.5% of participants met the recommended physical activity levels, a proportion much lower than reports from Sri Lanka, Bangladesh, Malawi, and several sub-Saharan African countries (Banda et al., 2019; Palermi et al., 2022; Paudel et al., 2022; Saumika et al., 2019), as well as findings from Dire Dawa, Dilla Referral Hospital, and Nekemte in Ethiopia (Addisu et al., 2014; Dedefo et al., 2019; Ketema et al., 2020). Sociocultural norms, occupational demands, and environmental constraints may contribute to the low activity levels observed.
Blood glucose self-monitoring was practiced by 34.8% of participants, a proportion lower than those reported in the United Kingdom, Bangladesh, and the United Arab Emirates (Al-Maskari et al., 2013; Barnard et al., 2010; Saleh et al., 2014), but higher than findings from Tigray and Nekemte (Dedefo et al., 2020; Molalign Takele et al., 2021). Notably, 65.2% of participants did not own a glucometer, which may hinder regular monitoring, consistent with evidence from Dire Dawa (Getie et al., 2020). These variations may be explained by differences in sample size, geographic context, socioeconomic conditions, and study settings.
A high proportion (87%) reported good foot-care practices, higher than studies from Bangladesh, Tanzania, Malawi, Addis Ababa, Benishangul-Gumuz, and Nekemte (Banda et al., 2019; Berhe et al., 2013; Chali et al., 2018; Chiwanga & Njelekela, 2015; Dedefo et al., 2019; Saleh et al., 2014) but slightly lower than Jimma Medical Center (Hirpha et al., 2020). Differences may reflect variations in education, socioeconomic conditions, and patient counseling. Medication adherence was high (97%), exceeding rates from Sri Lanka, Saudi Arabia, Zewditu Hospital, Bahir Dar, and Jimma (Abate, 2019; Alqarni et al., 2018; Ali et al., 2017; Kassahun et al., 2016; Saumika et al., 2019). Differences may relate to variations in education, access to medications, and health literacy across settings. More than one-fourth of participants (29.5%) reported cigarette smoking, predominantly among males. This prevalence is lower than findings reported in India (Islam et al., 2020) and Tigray (Molalign Takele et al., 2021). These discrepancies may be attributable to sociocultural norms and differences in study settings as well as variations in participants’ awareness of the health risks associated with smoking.
Strength and Limitation of the Study
There are notable strengths of the present study. First, the cross-sectional design of the study offered sufficient sample size for analysis. Second, the use of face-to-face interviewer-administered questionnaire helped to overcome the problem of nonresponse. Third, analysis of the association between DHL and diabetes self-care can be considered as the first of its kind in Ethiopia. The limitations of this study should be acknowledged. Its cross-sectional design limits the ability to infer causal relationships, and reliance on self-reported information may introduce recall and social desirability biases, particularly for sensitive behaviors such as dietary practices and smoking. Some important contextual factors, such as cultural practices, health system barriers, and food insecurity, were not assessed. Our inability to account for some potential confounders such as body mass index, comorbidities, severity of diabetes, and general health literacy can be considered as limitations of the study. In addition, systematic sampling based on clinic attendance may have excluded individuals who missed appointments or were hospitalized during data collection. The study was also conducted in a single zone, which may limit the generalizability of the findings to other regions. Lastly, the relatively lengthy questionnaire may have contributed to respondent fatigue.
Implications for Nursing Research and Practice
The findings of this study imply that targeted diabetes education should be prioritized for populations associated with low DHL, including rural residents, individuals with limited education, and male patients. Diversifying information channels (e.g., visual materials, mobile-based reminders, community health education) may improve DHL and self-care. Particularly, structured, culturally tailored, nurse-led diabetes self-management education in the community can specifically help to address the identified gaps. Routine screening for DHL during follow-up visits can help health care providers tailor counseling to patients’ comprehension levels. Strengthening self-care support, particularly diet and physical activity counseling, is essential for younger patients and those with low income or limited access to glucose-monitoring tools. Enhancing rural outreach programs may reduce information disparities and improve both DHL and self-care behaviors. Moreover, future longitudinal and/or interventional studies are recommended to strengthen the evidence base to clarify cause relationships.
Conclusion
Overall, both DHL and self-care behavior were suboptimal compared to several Ethiopian studies. Low DHL was associated with male sex, lower education, rural residence, limited information sources, lack of diabetes education and poor self-care. Poor self-care was associated with younger age, rural residence, low income, and absence of diabetes education. These findings highlight the need for tailored diabetes education strategies, routine DHL assessment, and strengthened nursing interventions to improve patient engagement and disease management. Policy efforts should prioritize integrating structured diabetes education into primary healthcare and expanding community-based health literacy initiatives, particularly in rural and low-income settings. In clinical practice, implementing DHL screening, using culturally appropriate educational tools, and providing individualized counseling are essential.
Footnotes
Acknowledgments
Our deepest gratitude goes to Addis Ababa University. We would also like to thank the Public hospitals staff and the study participants for generously sharing their time and experiences, without which this research would not have been possible.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board with Protocol number: SNM/01/2025 and permission from the Oromia region to conduct the study. Privacy and confidentiality of the study participants were maintained and written informed consent were obtained from each participant.
Author Contributions
Study conception and design: ABE and FA, data collection: ABE, data analysis and interpretation: ABE and FA, drafting of the article: AB, and critical revision of the article: ABE, FA, and AB.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset used and/or analyzed during the study was available from the corresponding author upon reasonable request.