
Abstract
Background
Diabetes mellitus (DM) is one of the most common chronic diseases globally. Despite the presence of national strategies to prevent potential sequelae DM has been associated with increased morbidities and mortality in Ethiopia, and the prevalence appears to be on the rise. Although studies have been conducted among DM patients in the country, there is a lack of information that could allow an in-depth understanding of the situation.
Objective
To assess dietary practices and associated factors among adult DM patients at academic tertiary-level hospitals in central Ethiopia.
Methods
The institution-based concurrent mixed-methods study was conducted from January 01 to 30 2024 involving 420 adult DM patients. Participants were selected using a simple random sampling technique for quantitative study. A purposive sampling technique was used to select 16 participants for qualitative analysis. For the quantitative study, a self-administered structured questionnaire was used to collect data, and an in-depth interview for the qualitative part. Multivariate binary logistic regressions were used to assess the explanatory variables associated with dietary practice. A thematic analysis was performed for qualitative data.
Result
Of 420 eligible participants, 406 (96.7%) participated in the study. The overall proportion of good dietary practices among participants was 172 (44.2%). The being female, urban residence a family history of DM, and good dietary were significantly associated with the dietary practice. From qualitative analysis, two themes have emerged; Living as before and not adhering to diabetic dietary recommendations and barriers to adherence to effective eating practice.
Conclusions and recommendations
Less than half of adult DM patients had good dietary practices. Sex, geographic location, family history of DM, and level of knowledge of diabetic diet were associated with dietary practice. Intervention programs on awareness creation and training to improve the dietary practice by stakeholders were recommended.
Introduction
Diabetes mellitus (DM), a set of metabolic disorders, is characterized by persistent high blood glucose levels because of errors in insulin secretion, its action, or both (Care, 2015). The dietary practices of patients refers to their food choices, which are guided by diabetes nutrition education focusing on consuming foods that are low in fat, high in fiber, and low in sodium (Shamsi et al., 2013). Good dietary practices are considered one of the pillars of diabetes management (Simegn & Moges, 2022).
In Africa, the prevalence of diabetes and the mortality and disability caused by diabetes are increasing. In the next 25 years, it is anticipated that an increase in sedentary behavior, a fast-expanding urban culture, and altered diets will quadruple the prevalence of DM (Ambachew et al., 2015).
According to estimates from the International Diabetes Federation (IDF), Ethiopia had 1.92 million (5%) adult people aged 20–79 years with diabetes, making it the largest diabetes population in sub-Saharan Africa (Simegn & Moges, 2022).
In Ethiopia, systematic review shows the prevalence of DM in Ethiopia ranged from 2.0% to 6.5% (Zeru et al., 2021). According to a previous study conducted in Ethiopia, the prevalence of good dietary practices varies from place to place; it was 40.6% at Arba Minch General Hospital, Gamo Zone (Worsa et al., 2021), 53.8% in Dire Dawa (Gebeyehu et al., 2022), and 64.1% at Felege Hiwot Referral Hospital in Bahir Dar City (Demilew et al., 2018b). Currently, one of the most prevalent non-communicable diseases in the world is diabetes (WHO, 2016), with significant diabetic complications. The most common reported diabetic complications are retinopathy (2.7–25%), neuropathy (4.8–35%), kidney disease (18.2–23.2%), hypertension (23–54.8%), and depression (13–61% (Cho et al., 2018).
World Health Organization recommends that patients maintain a healthy body weight, engage in regular physical exercise for at least 30 min and moderate-intensity activity per day, eat a nutritious diet, refrain from using tobacco products, and achieve and maintain a healthy body weight (Ayele et al., 2018). The American Diabetes Association (ADA) recommends that eating fruits, vegetables, whole grains, legumes, and fiber-containing foods and minimizing foods containing high sucrose are beneficial for secondary prevention of T2DM (WHO, 2016).
Review of Literatures
Various studies have shown that dietary practices in diabetic patients are strongly associated with factors such as nutrition education (Wang et al., 2014), education level, family support, gender, age, presence of comorbidity, income, employment status, disease knowledge, and dietary advice quality (Tadesse et al., 2019; Tiew et al., 2014).
While previous studies carried out in central Ethiopia have focused on quantitative findings, this study aims to provide a deeper understanding of dietary practices and associated factors among adult patients with DM in central Ethiopian tertiary hospitals in 2024 by combining quantitative and qualitative data.
Methods and Materials
Study Approach
The study was conducted using a convergent mixed method approach from January 01–30, 2024.
Study Area
The study was carried out in tertiary hospitals in central Ethiopia. In the region, there are three tertiary level hospitals: Wolikite, Worabe, and Wachemo tertiary level hospitals.
Wolikite university hospital is located in wolikite town in 172 kilometer south of Addis Abeba, 14 kilometer along Butajira to Wolikite town. The hospital was established in 2018 as part of teaching hospital for health science students. In addition to teaching the students, the hospitals give preventive, curative, and rehabilitative clinical services structured into four case teams in outpatient, inpatient, emergency, and maternal and child health. In the outpatient department, the hospital has two DM follow-up OPD rooms to patients requiring regular monitoring (Wondie et al., 2022). Currently, the clinic oversees a total of 1150 diabetic patients, with 690 of them diagnosed with Type II DM.
Worabe Hospital is located 172 km south of Ethiopia's capital, Addis Ababa, in Worabe, a town. The hospital is organized into outpatient, obstetrics and gynecology, internal medicine and surgery. Diabetic follow-up clinic is found under outpatient department. There are around 900 DM patients on follow-up and out of them 610 were diagnosed as type two DM.
The Wachemo Hospital referral is located in hosanna town, 232 km south of Addis Ababa, Ethiopia's capital city. It has around 18 outpatient departments. It supports three district hospitals and 65 health centers. In addition to teaching the students, the hospitals give preventive, curative, and rehabilitative clinical services structured into four case teams in outpatient, inpatient, emergency, and maternal and child health. In the outpatient department, the DM follow-up clinic caters to patients requiring regular monitoring. Currently, the clinic oversees 1300 diabetic patients, with 890 of them diagnosed with Type II DM.
Populations
Source Population
All adults diagnosed with DM at regular follow-up at the diabetes follow-up clinic.
Study Population
Those randomly selected adult patients with DM who had regular follow-ups and met the inclusion criteria were considered as our study population for the quantitative study.
The people selected were adult patients with diabetes mellitus who had regular follow-ups and met the inclusion criteria and were considered our study population for the qualitative study.
Inclusion and Exclusion Criteria
Inclusion Criteria
For the quantitative study, diabetes patients over 18 years and who followed up at least once in advance of the actual data collection period were included.
For qualitative study, patient diagnosed with DM and whose age <18 years, duration of the illness <6 months, willing to participate in the study and gave their informed voluntary consent were included
Exclusion Criteria
Mentally incompetent and unable to listen or speak were excluded from the study.
A qualitative study of excluded criteria: pregnant women, patients with known mental problems, communication problems, and serious illness.
Sample Size Determination
To determine the sample size for the quantitative study, the outcome variables were considered, the prevalence of poor dietary practices p = 53.7% (Erkocho et al., 2022) was used to estimate the minimum sample size to achieve the objective of the study. Then calculated using a single population proportion and considering the following assumptions, a level of confidence of 95% with the corresponding value (1.96 for normal distribution) and absolute precision of 5%. The following statistical formula was used:

p = 53.7% prevalence of poor dietary practices in a similar study
z = the standard value for normal distribution with a confidence level of α = 95%
d = the error margin between the sample and the population (0.05).
Z = 1.96, P = 53.7%, d = 5% = 0.05,
Add 10% by considering the non-response rate which is equal to 420.
The sample size of the specific objective was determined considering significantly associated factors with the two-sided confidence level of the outcome variable of 95%, power 80%, and the ratio of exposed to unexposed 1:1 using Epi Info Version 7.2.2.6 and the calculated sample size for the selected factors are shown in Table 1.
Sample Size Determination to Conduct a Study on Dietary Practices and Associated Factors.

Finally, the required sample size for this particular study was decided by taking the maximum sample size (i.e., first specific objective = 382) from the calculated sample size and then adding 10% considering the non-response rate, therefore, 420 samples of study participants required to carry out this particular study.
For the qualitative study, the sample size was determined based on data saturation. A total of 16 participants were included in the qualitative study.
Sampling Techniques and Procedure
Sampling for the quantitative study was carried out after obtaining the average three-month number of patients with DM who have follow-ups in tertiary hospitals. The total sample size was distributed proportionally according to the number of diabetic patients at follow-up in each academic tertiary hospital as shown in Figure 1.

Sampling procedure to select study participants from academic tertiary level hospitals.
A systematic random sampling technique was used to select study subjects from tertiary hospitals based on patient flow during the study period. The sampling interval was obtained by dividing the sampling proportion in three three-month average numbers (N) by the number of samples (n). The K-value, representing the interval for patient selection, was determined by dividing the total number of type-2 diabetic patients in Wachemo University Referral Hospital (890 patients), Wolikite University Referral Hospital (690 patients), and Worabe Comprehensive Hospital (610 patients) by the respective allocated proportions for each hospital (171, 132, and 117). This method ensured a systematic approach to patient selection, with every 5th patient being chosen for inclusion in the study. The initial sample for each hospital was selected randomly from the range of 1 to K, ensuring a fair and unbiased representation of patients across the different healthcare facilities.
The first participant (starting individual) was selected using the simple random sampling technique, and then other study participants were selected through every K interval using the systematic sampling technique until the desired sample size.
A purposive sampling strategy was used to select study participants for qualitative study. Qualitative data were obtained from the same existing patients from the quantitative sample. Sampling and data collection were continued until data saturation was reached and no new data was obtained from the interviews.
Study Variables
Dependent Variable
Dietary practices of the patient with DM
Independent Variable
Data Collection Procedure
Data from the quantitative study were collected by three BSc nurses and supervised by the principal investigator. The data collectors were trained for one day by the principal investigator about the purpose of the study, tools, and sampling methods. Data were collected after obtaining written informed consent from study participants by data collectors through structured questionnaires administered by interviews. Data was collected after obtaining informed consent from the study participants by data collectors through structured interviewer administers questionnaires.
One-to-one interviews were conducted in Amharic in a quiet and private room, free from disturbances, and where study participants felt safe. The interview session ranged from 25 to 30 min. With the participants’ written consent, the primary investigator recorded the interviews and took notes during the interview to capture the original accounts of the participants’ responses. On the same day, each interview was transcribed and translated into English by cross-checking both the audio record and the notes. The transcripts of each interview were read and reread to gain an understanding of the whole situation and then reread slowly to determine its significant features.
Operational Definition
Data Collection Instrument
The questionnaire administered by the interviewer was adapted from different literature on the dietary practices of DM patients (Gebeyehu et al., 2022; Worsa et al., 2021). The tools contain 42 questions which were designed to cover the following sections: participant's socio-demographic characteristics, health profile-related questions, knowledge measurement questions, and dietary practices measurement questions of patients with DM.
To assess health profile-related questions, 10 items were used. The tool's reliability in the current study was tested using the data from the study data, and Cronbach's alpha value was 0.961.
To assess knowledge of participants diabetic diet was assessed using. In a previous study, Cronbach's alpha was recorded as 0.65 (Gebeyehu et al.), the tool's reliability in the current study was tested using the data from the study data, and Cronbach's alpha value was 00.83. A visual examination of the histogram revealed that the knowledge scores was approximately normally distributed and had a skewness of −0.372 (SE = 0.121) and a kurtosis of −0.529 (SE = 0.241), indicating it is normally distributed. After reverse scoring for one negative items (item 7), the overall mean was calculated. Respondents who scored more than the mean on the total of all knowledge related questions were categorized as having a “Good knowledge” otherwise “poor knowledge.”
To assess dietary practices measurement questions of patients with DM was used. The general dietary guidelines of the South African Diabetes Association and Amalmal Worku's modified version of the fifteen Morisky medication adherence scale (MMAS-8) were used to produce the questionnaires used to evaluate the dietary practices of DM patients (Morisky & DiMatteo, 2011). It comprised 15 components, and the mean value was used to categorize the respondents’ dietary practices into good and poor categories. Each of the items contains two response options (Yes = 1and No = 0), here yes was used for those responses which were negatively answered or far true answer from what science is talking about. As a result, by selecting Yes or No for each statement, respondents were able to select the correct response. Ultimately, the variables related to dietary practices were calculated and scores were assigned to the respondents’ dietary practices. In a previous study, Cronbach's alpha was recorded as 0.65 (Gebeyehu et al.). After reverse scoring for one negative items (item 5, 6, and 11), the overall mean was calculated. The mean score was calculated after checking the normality of the distribution. A visual examination of the histogram revealed the dietary practices measurement questions of patients with DM. Scores was approximately normally distributed and had a skewness of 0.034 (SE = 0.121) and a kurtosis of 0.175 (SE = 0.241), indicating it is normally distributed. Respondents who scored more than the mean were considered “good dietary practices” otherwise “poor dietary practices.”
In-depth interviews were conducted to collect qualitative data. The interview was guided by an in-depth interview guide developed from the existing academic literature and a discussion among the principal investigator and immediate supervisors (Supplemental material). Purposive sampling was used to choose participants for in-depth interviews and conducted face-to-face interviews with participants. An interview guide was utilized to outline open topics. The interview contained open-ended questions that covered socio-demographic characteristics. What do you think about the role of a diabetic diet in controlling your blood sugar level? Have you received information from your healthcare provider on the importance of adhering to dietary modifications? Are you able to adhere to dietary modifications?
Data Quality Control
To achieve the quantitative data quality control issue of quantitative data, training was given to data collectors and supervisors using the local language (Amharic). The questionnaire was translated into the local language for data collection and then retranslated back into the English version to check for consistency. A pre-test was conducted at Sodo Comprehensive Specialized Hospital to ensure its consistency and errors will be corrected. Short-term discussions were held after each data collection day with all data collectors and supervisors to address challenges and to make them clear on how to solve the challenges they faced. The completeness of each questionnaire was checked by the principal investigator and supervisors daily.
After being recorded in Amharic, the qualitative data were transcribed and analyzed in English. The QDA (qualitative data analysis) miner software was used to enter and analyze the qualitative data that had been transcribed. Thematic analysis was performed using an inductive approach.
To ensure the credibility of the study, sustained interaction with participants, and to preserve data source triangulation, in-depth research was conducted in a confidential and comfortable setting among those participants. To ensure the dependability of the study, the audio tape was transcribed in Amharic word by word before being translated into English by cross-checking both the audio record and the notes. Transcripts of each interview were read and reread to gain an understanding of the whole situation and then reread slowly to determine its significant features. To ensure the conformability of the study, an interview guide was used and the semi-structured interview guide allowed focus and flexibility during the interview by coding the participants’ own words instead of the researchers’ opinions. To ensure the transferability of the study, purposive quota criteria and data saturation during the interview were used.
Data Processing and Analysis
The data was cleaned and coded, then entered into Epi-data version 4.6 software and exported to SPSS version 25 for analysis. Different dummy tables, graphs, and descriptive summaries were used to present the study variables. Binary logistic regressions were performed to assess the strength of the association between each independent variable and the outcome variables. Hosmer and the Lemeshow goodness of fit test were done to determine the model's fitness. All variables with p-values less than .25 in bivariate logistic regressions were fitted into the backward stepwise multivariable logistic regression model. Finally, only those independent variables that maintain their association with outcome variables in multivariate regressions (p-value <.05) were declared statistically significant. The odds ratio with its p-value and confidence interval will be used or reported in each logistic regression analysis. To measure the strength of the association between the outcome and the independent variables, the crude odds ratio (COR) and the adjusted odds ratio (AOR) along with a 95% confidence interval (CI) were calculated.
Results
Quantitative Result
Socio-Demographic Characteristics
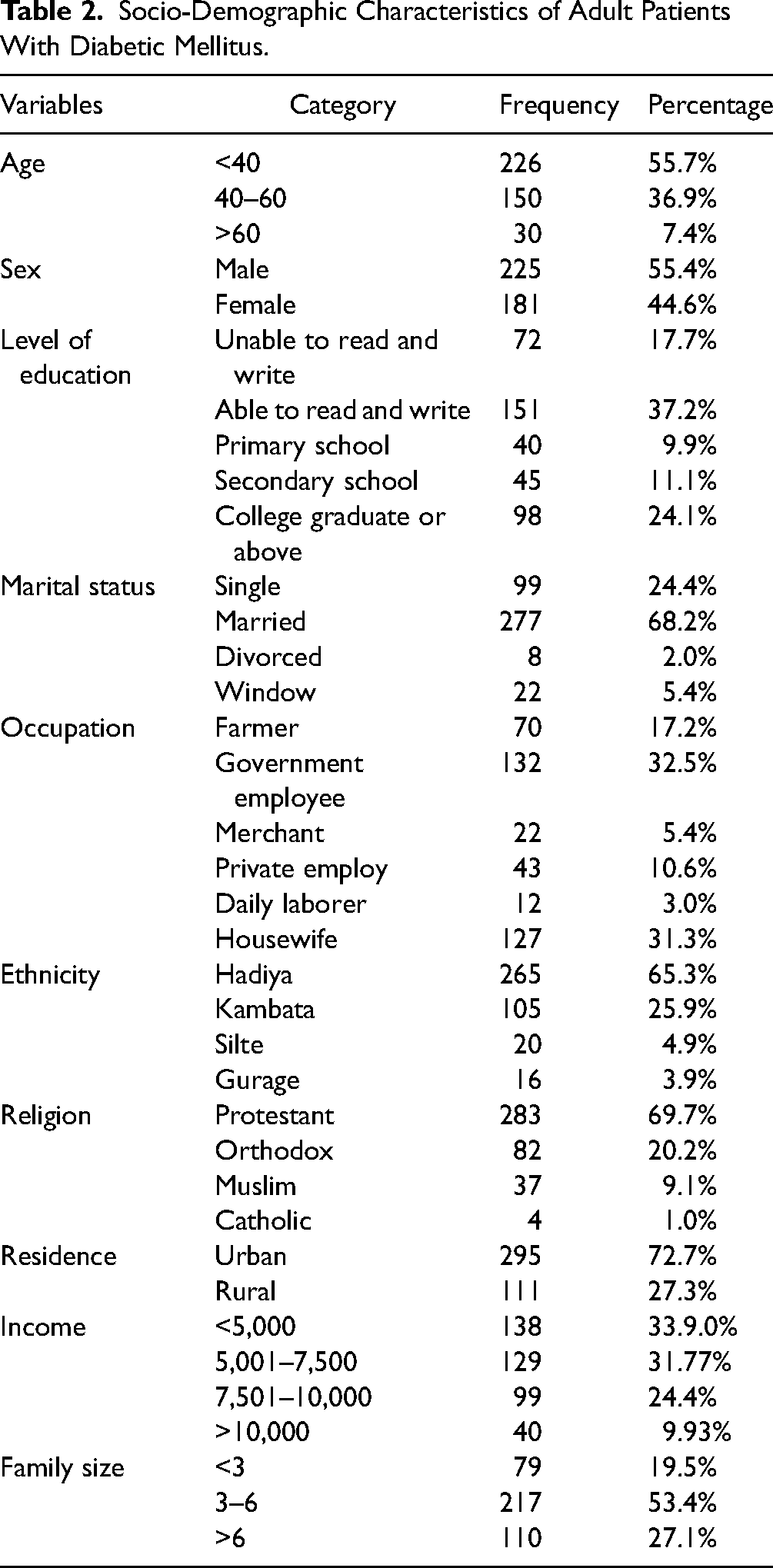
Of 420 eligible DM patients, 406 (96.7%) participated in the study. More than half 225 (55.4%) of the participants were male. The mean age (±SD) of the participants was 42.07± (11.525) years with an age range from 23 to 78 years. The majority of the study participants (55.7%) were less than the age group of 40 years. Of the participants, two-thirds, 265 (65.3%), were Hadiya in their ethnicity, and more than two-thirds, 283(69.7%), of the participants were protestant religious followers (Table 2).
Socio-Demographic Characteristics of Adult Patients With Diabetic Mellitus.
Health and Information-Related Profile
More than half, 245(60.3%), of the participants had diabetic duration >36 months and one-third 135 (33.3%) of them were on follow-up for between 12 and 36 months. One hundred twenty-six (31%) and 170 (41.9%) participants had comorbidity and family history of DM, respectively (Table 3).
Health-Related Profile of Adult Patients With Diabetic Mellitus on Follow-up.

Barriers to following a dietary plan
Regarding barriers to following the dietary plan, family support (7.4%), cost of healthy food, 113 (27.8%), and availability of fruit, 57 (14%), were the major ones (Figure 2).

Barriers to follow a dietary plan.
Proportion of dietary knowledge of diabetic patients
The overall proportion of good dietary knowledge among diabetic patients was 45.8% (Figure 3).

Proportion of dietary knowledge of adult patients with diabetic mellitus.
Proportion of Dietary Practices of Diabetic Patients
Among our study participants, 38.9% reported having a planned meal ahead, 43.6% followed a flexible meal plan, and only 41.6% consumed vegetables more than three times a day. On the contrary, 24.1% of the participants adhered to a specific diet plan and 4.2% consumed fruit more than three times a day (Table 4).
The Dietary Practices of Adult Patients With Diabetic Mellitus.

The overall proportion of good dietary practice among diabetic patients was 172 (42.4%) [95% CI (37.7–47.5)], see (Figure 4).
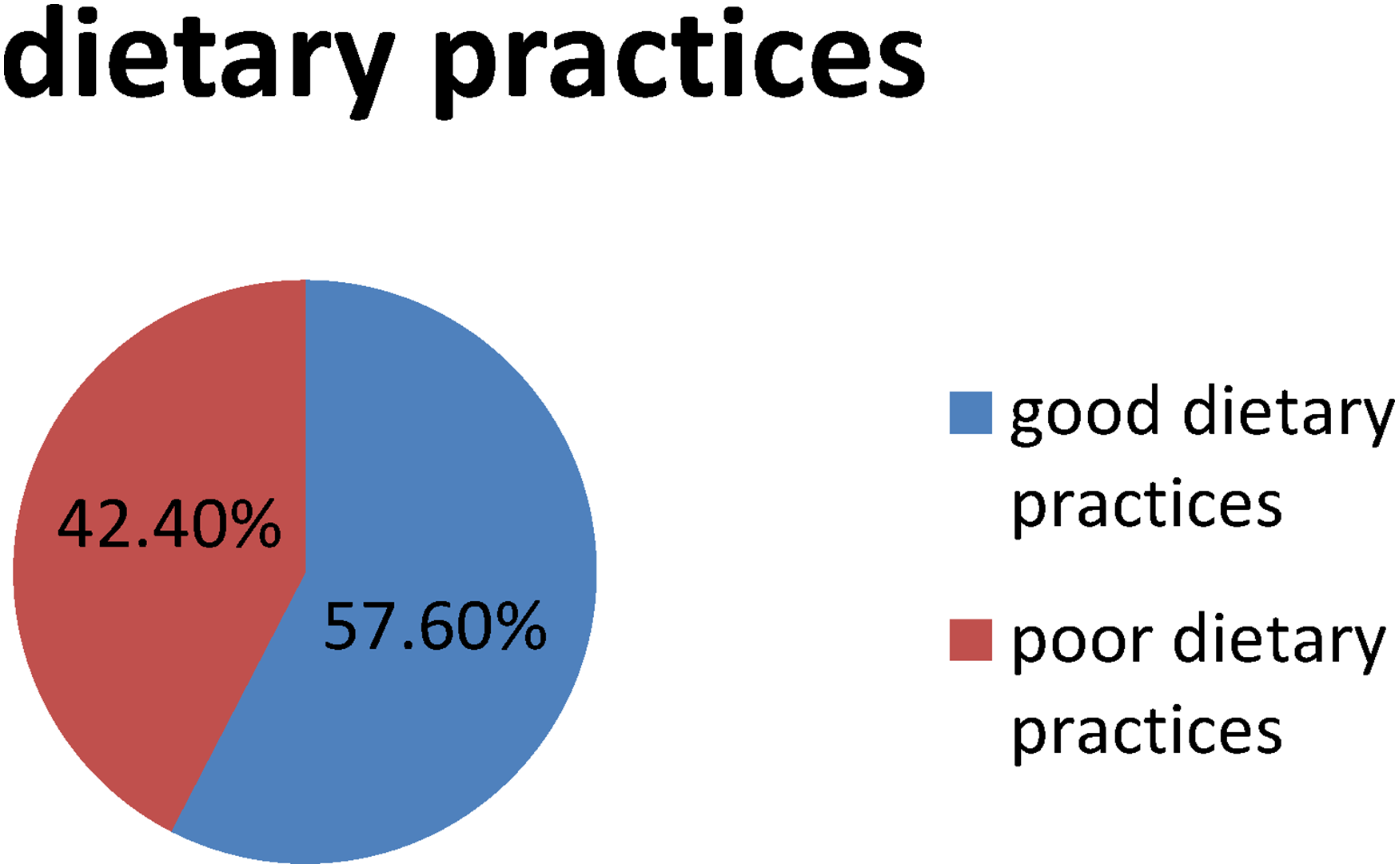
Proportion of dietary practices of adult patients with diabetic mellitus on follow-up.
Factors Associated With the Dietary Practices of Diabetic Patients
Bivariate logistic regression analysis was used to evaluate various independent variables with outcome variables. Thus, marital status, sex, residence, family size, family history of DM, comorbid diseases, and knowledge were significantly associated with the dietary practices of adult diabetic patients at follow-up. Significantly associated with the dietary practices of adult diabetic patients at follow-up were all variables with p-values less than .25 that were fitted into the backward likelihood multivariate logistic regression model.
However, on multivariable analysis, sex, residence, family history of DM, and knowledge were significantly associated with the dietary practices of adult diabetic patients at follow-up. The probability of female patients having good dietary practices was 2.22 times higher than that of male patients (AOR: 2.22, 95% CI 1.283–3.841). Furthermore, the odds of good dietary practices among urban diabetic patients were 3.136 times higher than those of rural areas (AOR: 3.136, 95% CI 1.666–5.904). Additionally, individuals with a family history of diabetes had 3.014 times higher odds of having good dietary practices compared to those without a family history of diabetes (AOR: 3.014, 95% CI 1.654–5.492). Furthermore, diabetic patients with good knowledge had 2.876 times higher odds of having a good diet compared to those with poor knowledge (AOR: 2.876, 95% CI 1.524–5.428) (Table 5).
Bivariate and Multivariate Analysis of the Dietary Practices of Adult Patients With Diabetic Mellitus on Follow-up.

AOR = adjusted odd ratio; COR = crude odd ratio.
* p-value < .05, ** p-value < .025, *** p-value < .0001.
Qualitative Results
Participants’ Characteristics
A total of 16 patients were recruited for the qualitative study. The mean (±SD) age of the participants was 29.185 (±3.67). The participants’ ages ranged from 25 to 67 years. Regarding their working positions, four were government employees, three were merchants, two were housewives, and seven were farmers.
Living as before and not adhering to diabetic dietary recommendations
The majority of participants acknowledged the significance of diet in controlling blood glucose levels. Nearly all participants described their typical meal as consisting of Injera. However, most participants did not recognize diabetic-friendly meal plans. This is evident from the following quotes: I do not want to say on every occasion, ‘I am diabetic, I don’t eat this.’ That is too boring From the day of diagnosis, I have not changed my meals. I eat like everybody else. I don't want to be too picky about my meals. (37 years old male participant 9) What does it matter if I avoid a meal that has sugar? I don't like to stress myself too much about what I eat, drink, and the like. When I am hungry, I eat whatever is in front of me. (42 years old male participant 1) Sugar for diabetic patients? No, we don't do that… Even I forget, my wife reminds me not to touch anything that has sugar. My problem is I don't plan my meals… this time this food and the like. (54 years old male participant 14)
Barriers to adherence to effective diabetic dietary practices
A diverse array of responses emerged concerning obstacles to effective dietary practices adherence.
Societal Pressure
Almost all respondents mentioned that societal pressure during gatherings sometimes affects their dietary practices. In Ethiopia, sharing food during gatherings is considered a way of expressing love.
As one participant expressed, “When I visit family or friends, people share food on a plate and insist that I join and have the food… they will say, ‘Come, have a bite, we will pray. One bite can't kill you.’” (50 years old female participant 16).
Accessibility
Many participants reported living in rural areas, resulting in reduced access to food variety, as illustrated by these quotations: Are you kidding? I am from a rural area. We don't have many options for fruits and vegetables. Even if we have the means and desire to purchase them, we must travel to the market, which occurs just once per week. (67 years old female participant 6)
Lack of Support
Participants highlighted the role of insufficient social support in hindering effective dietary practice adherence, as evidenced by the following statements: You know we are humans, and we require support from our families and communities as well. Sometimes I feel exhausted from my job (which requires a great deal of energy because I am a farmer). When I am hungry, I forget that I am diabetic and consume foods in front of me. We often need support and someone to remind us. (43 years old male participant 15)
Knowledge
Lack of knowledge on dietary self-care practices such as exercise, proper nutrition, and blood glucose monitoring was cited as a barrier to implementing effective dietary practice adherence, as exemplified by these comments: No one has informed me about which foods to eat……This is my fourth year since my diagnosis of diabetes. I didn't realize that fruits and vegetables are important. I thought if I ate fruit, my blood glucose would rise. (50 years old female participant 14)
Moreover, some participants indicated that strict adherence to effective dietary practices might be perceived as monotonous: As you can see, I am young, and I cannot stop everything at this age, especially food and drinks. How can I live without even sipping beer?….. Because I enjoy beer very much. I have continued consuming beer despite my diagnosis, although not excessively. (60 years old male participant 3)
Discussion
This study aimed to investigate the dietary practices and associated factors among adult DM patients at academic tertiary-level hospitals in central Ethiopia. Through this institution-based cross-sectional study, the research delved into assessing and exploring the dietary practices of diabetic patients and the barriers that hinder their adherence to recommended dietary guidelines.
The study revealed that the overall proportion of good dietary practices among diabetic patients was 42.4% [95% CI (37.7, 47.5)]. As the finding indicates good dietary practices was low, this finding was reinforced by an in-depth interview where a participant expressed a tendency to continue living as before without adhering to diabetic dietary recommendations. While the majority of participants recognized the importance of diet in managing blood glucose levels, many described their typical meals as centered on Injera. Surprisingly, most participants did not identify diabetic-friendly meal plans as part of their dietary choices. The study revealed that the overall proportion of good dietary practice among diabetic patients was 42.4% [95% CI (37.7, 47.5)]. This finding is consistent with the findings from Gonder (46.7%) (Belay et al., 2021). However, this finding is lower than studies conducted in other parts of Ethiopia: Addis Ababa (48.6%) (Worku et al., 2015), Hawassa (55.8%) (Desta et al., 2021), and Nigeria (76%) (Isara et al., 2014). Differences in findings could be due to differences in the study setting, sample size, and socioeconomic status of participants. The other possible explanation could be the tool used to asses (measure outcome).
The proportion of good dietary practices among diabetic patients in this study is higher than the studies from central Ethiopia (35.6%) (Tirfessa et al., 2023), Bahir Dar (35.9%) (Demilew et al., 2018b), and Dire Dawa, Ethiopia found a 53.8% prevalence of poor dietary practices (Gebeyehu et al., 2022). The possible explanation for the variation could be due to differences in socioeconomic status of participants, study setting, and level of awareness.
The likelihood of female patients having a good dietary practices was 2.22 times higher than that of male patients. The finding is consistent with studies from central Ethiopia (Tirfessa et al., 2023), south-west Ethiopia (Zeleke Negera & Charles Epiphanio), India (Klinovszky et al., 2019), and Yemen (Alhariri et al., 2017). One possible explanation for this finding is that women may be more receptive to changing their dietary habits than men. Additionally, as cooking is typically a task performed by women in Ethiopia, they may have more opportunities to prepare food per dietary recommendations for their health condition. This may contribute to the higher likelihood of good dietary practices among female patients compared to male patients. Contrasting these results, previous research conducted in Nepal (Parajuli et al., 2014) lower likelihood of good dietary practice among males than females.
The odds of good dietary practices among urban diabetic patients were 3.136 times higher than those in rural areas. This finding is consistent with studies from Bahir Dar (Belay et al., 2021), Tigray Ethiopia (Molalign Takele et al., 2021), Yemen (Alhariri et al., 2017), and Gambella (Teklemariam et al., 2022). One possible explanation for this could be that diabetic patients living in urban areas have easier access to a variety of food and information, which may enhance their ability to practice dietary self-care management for diabetes (Gebremichael, 2017). This advantage in access to food and information is supported by in-depth interviews, as most participants explained that they reside in rural areas, where they have limited access to a variety of food. This disparity in access to food resources between urban and rural areas may significantly impact the dietary choices and self-care practices of individuals living with diabetes.
Individuals with a family history of diabetes had 3.014 times higher odds of having good dietary practices compared to those without a family history of diabetes. This finding is consistent with previous studies conducted in Dire Dawa (Getie et al., 2020) and western India (Patel et al., 2012). One possible explanation for the association between family history and good dietary practices among diabetic patients is that individuals with a family history of diabetes may have a better understanding of dietary recommendations due to the availability of information from their family members who have experienced the condition. This may contribute to their increased likelihood of adhering to beneficial dietary practices. The finding was further reinforced by in-depth interviews, revealing that social support and societal pressure posed barriers to adhering to an effective diabetic diet. Nearly all respondents noted that societal pressure during gatherings could impact their dietary choices. In Ethiopia, the act of sharing food during social gatherings is a cultural expression of love. Participants emphasized the impact of inadequate social support on impeding adherence to effective dietary practices, as illustrated by the following statements.
Diabetic patients with good knowledge had 2.876 times higher odds of having good dietary practices compared to those with poor knowledge. This finding is consistent with studies from central Ethiopia (Tirfessa et al., 2023), Addis Ababa (Tewahido & Berhane, 2017), Bahir Dar (Demilew et al., 2018a), Arba Minch (Worsa et al., 2021), Dire Dawa (Getie et al., 2020), Kenya (Wahome et al., 2018). A possible explanation for this could be knowledge of diabetic patients about diabetes self-care practices increase dietary practice which is one of the components of diabetic self-care practice.
Good dietary practice is the pillar for diabetes self-management, and poor dietary practices are associated with poor knowledge about diabetes and vice versa (Parajuli et al., 2014). This was further corroborated by in-depth interviews, as some participants expressed their challenges in adhering to effective dietary practices due to a lack of awareness about dietary self-care, including exercise, diet, foot care, and blood glucose monitoring. Additionally, some participants described their difficulty in adhering to effective dietary practices due to the perceived monotony of strict adherence. These insights highlight the need for tailored education and support to address knowledge gaps and perceptions that hinder adherence to beneficial dietary practices among individuals with diabetes.
Conclusion and Recommendations
This study unveiled that less than half of DM patients exhibited good eating practices. Factors such as sex, place of residence, family history of diabetes, and level of dietary knowledge showed significant associations with dietary practices. Through qualitative analysis, notable barriers hindering compliance with beneficial dietary regimens were identified, including societal pressure, accessibility to foods, lack of support, and lack of knowledge. Our recommendations include advising patients to adhere to dietary recommendations, with a specific emphasis on male patients paying close attention to diabetic diets. Health professionals and healthcare facilities are encouraged to provide tailored health education based on geographic locations and involve the families of diabetic patients in these educational efforts. Lastly, families and communities should offer support to diabetic patients in managing their diets effectively.
Strengths and Limitations
Strength
The study used a mixed convergence method in which quantitative and qualitative data were collected and analyzed, and then the analyzed data were compared to see if the data confirmed or disproved each other.
Limitation
Qualitative data were collected through interviews, so the response to the practice may be inflated due to the social desirability bias of the respondents.
This study may not show the temporal relationship between factors and dietary practice because it is a cross-sectional study.
Supplemental Material
sj-docx-1-son-10.1177_23779608241279151 - Supplemental material for Dietary Practices and Associated Factors Among Adult Diabetic Patients at Academic Tertiary-Level Hospitals in Central Ethiopia: Convergent Mixed Study
Supplemental material, sj-docx-1-son-10.1177_23779608241279151 for Dietary Practices and Associated Factors Among Adult Diabetic Patients at Academic Tertiary-Level Hospitals in Central Ethiopia: Convergent Mixed Study by Sentayehu Admasu Saliya, Taye Mezgebu Ashine, Asnakech Zekiwos Heliso, Getachew Ossabo Babore, Bethelhem Birhanu, Awoke Girma Hailu, Sisay Foga Sebro, Elias Ezo and Selamawit Wondale Begizew in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608241279151 - Supplemental material for Dietary Practices and Associated Factors Among Adult Diabetic Patients at Academic Tertiary-Level Hospitals in Central Ethiopia: Convergent Mixed Study
Supplemental material, sj-docx-2-son-10.1177_23779608241279151 for Dietary Practices and Associated Factors Among Adult Diabetic Patients at Academic Tertiary-Level Hospitals in Central Ethiopia: Convergent Mixed Study by Sentayehu Admasu Saliya, Taye Mezgebu Ashine, Asnakech Zekiwos Heliso, Getachew Ossabo Babore, Bethelhem Birhanu, Awoke Girma Hailu, Sisay Foga Sebro, Elias Ezo and Selamawit Wondale Begizew in SAGE Open Nursing
Footnotes
Abbreviations
Acknowledgments
We would like to thank the supervisors, data collectors, and our study participants for their prized input. We also would like to give our greatest thanks to Wachemo University, College of Medicine and Health Science, School of Nursing, for providing an opportunity to carry out this study.
Author Contributions
Conceptualization: Sentayehu Admasu Saliya. Data curation: Sentayehu Admasu Saliya and Taye Mezgebu Ashine. Formal analysis: Sentayehu Admasu Saliya, Taye Mezgebu Ashine, and Asnakech Zekiwos Heliso. Funding acquisition: Getachew Ossabo Babore, Bethelhem Birhanu, Awoke Girma Hailu, Investigation: Sentayehu Admasu Saliya. Methodology: Sentayehu Admasu Saliya, Taye Mezgebu Ashine, Asnakech Zekiwos Heliso, Getachew Ossabo Babore, Bethelhem Birhanu, Awoke Girma Hailu, Sisay Foga Sebro, Elias Ezo, Selamawit Wondale Begizew. Validation: Sentayehu Admasu Saliya, Taye Mezgebu Ashine, Asnakech Zekiwos Heliso, Getachew Ossabo Babore, Bethelhem Birhanu, Awoke Girma Hailu, Sisay Foga Sebro, Elias Ezo, Selamawit Wondale Begizew. Visualization: Sentayehu Admasu Saliya, Taye Mezgebu Ashine, Asnakech Zekiwos Heliso, Getachew Ossabo Babore, Bethelhem Birhanu, Awoke Girma Hailu, Sisay Foga Sebro, Elias Ezo, Selamawit Wondale Begizew. Writing—original draft: Sentayehu Admasu Saliya. Writing—review & editing: Sentayehu Admasu Saliya, Taye Mezgebu Ashine, Asnakech Zekiwos Heliso, Getachew Ossabo Babore, Bethelhem Birhanu, Awoke Girma Hailu, Sisay Foga Sebro, Elias Ezo, Selamawit Wondale Begizew.
Availability of Data and Materials
The dataset used and analyzed during the current study will be available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Consideration and Consent to Participate
Ethical clearance was obtained from the Wachemo University College of Medicine and Health Sciences with reference number IRB/172/16. An official support letter was obtained from WCUNEMMCSH. Verbal informed consent was obtained from all randomly selected study participants for their voluntary participation in the study. A detail explanation about the purpose of the study, data confidentiality, and benefits of the study. No personal identification of participants was recorded to ensure confidentiality. Verbal informed consent was obtained from study participants as approved by Wachemo University Institutional Review Board (IRB) of the College of Medicine and Health Science. All study participants were received information on the study objectives and recruitment process. To protect participants from risks, the study did not record participants’ names, identification numbers and names of health facilities where he or she worked. Data were also entered in a computer with unique random generated ID numbers given for each study participant. All methods were carried out in accordance with relevant guidelines and regulations.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Implication for Nursing Practices
Nurses can bridge the gap by reflecting on their practices, seeking continuous learning in research and implementation, collaborating with peers and advocating for change, and prioritizing patient-centered care through evidence-based interventions. This ongoing journey, supported by research participation and scholarship, empowers nurses to be champions of optimal healthcare for all.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.