
Abstract
Background
Neonatal near-miss refers to conditions in which a newborn is on the verge of dying, but survived within 28 days of life. Although the study of neonatal near miss has emerged in many countries, there is limited data about the condition in Garowe, Somalia. Hence, the study aimed to assess the magnitude of neonatal near miss and its associated factors among neonates in Garowe City, Puntland.
Methods
Institution based cross-sectional study was conducted from June 01–29 2024 among randomly selected 375 neonates. Data were collected by trained nurses through face-to-face interview of the mothers or guardians using a pre-tested standard questionnaire. Neonatal near miss was defined as having any of the pragmatic (birth weight <1750g, <33 weeks gestational age,or <5 fifth minute APGAR score) or management criteria (mechanical ventillation, cardiopulmonary resuscitation, nasal continous positive airway pressure, parentral antiobiotics, parentral nutrition, use of vasoactive drugs, or phototherapy within 24 hours of birth). Data were entered into Epidata version 3.1 and exported to Stata version 14.0 for analysis. Bivariable and multivariable logistic regression were done to identify factors associated with neonatal near miss. Level of statistical significance was declared at p-value < 0.05.
Results
The magnitude of neonatal near miss was found to be 48.2% (95% CI: 43%, 53%). Neonates born from daily laborer mothers (AOR = 5.72; 95% CI: 1.73-18.89), from women with history of abortion (AOR = 2.75; 95% CI: 1.37-5.53), and those admitted to the neonatal intensive care unit (AOR = 13.99; 95% CI: 7.36-26.59) were more likely to have neonatal near miss.
Conclusion
Nearly half of neonates in Garowe experienced a near miss event. Maternal occupation, history of abortion, and admission to neonatal intensive care unit were found to be key associated factors. Health care professionals should enhance early identification and follow-up of high-risk pregnancies and newborns, particularly in mothers with a history of abortion or those engaged in physically demanding jobs.
Introduction
Globally, 2.5 million babies died within a month of life, with approximately 2 million of these deaths occurring during the first week of life (WHO, 2018). Though, the numbers of mortality show a huge improvement , up to eight newborns for each death survive with life-threatening complications (Lawn et al., 2013). These events are known as neonatal near-misses (NNM) and are crucial indicators for epidemiologic surveillance as well as the evaluation of healthcare quality (Bakari et al., 2019). Wardlaw et al., 2014
The main causes of neonatal death worldwide are complications arising from preterm birth, asphyxia during labor and sepsis, accounting to 75% of the deaths (WHO, 2023). Internationally, complications arising from preterm birth alone contribute to approximately 35% of neonatal deaths, while birth asphyxia accounts for about 24%; Furthermore, an estimated 14% of newborns are delivered with low birth weight (LBW), with the highest prevalence observed in Asian and African countries (Mengesha & Sahle, 2017; WHO, 2018). These conditions negatively impact childhood growth and development with an increased risk of chronic diseases later in life (Lawn et al., 2013; Bugelli et al., 2021). As a result, they impose social, emotional, and economic burdens on families and communities (Santos et al., 2015). The magnitude of NNM varies widely across studies, primarily due to differences in the criteria used for its identification. Studies that relied solely on pragmatic criteria reported an incidence ranging from 21.4 per 1,000 live births in Brazil (De Lima et al., 2018) to 86.7 per 1,000 live births in Portugal (Da Costa et al., 2022).
Scholars indicate that, the number of newborn babies surviving as NNM event were approximately three to six times higher than the number of newborn babies who died (Haile et al., 2023). In Portugal, the estimated number of survivors as of NNM cases were seven times higher than the number of newborn deaths (Da Costa et al., 2022). Similarly, in Uganda, the NNM rate was estimated to be double than the neonatal mortality rate (Nakimuli et al., 2015). Infants with severe complications can also develop long-term illnesses due to neurological and cognitive effects with a possibility of later life complications such as diabetes, cardiovascular disease, and chronic lung disease, as well as other serious disabilities including blindness or vision problems and hearing loss (Wondimu et al., 2021). The majority of neonatal deaths are preventable, and substantial reductions can be achieved through improving maternal and newborn care (WHO, 2023). Severe infections, low birth weight, and birth asphyxia are among the most common causes of NNM reported in health facilities (WHO, 2018).
In South Central Asia and sub-Saharan Africa, neonatal morbidity and mortality remains high despite reduction of post neonatal mortality (Mengesha et al., 2020;Haile et al., 2023). Similarly, in Ethiopia, complications of preterm birth (22%), intrapartum-related events (32%), infections (20%), and congenital abnormalities (12%) were the leading causes of neonatal mortality (Tekola et al., 2021; Asaye et al., 2023).
Review of the Literature
A hospital-based cross-sectional study in Nepal, involving 1000 mother-newborn pairs revealed a NNM rate of 79 per 1,000 live births (Sushma et al., 2021). An observational study in Morocco among 2,676 neonates revealed that, 88.5% (95% CI: 88.3–90.7) of them had NNM (Chafik, et al., 2023). Asystematic review and meta-analysis by (Deressa & Desta, 2023) found a pooled NNM prevalence of 35.51% (95% CI: 20.32–50.70). Quantitative, facility-based cross-sectional study among 403 neonates admitted to NICU were reported that, just about half (196 (48.6%), 95% CI = (43.79%, 53.5%)) were diagnosed as having NNM using the pragmatic and management criteria (Gutema et al., 2022).
A retrospective cross-sectional study at Debre Tabor General Hospital Ethiopia found a prevalence of 32.2% (95% CI: 28–36) (Tassew et al., 2020). While a similar study in North Shewa zone reported 35.3% (95% CI: 31.9–38.6) per 1,000 live births (Goyomsa et al., 2022). In Addis Ababa, a study across four hospitals showed a prevalence of 25.6% (95% CI: 21.0–30.5) (Legamo & Sendo, 2023). In Jimma Zone, Southwest Ethiopia, two different studies have been reported related findings where, a NNM prevalence was 26.7% (95% CI: 21.6–32.5 (Wondimu et al., 2021). In a study at Injibara General Hospital, Amhara Region, reported a magnitude of 23.3% (95% CI: 19.1–27.7) (Gebrehana Belay et al., 2020). A prospective study in South Ethiopia among 2,704 neonates showed a NNM rate of 45.1 per 1,000 live births (95% CI: 37.7–53.8) (Tekelab et al., 2020). Another study in Adare General Hospital and Hawassa University hospitals reported an overall magnitude of 33.4% (95% CI: 29.7–37.1%) among 604 live births (Tekola et al., 2021). Another research carried out in the East Gojjam zone, in Amhara Region, Ethiopia showed that, the prevalence of NNM was found to be 41.3% (95% CI: 37.1%, 45.3%). (Tesfa et al., 2025).
Many quantitative studies also pointed out that, parental sociodemographic factors (advanced maternal age, residence, paternal and maternal education, maternal and paternal occupation) ; Obstetrics and medical-related factors (history of abortion, maternal medical comorbidity); Fetal-related factors (time of breast feeding initiation, APGAR score) and health system related factors were collectively a significant risk factor for adverse neonatal outcomes, including NNM (Martinelli et al., 2019; Tesfa et al., 2025; Sintayehu et al., 2022; Goyomsa et al., 2022; Endawkie et al., 2023; Fikrie et al., 2022; Asaye et al., 2023;Ahmed & Salih, 2019; Gebrehana Belay et al., 2020).
Although various studies quantify the magnitude of NNM and identify corresponding factors, regional variation and low implementation practice of health policy including differences in socio economic development can create room for regionally specific clinical audit in Puntland, Somalia to determine and identify modifiable risk factors and inform targeted neonatal care improvement.
Methods and Materials
Study Setting and Period
This study was conducted in Garowe City, Puntland, which is located in the northeastern region of Somalia. Garowe is the capital city of the Puntland state and the second largest city of Somalia situated in Nugal with an estimated population of 40,000 to 70.000 (UN habitat 2005). Garowe city has one public governmental hospital, and two private hospitals. These hospitals had major clinical departments like surgery, pediatrics, obstetrics and gynecology, and others. Around 400–550 neonates are born in the selected health institutions per month. The study was conducted from June 1 to 29, 2024.
Study Design and Population
An institutional based cross-sectional study design was conducted. All live-born neonates born in the selected facilities and their mothers or guardians were included in the study. However, neonates who were discharged against medical advice or died were excluded.
Sample Size Determination and Sampling Technique
The sample size was determined using a single proportion formula: n = (Z a/2)2 P (1 − P)/W2 where n = total sample size, Z = confidence interval (with 95% level of certainty), w = margin of error (5%), and p = proportion of live born neonates surviving from life-threatening conditions or using the magnitude of NNM from the previous study North Shewa zone public hospital Ethiopia was 35.3% (Goyomsa et al., 2022). Thus, n = (1.96)2 × 0.353 × 0.647/ (0.05)2 = 351. By adding 10% of the nonresponse rate, the final sample size is 386.
All three hospitals in the city were included. The calculated sample size was proportionally allocated for each hospital based on information from the hospitals, an average number of neonates delivered at selected health institutions per month were around 550 and the sampling interval was determined with K = N/n; K average = 550 / 386 = 1.42 = 2; the first neonate was selected by lottery method and then, the data were collected using a systematic sampling technique for every value of two (Figure 1).

Schematic presentation of sampling procedure to assess neonatal near miss and its associated factors among neonates delivered in Garowe city health facility, Puntland, Somalia, 2024.
Data Collection Procedures
Data were collected by trained interviewer's face-to-face (seven trained BSc nurses) with the supervision of three pediatricians using a structured questionnaire and review medical chart at discharge. The questionnaire was first prepared in English and translated to the local language (Af-Somali) and was translated back to English to check its consistency. The questionnaire contains information on socio-demographic characteristics, obstetric factors, institutional health related factors and fetal health related problems.
Operational Definition
NNM refers to a newborn who experiences a severe, life-threatening complication during the neonatal period but survives the event with the following clear criteria (Rocha et al., 2023); (Santos et al., 2015); Pragmatic Criteria refers birth weight < 1750 g, gestational age < 33 weeks 5th-minute APGAR score < 7 at 5 min (Tesfa et al., 2025), (Pileggi-Castro et al., 2014).;Management Criteria refers mechanical ventilation, cardiopulmonary resuscitation, nasal continuous positive airway pressure, parenteral antibiotics, parenteral nutrition, vasoactive drugs, use of phototherapy within 24 h of life (Tesfa et al., 2025); (Gutema et al., 2022); Clinical Criteria encompass observable signs and symptoms indicating severe neonatal complications, these include: Hypothermia (< 36.50 °C), absence of regular breathing, cardiac arrest, respiratory rate > 70 bpm, bradycardia < 80 bpm, jaundice during the first 24 h (Tesfa et al., 2025; Kale et al., 2017).
Data Quality Control
Data collectors and supervisors were trained on the objective of the study, contents of the questionnaires and how to maintain confidentiality and privacy of the study subjects. The questionnaire was pre-tested on 5% (20) for three days of sampled population in Gol-nugal hospitals and checked for any amendments to be made. The overall data collection process was strictly supervised in each step. The questionnaire was translated to the local language and back translated by individuals with good command of both languages.
Data Analysis
The data were first checked for completeness and internal consistency through cross-checking before being coded and double-entered into Epidata version 3.1. After cleaning for inconsistencies, the dataset was exported to STATA version 14 for statistical analysis. Bivariable logistic regression was performed to examine the crude association between NNM and each independent variable; then, variables with a p-value less than 0.25 in the bivariable analysis were considered as candidates for multivariable logistic regression. Multicollinearity among independent variables was assessed using the variance inflation factor (VIF), and potential interaction effects between variables were examined. The overall model fitness was evaluated using the Hosmer–Lemeshow goodness-of-fit test. Multivariable logistic regression was then conducted to control for possible confounders, and the results were presented using adjusted odds ratios (AOR) with corresponding 95% confidence intervals (CI). Finally, statistical significance was declared at a p-value <0.05.
Results
Socio-Demographic and Child Related Characteristics
A total 375 (97%) of the 386 mother-baby dyads invited participated in the study. The mean maternal age was 28.52 (±SD 7.21) years, with the majority being 20–34 years old (245; 65.33%). In terms of educational status, 72 (19.20%) of the mothers were unable to read and write. Fathers’ educational background showed that, 64 (17.98%) were unable to read and write. In terms of maternal occupation, the majority 219 (58.40%) were housewives. A substantial proportion of the participants 317 (84.53%) resided in urban areas. Most mothers 343 (91.47%) accessed the health facility through self-referral. Among those who were referred, the most common reason was prolonged labor 11 (34.38%). With regard to family income, 93 respondents (24.80%) reported earning less than $100 per month (Table 1).
Sociodemographic Characteristics of Mothers of Neonates among Neonates in Garowe City, Puntland, Somalia (n = 375).

Maternal Medical and Obstetrics Conditions
Among 375 mothers included in the study, the majority 288 (76.80%) were multigravida. Regarding parity, 157 (41.87%) had given birth to more than one child. A history of stillbirth was reported by 86 participants (22.93%), while 94 (25.07%) had experienced at least one abortion. Additionally, 88 mothers (23.47%) reported a previous neonatal loss. Concerning birth spacing, 144 (38.40%) had a birth interval of less than 24 months. The majority of mothers 295 (78.67%) reported attending at least one ANC visit. In terms of mode of delivery, 234 (62.40%) had spontaneous vaginal deliveries. A high proportion of participants 222 (59.20%) reported experiencing an infection during pregnancy, of whom 207 (93.24%) received treatment (Table 2).
Maternal Medical and Obstetrics Conditions among Neonates in Garowe City, Puntland, Somalia (n = 375).

NB. ### Cervical lesion, and coagulation disorder.
Neonatal Characteristics
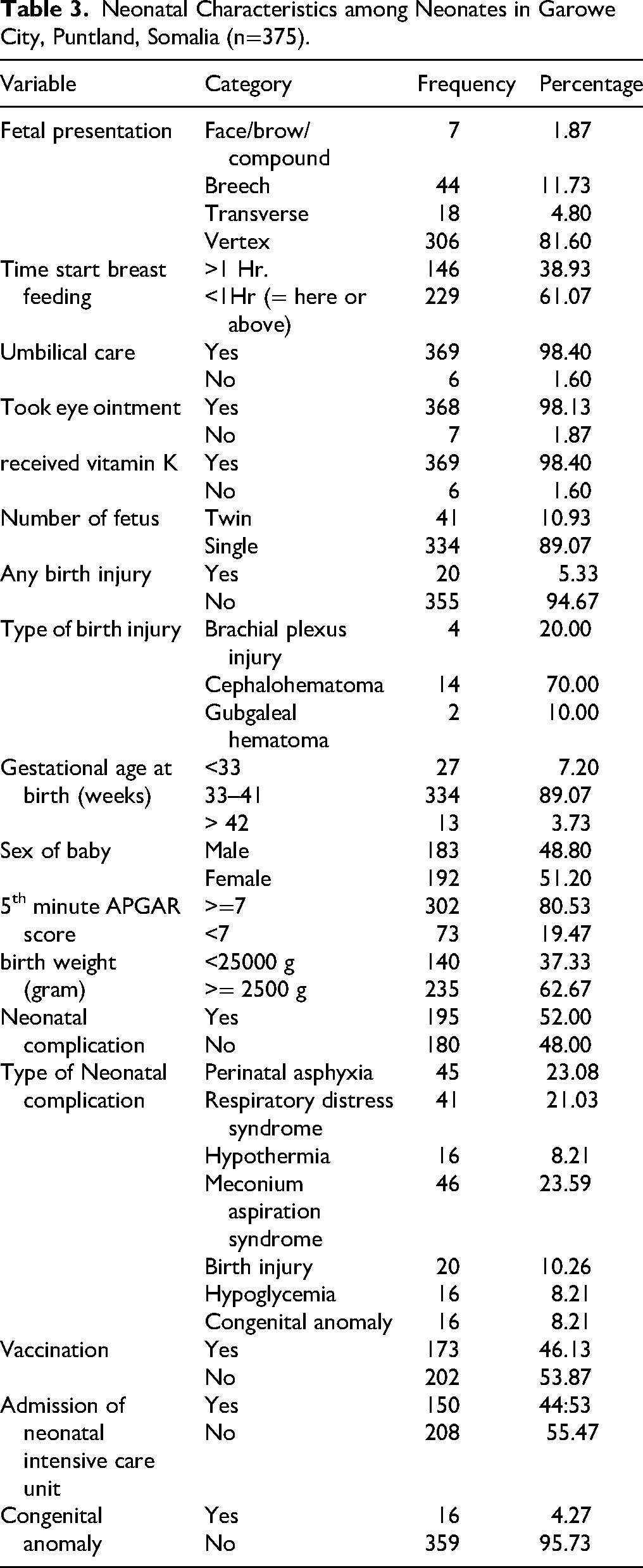
The majority of neonates were vertex presentation (81.60%). Regarding gestational age, the majority (89.07%) were born between 33 and 41 weeks of gestation. At the fifth minute of life, 80.53% of the neonates had an Apgar score of ≥7 (Table 3).
Neonatal Characteristics among Neonates in Garowe City, Puntland, Somalia (n=375).
Neonatal Near Miss Events
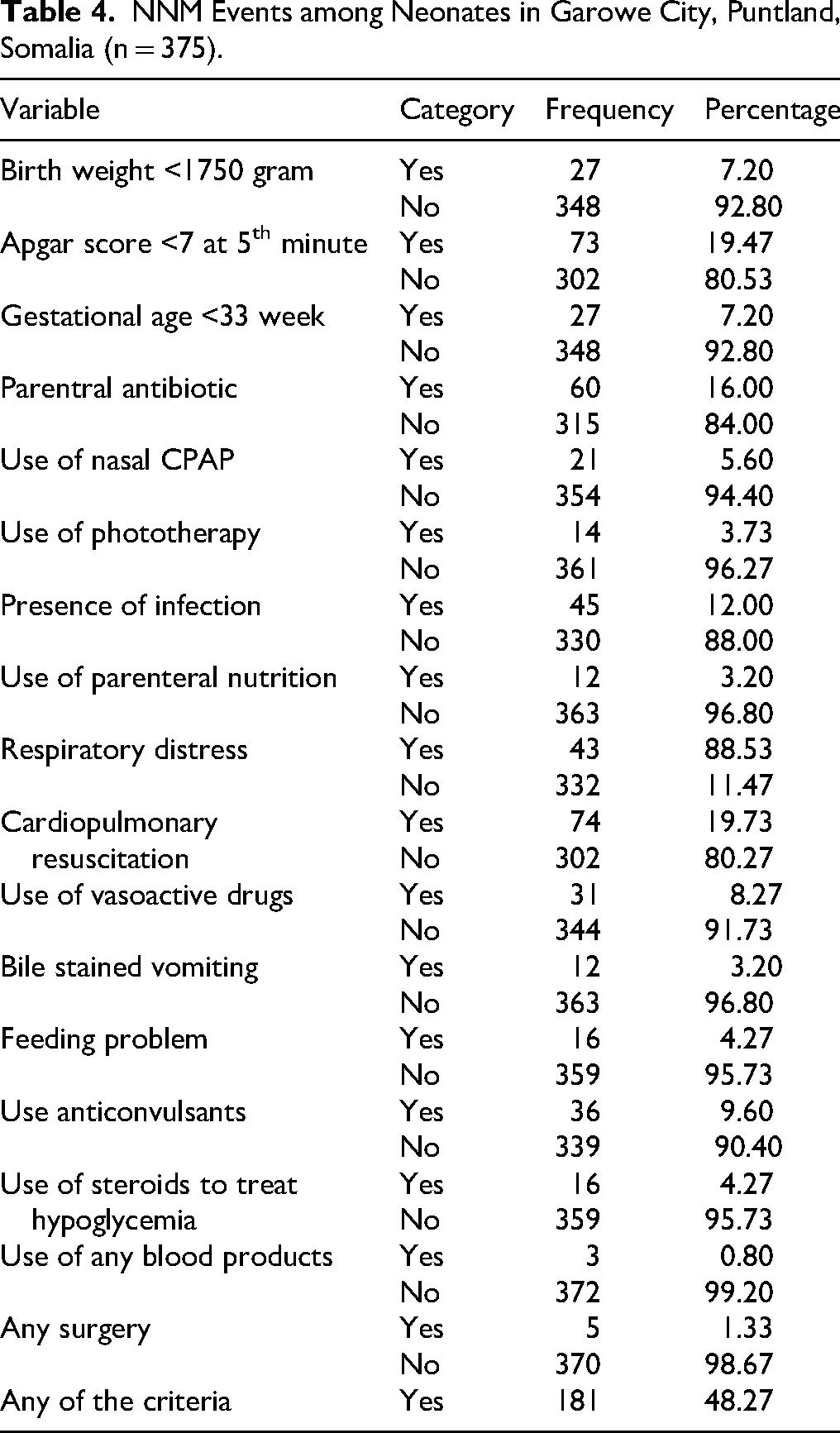
Of 375 neonates, 181 (48.27%) had at least one of the pragmatic or management criteria corresponding with a NNM of 482 per 1000 births. The most frequent NNM events were cardiopulmonary resuscitation 74(19.73%) followed by low 5th minute Apgar score 73(19.47%) and parentral antibiotic uses 60(16.00%). A small proportion of neonates 27 (7.20%) had extream low birth weight, which is less than 1750 grams (Table 4).
NNM Events among Neonates in Garowe City, Puntland, Somalia (n = 375).
Factors Associated with Neonatal Near Miss
In bivariable analysis; mother and father occupation, resident area, mother referral status, monthly family income, history of abortion, mode of delivery, hypertensive disorder during pregnancy, anemia, infection, mother referral status, delivered time, time start to breast feeding, admission to NICU, congenital anomaly and vaccination were associated at p-value <0.25 and considered for multivariable analysis to control for potential confounders. In multivariable analysis, maternal occupation, history of abortion, and neonate admission to NICU remained statistically significant at a p-value <0.05 (Table 5).
Factors Associated with NNM among Neonates born in Garowe City, Puntland, Somalia (n = 375) 2024.
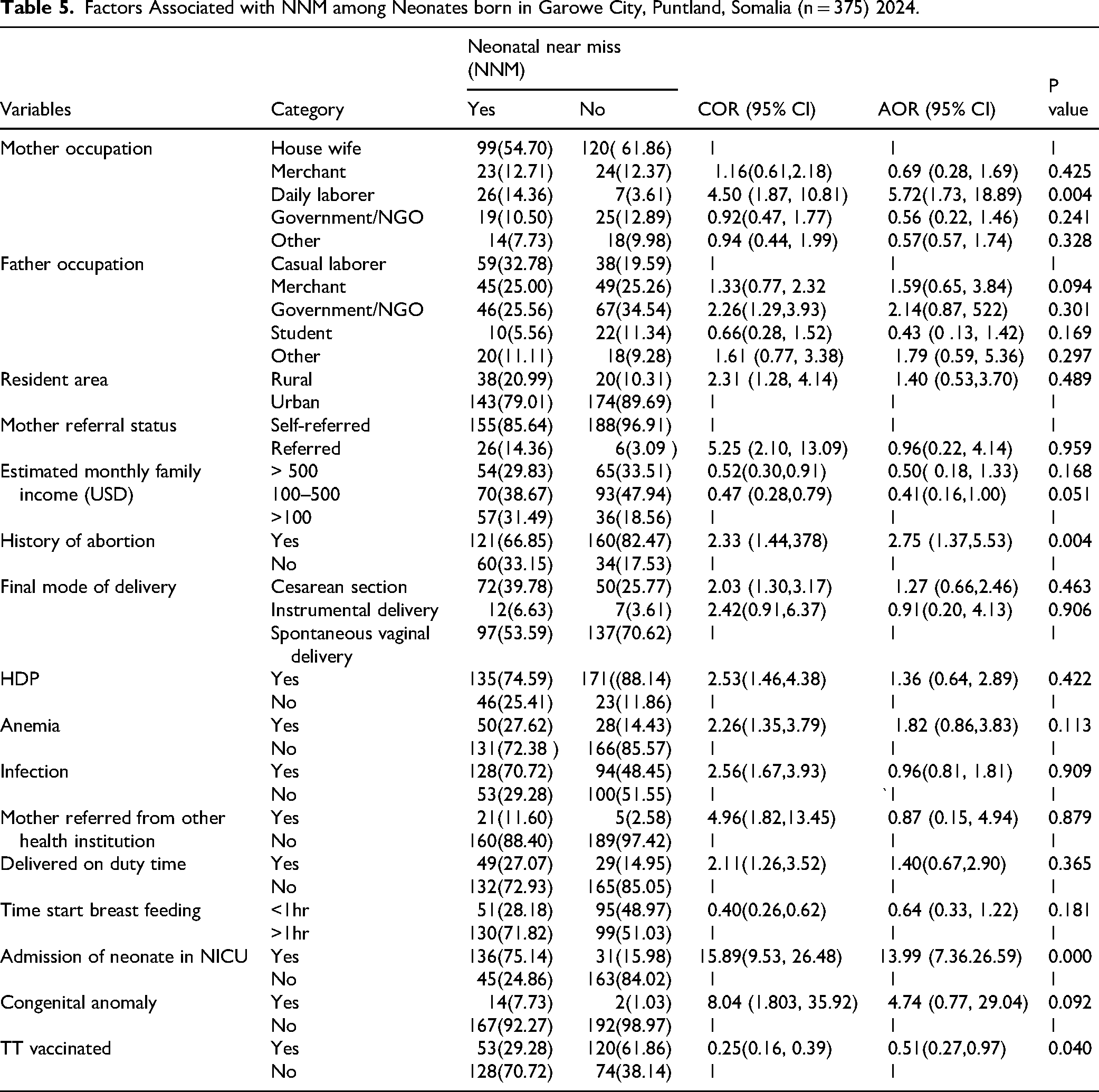
Neonates born to mothers who were daily laborers were about six times (AOR = 5.72; 95% CI: 1.73-18.89) more likely to have NNM compared to those born to housewives. Mothers with a history of abortion were nearly three times (AOR = 2.75; 95% CI: 1.37-5.53) more likely to have a neonate with NNM compared to those without such history. Similarly, neonates admitted to NICU were about fourteen times (AOR = 13.99; 95% CI: 7.36-26.59) more likely to have NNM compared to neonates who were not admitted to NICU (Table 5).
Discussion
This study assessed the magnitude of NNM and its associated factors among neonates in Garowe, Puntland, Somalia. The overall NNM rate was found to be 48.2% (95% CI: 43–53%). Factors such as maternal occupation, history of abortion, and admission to the NICU were significantly associated with NNM.
The magnitude of NNM observed in this study is comparable to findings from East Wollega Zone, Ethiopia (48.6%) (Gutema et al., 2022) and Southern Ethiopia (45.1%) (Tekelab et al., 2020). However, it is higher than the reports from Addis Ababa, Ethiopia (25.6%) (Legamo & Sendo, 2023), Harari Region, Ethiopia (31.4%), East Gojjam, Ethiopia (41.3%) (Tesfa et al., 2025), Uganda (34.1%) (Nakimuli et al., 2015), and Northeastern Brazil (22%) (De Lima et al., 2018), yet lower than other findings from Ghana (70%) (Bakari et al., 2019) and Morocco (88.5%) (Chafik, et al., 2023). These differences may be due to variations in maternal healthcare services access, quality of neonatal services, study settings, and sociodemographic factors.
In this study, maternal occupation was significantly associated with NNM; neonates born to mothers who are daily laborers had 5.7 times higher odds of experiencing NNM compared to those born to unemployed mothers. Similar findings were reported in Dessie Comprehensive Specialized Hospital, Ethiopia (Endawkie et al., 2023) and Hawassa City Governmental Hospitals, Ethiopia (Yeshaneh et al., 2021), where, mothers engaged in labor-intensive or informal jobs faced higher risks. The increased risk could be due to work-related stress, poor nutrition, and limited access to healthcare (Sintayehu et al., 2022).
Moreover, a maternal history of abortion was found to increase the risk of NNM. Neonates born from mothers with abortion history had 2.75 higher odds of developing NNM conditions compared to those without. This aligns with the findings reported from the study conducted in Guji and Borona Zones (Fikrie et al., 2022) and North Shewa Zone (Goyomsa et al., 2022) where, prior abortion raised the risk of NNM. The reason might be due to the direct effect of maternal morbidities such as pain, bleeding, uterine perforation, gastrointestinal and thermoregulatory side effects on the unborn fetus and maternal inability to provide appropriate care for the newborn due to maternal medical conditions (Abebe et al., 2021).
Finally, neonates admitted to NICU had approximately 14 times greater odds of being classified as a NNM compared to those not admitted. This was similar with a study findings from Portugal where, NICU admission reflected severe neonatal illness and higher odds of NNM events (Da Costa et al., 2022). Highlighting that, admission to NICU is a robust indicator of severe neonatal illness and potentially leading to NNM events (Carvalho et al., 2020).
Implication for Practice
This study suggests useful insights for clinical care, health care management, and further research in the areas of NNM management and neonatal care specialization. Clinically, healthcare workers can identify prognostic factors associated with NNM among neonates and implement appropriate interventions; specifically, nurses become better equipped to recognize early warning signs and prioritize high risk neonates for immediate care. They can also create structured follow up plans and educate mothers on danger signs even after discharge. Moreover, nurses can adopt evidence based practices and refine care plan based on real outcomes. Healthcare managers can use this evidence to assess and improve the quality of care provided by clinicians. The finding can provide strong evidence for improving referral pathways, upgrading neonatal units, training program for nurses/midwives and proper resource allocation to the highest risk areas. Researchers can also be encouraged to conduct further advanced research on this critical issue to develop effective strategies to reduce neonatal mortality and mortality in all health care system of the country.
In general, this study finding can improve the quality, readiness and responsiveness of neonatal care. It helps identify gaps before they result in death and support evidence based strategies to strengthen neonatal survival.
Strengths and Limitations of the Study
The strength of this study is the combined use of face-to-face interviews and medical record reviews, which enabled comprehensive collection of sociodemographic and obstetric data. However, the cross-sectional design limits the ability to establish causal relationships, as it does not clarify whether the identified factors occurred before or contributed to the NNM events. Follow up was limited to discharge from respective facilities or 28 days of duration, whichever occurred first. Consequently, neonates who were discharged but subsequently develop NNM within the neonatal period may not have been captured unless they were re-admitted to the participating facility.
Conclusions
Nearly half of neonates born in Garowe experienced a NNM event. Maternal occupation, history of abortion, and admission to NICU were key factors associated with the increased occurrence of NNM. Implementing effective strategies using targeted therapeutic interventions to have healthy neonatal outcomes by enhancing continuum of maternal health care services in all level of health care system is vital. Moreover, attention to mothers having history of abortion in line with her occupation is warranted; additionally, all neonates admitted to NICU need to get great emphasis so as to minimize possible NNM.
Footnotes
Acknowledgments
We thank Haramaya University for its technical support. We would also like to extend our gratitude to the head and staff working at Puntland Garowe City health care institution, data collectors, and supervisors for their collaboration.
Ethical Approval and Consent to Participate
Before starting the data collection process, the study protocol was approved by Haramaya University, College of Health and Medical Sciences, Institution Health Research Ethical Review Committee (Ref. No. IHRERC/015/2024). Moreover, an official letter of cooperation was submitted to the selected health institution's head to obtain cooperation and consent to facilitate the study. Voluntary, informed, written, and signed consent was obtained from all study participants/subjects and/or their legal guardians. This study had no danger or negative consequences for the study participants. Confidentiality of information was assured by excluding names and identifiers in the questionnaire. Access to collected information was limited to the principal investigator, and confidentiality was preserved throughout the time. This study was conducted according to the guidelines and regulations of the Declaration of Helsinki.
Author Contribution Statements
MMH made a substantial contribution from conception to data acquisition. All the authors made significant contributions to the study design, analysis, and interpretation of the findings. FM drafted the manuscript. All authors have carefully revised the manuscript. All authors have read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data will be available from the corresponding author upon reasonable request.