
Abstract
Background
Antenatal care (ANC) is a healthcare service designed to ensure a safe pregnancy. The World Health Organization recommends that pregnant women have at least four ANC visits for a healthy pregnancy. However, it is unclear whether this guideline is being followed in Mogadishu, Somalia. Therefore, this study aims to investigate the factors that influence ANC attendance among pregnant women in Mogadishu, Somalia.
Methods
A cross-sectional study was conducted at two hospitals, involving 329 pregnant women in their third trimester. Data were collected using structured questionnaires through face-to-face interviews. Statistical analysis was performed with SPSS 26, using descriptive statistics and logistic regression to assess the association between variables, with a significance level set at a p-value of less than .05.
Results
Only 14% of women met the recommended minimum for ANC visits. Nulliparous women were less likely to attend ANC compared to those with children (adjusted odds ratio [AOR] = 0.1, p = .031). In contrast, women receiving home visits from healthcare workers had higher odds of attending ANC (AOR = 8.3, p < .001). Those who felt their appointments were too short also had lower odds of attending ANC (AOR = 0.3, p = .007).
Conclusion
Many pregnant women do not attend ANC services as the World Health Organization recommends, which suggests at least four visits. Factors influencing attendance include parity, healthcare worker home visits, and perceived appointment quality. Improving these factors, particularly home visits and appointment durations, could enhance ANC attendance.
Background
Antenatal care (ANC) is the point of contact between healthcare providers and pregnant women, during which interventions are offered to ensure the safety of both the mother and the fetus (Sabiti, 2023). Initiation of ANC attendance during the first trimester of pregnancy and optimal ANC care are crucial for the well-being of pregnant women and their unborn babies (Nagatani et al., 2023). The minimum number of ANC visits recommended by the World Health Organization (WHO) (four visits) was possible for less than a third of the pregnant women in Sub-Saharan African countries (Berhan & Berhan, 2014). Antenatal care is generally considered an effective method of improving outcomes in pregnant women and their babies, although many specific ANC practices have not been subject to rigorous evaluation (Apiso, 2021). The elements of ANC consist of identifying risks, preventing and managing pregnancy-related illnesses, and promoting health education. (Tiruaynet & Muchie, 2019).
In recent years, there has been a considerable enhancement in the global accessibility of ANC services (Kuhnt & Vollmer, 2017). The Sustainable Development Goals target a global maternal mortality ratio not greater than 70 maternal deaths per 100,000 live births by 2030. Maternal mortality is high in many countries to the point that every minute, a woman dies due to pregnancy-related complications (Gitonga, 2017). Nearly 4 million neonatal deaths and 500,000 maternal deaths are estimated to occur annually in the world. About 98% of these occur in low and middle-income countries (Tran et al., 2012). Maternal and neonatal morbidity and mortality have continued to be a major problem in developing countries despite efforts to reverse the trend (Banda et al., 2012). Despite the substantial growth in ANC services in developing countries, only a small proportion of pregnant women attend four or more ANC appointments (Konje et al., 2018). Twelve of the 25 countries that achieved 50% or more coverage of pregnant women with at least 4 ANC visits included Sub-Saharan African countries (Tran et al., 2012).
Recent reviews have highlighted numerous barriers to attending ANC in sub-Saharan Africa, such as the costs of healthcare services, transportation expenses, accessibility, support from partners and the community, the distance to healthcare facilities, past encounters with the healthcare system, and cultural perceptions (Kyei-Nimakoh et al., 2017). Additional barriers to accessing care include requirements that must be fulfilled before receiving services, long distances to clinics, scattered health services, prolonged waiting times, and negative interactions with healthcare workers (HCWs; Tengera et al., 2025). The quality of ANC is a crucial factor that is often overlooked. Research has shown that a woman's experience of care—especially whether she feels valued or rushed—significantly influences her willingness to continue seeking care (Alabi et al., 2023; Hibusu et al., 2024). This issue is critical in low-resource settings, where healthcare providers may be overwhelmed and struggle to provide comprehensive, patient-centered counseling (Grenier et al., 2022). Additionally, entrenched gender norms and dynamics of power within families significantly contribute, though they are frequently overlooked, to this issue. A woman's ability to make decisions and the backing of her husband are vital factors that empower her to pursue care, while the absence of decision-making authority can serve as a significant obstacle (Garrison-Desany et al., 2021; Idris et al., 2023; Wassif et al., 2025).
Maternal and newborn mortality remains a major public health issue in developing countries, particularly those in Sub-Saharan Africa, and remains one of the key indicators of the Sustainable Development Goals set for the continuation of the unfinished business of the Millennium Development Goals time (Garenne, 2015). Utilizing maternal health services is identified as one of the most effective ways to lower the chances of complications and death for both mothers and newborns (Zamawe et al., 2016). Furthermore, the provision of ANC plays a crucial role in ensuring the well-being of newborns, which, in the long run, leads to decreased incidences of child mortality and malnutrition (Kuhnt & Vollmer, 2017). In Somalia, engagement of pregnant women with healthcare services that provide prebirth assistance is extremely rare (Jimale et al., 2020). As a result, a woman has a 1 in 22 chance of experiencing death due to complications related to pregnancy or childbirth (Miikkulainen et al., 2023). Data indicate that Somalia, along with seven other countries in sub-Saharan Africa, is among the 15 places with the highest rates of women dying during or after childbirth (Adedokun & Yaya, 2020). Despite the high maternal mortality rates in Somalia, engagement with healthcare services is remarkably low. Therefore, this study aims to analyze the factors influencing ANC attendance among pregnant women in Mogadishu, addressing the lack of recent data and documentation of ANC services in the area. Understanding these determinants is essential for improving access and utilization of ANC services and guiding effective public health interventions.
Review of Literature
Antenatal care offers a variety of essential services aimed at promoting the best possible health outcomes for both the mother and the fetus. These services include administering micronutrient supplements, such as iron and folic acid, to prevent nutritional deficiencies; providing important vaccinations to protect against infectious diseases; and offering counseling and testing for HIV to facilitate early detection and management (Myburgh et al., 2024). Consistent attendance at ANC appointments is associated with significant improvements in health outcomes, particularly through the early identification of complications, which can help reduce maternal illness and mortality. Additionally, regular participation in ANC increases the likelihood of giving birth in a healthcare facility, ensuring access to skilled care during delivery. This shift to facility-based births is crucial for reducing both maternal and neonatal mortality rates, as highlighted by Berhan & Berhan (2014).
Despite the well-documented benefits of ANC, attendance rates, especially in low- and middle-income countries, remain suboptimal (Konje et al., 2018). A substantial body of literature has examined various factors that influence a pregnant woman's decision and ability to seek and adhere to ANC services. One significant finding is that women with higher levels of education are much more likely to attend four or more ANC visits during their pregnancies. This correlation suggests that education enhances awareness of the importance of regular healthcare visits and the benefits they provide for both mother and child (Mathe, 2017). Having access to different media outlets and reliable information about ANC services is vital for increasing attendance rates among pregnant women. By providing precise and thorough information about the advantages and accessibility of ANC, including regular check-ups, nutritional advice, and maternal health education, we can enable women to prioritize their own health and that of their infants (Ahmed et al., 2024).
Age is another important factor affecting attendance at ANC. Research shows that younger women tend to utilize antenatal services more than older women. In contrast, older women, who may have experienced multiple pregnancies and various challenges, might not recognize the need to attend ANC as regularly (Andriani et al., 2022). Additionally, marital status can influence ANC attendance. A study conducted in Rwanda found that unmarried women who do not have support from family, relatives, or friends face a greater likelihood of limited access to and utilization of ANC services (Rurangirwa et al., 2017). Economic status also plays a crucial role in attendance. Women from wealthier families typically have better access to healthcare resources, including transportation and medical facilities, making them more likely to complete the recommended number of ANC visits (Ahmed et al., 2024). Women who actively plan their pregnancies also demonstrate a greater likelihood of adhering to the recommended ANC schedule. Such women are generally more proactive in seeking care and understand the importance of this care for their own health and that of their child (Mbarushimana & Nsanzabera, 2024).
Furthermore, access to healthcare facilities for ANC attendance is hindered by factors such as long distances to clinics, high transportation costs, poor road infrastructure, and inadequate transportation options (Khan et al., 2024; Nyathi et al., 2017). The quality, availability, and organization of ANC services significantly impact attendance rates. Ensuring timely services and access to essential medical supplies is vital for removing barriers that may prevent women from attending their appointments (Muhirwe & Aagard, 2023). Additionally, the nature of interactions with healthcare providers is crucial; supportive supervision and the absence of mistreatment can create a positive healthcare experience that encourages women to attend their ANC visits (Mbarushimana & Nsanzabera, 2024).
While considerable research has addressed global factors affecting ANC attendance, research on ANC attendance in Mogadishu, Somalia, is limited, despite unique sociodemographic and healthcare challenges in the capital. The city's high population and mainly privatized healthcare system create barriers to accessing ANC services, compounded by ongoing civil unrest and political instability. This study addresses this critical gap by providing a detailed, context-specific analysis of the factors influencing ANC attendance among pregnant women in Mogadishu, Somalia.
Methods
Study Design and Population
The cross-sectional study, which used a quantitative approach, was conducted from May to June 2025. It included all pregnant women in their third trimester (28+ weeks) attending ANC services at selected hospitals in Mogadishu, Somalia. Mentally unstable pregnant women, those with obstetric emergencies, and those who did not consent to participate were excluded from the study. The participant flowchart is shown in Figure 1.

Participant Sqqqelection Flowchart.
The study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines to enhance transparency and comprehensiveness in reporting. By adhering to these guidelines, researchers ensured clear articulation of study design, methodology, and findings, including participant selection, data collection, and statistical analyses. This application strengthens the credibility of observational research and aids in the evaluation and replication of the study by other researchers (Von Elm et al., 2007).
Study Setting
The research was conducted at two prominent hospitals in Mogadishu, Somalia. One hospital, Banadir Hospital, is located in Wadajir, a large district, while the other, Shangaani Referral Hospital, is situated in the smaller Shangaani district. This initiative aims to involve a diverse group of pregnant women to ensure participation from various demographic backgrounds. By doing this, the study seeks to gather comprehensive insights that accurately reflect the experiences and needs of different communities in the region.
Sample Size and Sampling Procedure
The researchers used Fisher's formula to determine the sample size, which is n = [Z^2×p (1-p)] / d^2, where p is the assumed proportion of pregnant women who completed ANC contacts, which is set at 28%, or 0.28 (Omar Haji Elmi et al., 2021), with a 95% confidence interval and a margin of error of 0.05. The calculation yielded a sample size of 310, as shown below:
(1.96)2(0.28)(1−0.28)/(0.05)2 = 310
To account for nonresponse, 10% was added to the sample size as recommended by Tumiran (2024), resulting in a final sample size of 341. Participants were selected using consecutive sampling, where each member of the population who met the selection criteria was chosen for the sample, resulting in a sequence of subjects. The participants were selected based on their daily attendance at ANC services until the target sample size was reached.
Data Collection
A questionnaire was developed based on existing tools (Alanazy & Brown, 2020; Banda et al., 2012; Gitonga, 2017; Steele et al., 2021; Tawfiq et al., 2023), with some adaptations made and additional questions included where suitable tools were unavailable. Face-to-face interviews were conducted to collect data from participants using this structured questionnaire. A pilot study was conducted with 35 participants, representing 10% of the total sample size (Bujang et al., 2024), who were recruited from SOS Hospital. The aim was to assess the clarity of the questions, estimate the time required for administration, and identify any logistical challenges before launching the main study. To ensure the reliability of the questionnaire, a Cronbach's alpha test was performed, resulting in a score of 0.84, which indicates good internal consistency. The data collected during this pilot phase were not included in the final analysis.
Variables
The study included several independent variables, consisting of sociodemographic factors such as age, marital status, education level, occupation, income, number of pregnancies (gravida), number of live births (parity), and the desire for pregnancy. Additionally, factors related to healthcare access were considered, including transportation costs, distance to the facility, home visits by health workers, clarity of communication, waiting times for appointments, availability of a midwife at the facility, the nature of appointments, and the availability of medical supplies.
The dependent variable in this study was ANC attendance, which was determined by asking respondents if they had attended ANC visits during their pregnancy. This information was further validated by reviewing clinic records. The categorization of targeted ANC defined “uptake” as pregnant women who attended at least four ANC visits, while “nonuptake” referred to those who attended fewer than four visits.
Data Analysis
Data were analyzed using IBM SPSS Statistics for Windows, Version 26.0 (Armonk, NY: IBM Corp.). Descriptive statistics, including frequency tables and percentages, were utilized to summarize the quantitative variables. Additionally, crude and adjusted odds ratios were calculated with a 95% confidence interval. In the multivariable logistic regression model, variables with a p-value of less than .25 in the bivariate analysis were included. Factors related to the outcome variable were assessed, and potential confounders were controlled for using multivariable logistic regression with odds ratios and 95% confidence intervals. All results were considered significant if the p-value was less than .05. Finally, the model is consistent with the data, as shown by the Hosmer–Lemeshow goodness-of-fit test, which returned a p-value of .920.
Ethical Considerations
The Ethical Review Board of the National Institute of Health (NIH)—Somalia has approved the study (Ref: NIH/IRB/55/DEC/2024). An oral consent form was utilized, and the researchers obtained permission from the respondents before conducting the research. Participation was voluntary, and respondents were not pressured to complete the questionnaire. The researchers ensured that all personal information would be kept confidential. Since the study is purely observational, no additional risks are expected beyond those associated with the standard management protocol.
Results
Sociodemographic Characteristics of Participants and ANC Coverage
Of the 341 participants in the study, 329 completed the survey, resulting in a response rate of 96.5%. The majority of respondents were aged 20 or older (73.9%) and were married (66.9%). A significant portion of the participants were illiterate (57.8%), and many were unemployed (61.7%). In terms of monthly earnings, just over half of the participants reported earning at least 200 USD (52.3%). Additionally, 77.5% of the participants were multigravida, and 77.8% had one or more children, with 75.7% expressing a positive intention regarding future pregnancies (Table 1). Regarding ANC, most participants had attended at least one visit (35%), while 14% had attended four or more visits (Figure 2).
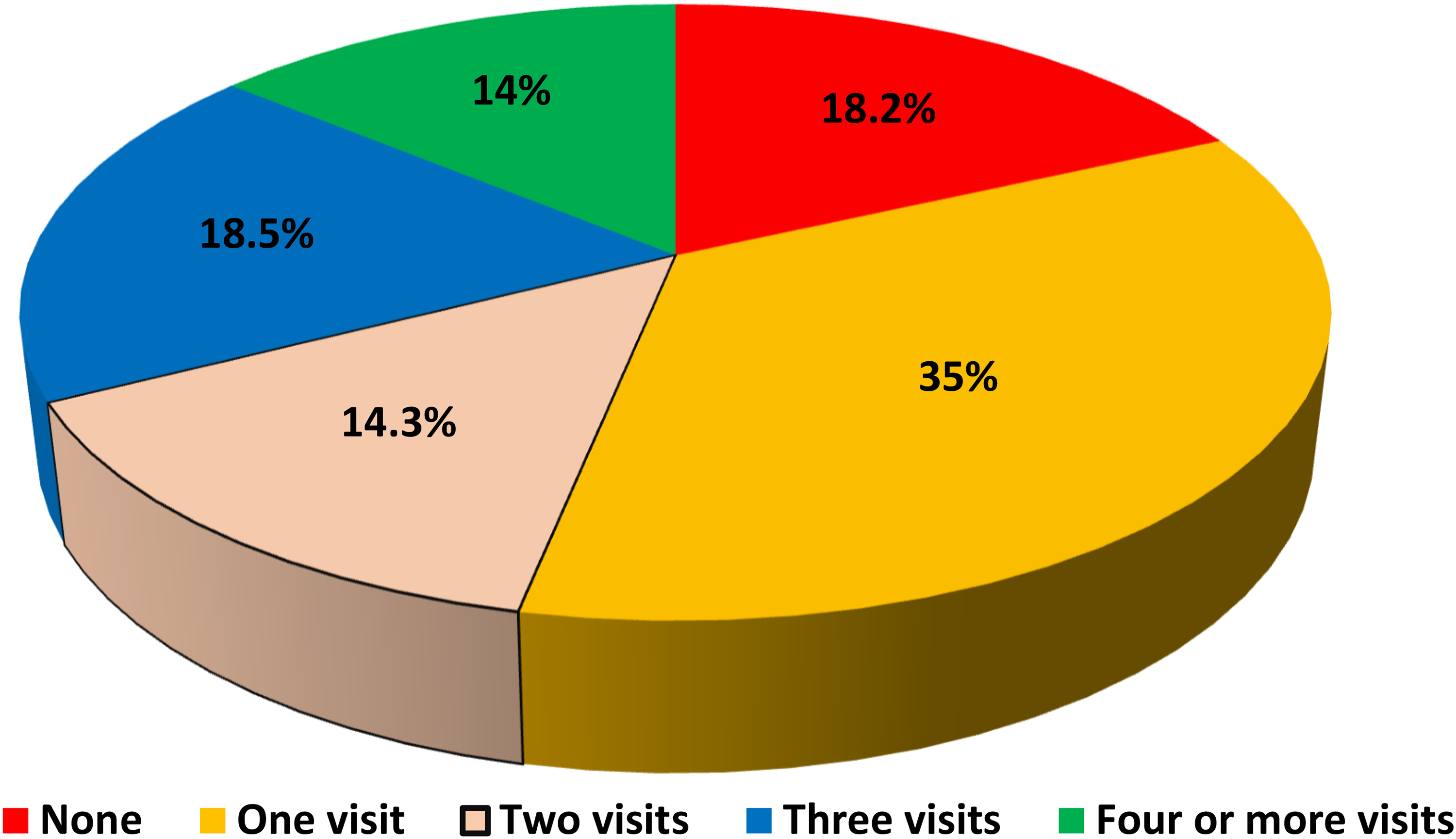
Distribution of antenatal care visits among participants.
Sociodemographic Characteristics of Participants.

USD = United States Dollar.
Healthcare Access Characteristics for Study Participants
In Table 2, a significant number of participants (70.2%) reported that transportation costs were expensive. Additionally, distance to the health facility posed a barrier for many, with 66% living at least 5 km away. Furthermore, 60.2% of participants indicated that they were not visited by HCWs at home. On a positive note, communication seemed to be effective, as 74.5% of respondents reported that they understood the language used by HCWs. However, waiting times for appointments were a concern; over half (51.4%) of participants waited 2 h or more. Many participants (74.8%) also felt that the appointments were too short and rushed. Regarding facility resources, a midwife was present at the health facility for the majority of participants (71.7%). Additionally, the availability of medical supplies was viewed positively by a substantial majority (80.9%).
Healthcare Access Characteristics for Study Participants.

HCW = Healthcare Workers.
Factors Affecting ANC Attendance among Participants
In the bivariable logistic regression analysis, factors such as marital status, monthly income, gravidity, parity, distance to health facilities, home visits by HCWs, waiting times for appointments, the nature of appointments, the presence of a midwife at the health facility, and the availability of medical supplies were all associated with the outcome variable. However, in the multivariable logistic regression analysis, parity, home visits by HCWs, and the nature of appointments were found to significantly influence ANC attendance among pregnant women (Table 3).
Factors Affecting Antenatal Care Attendance among Participants.
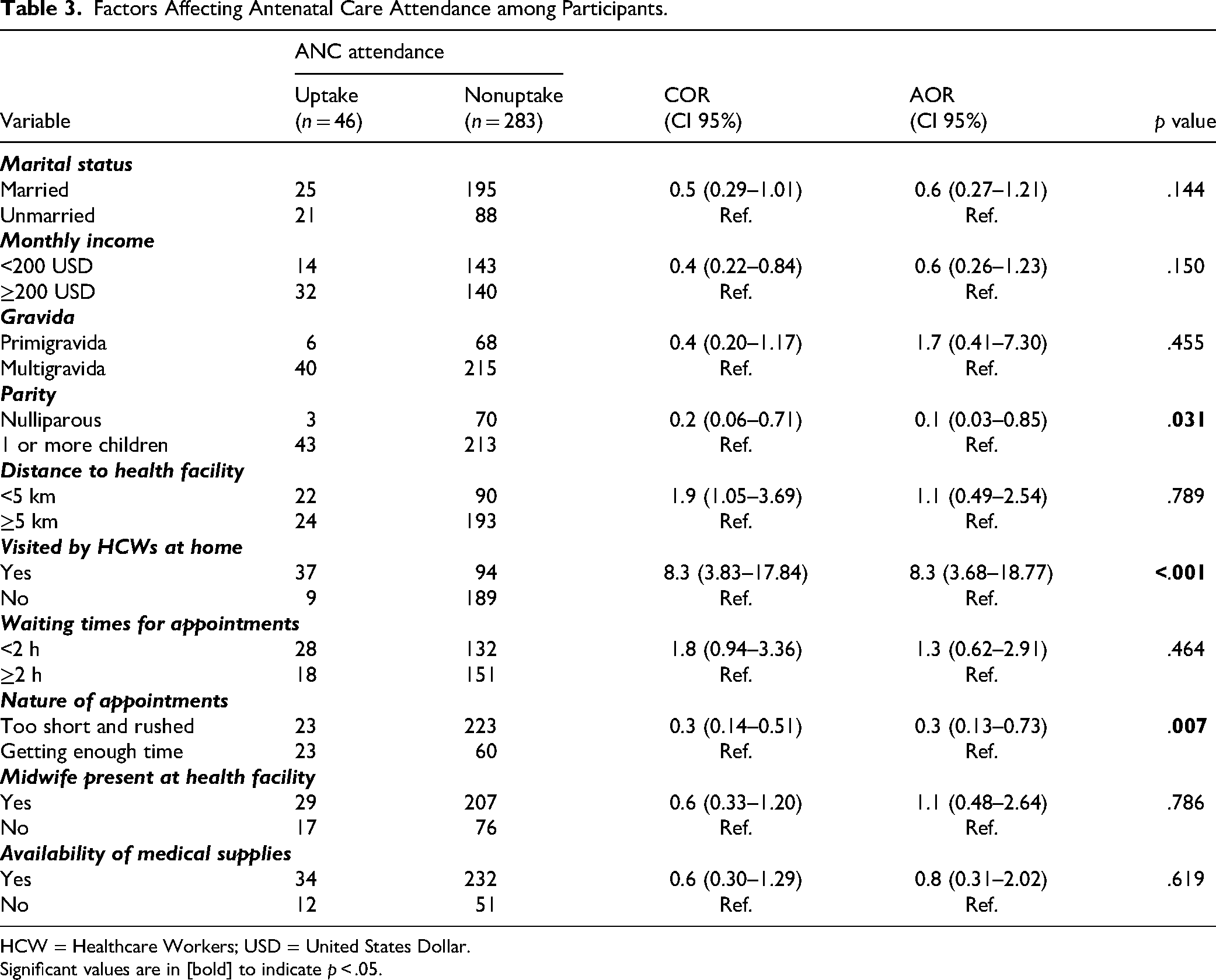
HCW = Healthcare Workers; USD = United States Dollar.
Significant values are in [bold] to indicate p < .05.
Nulliparous women had significantly lower odds of attending ANC compared to women with one or more children (adjusted odds ratio [AOR] = 0.1, 95% confidence interval [CI]: 0.03–0.85; p = .031). Conversely, participants who received home visits from HCWs had significantly higher odds of attending ANC (AOR = 8.3, 95% CI: 3.68–18.77; p < .001). Additionally, participants who felt their appointments were too short and rushed had significantly lower odds of attending ANC (AOR = 0.3, 95% CI: 0.13–0.73; p = .007).
Discussion
This study aimed to evaluate the factors influencing ANC attendance among pregnant women in Mogadishu, Somalia. The results show that only 14% of the pregnant women completed the minimum requirement of at least four ANC visits, highlighting significant barriers to accessing and receiving quality maternal healthcare. This finding is consistent with similar studies conducted in Uganda (16%) (Aidah & Kizito, 2022), South Africa (21%) (Nxiweni et al., 2022), and Ethiopia (21.5%) (Gebeyehu et al., 2024), indicating low utilization of ANC services. Conversely, this percentage is significantly lower than those reported in surveys from China (78.79%) (Hu et al., 2021) and India (59.25%) (Girotra et al., 2023). The observed differences may stem from the diverse backgrounds of the study populations. Additionally, many Somali women view pregnancy and childbirth as natural life events, seeking medical assistance primarily when complications arise.
The present study found a statistically significant relationship between a woman's parity (the number of times a woman has given birth) and the utilization of adequate ANC. Nulliparous women, or those who have never given birth, were found to be 90% less likely to attend ANC frequently compared to women who had one or more children. This finding was in line with a previous study from Malaysia (Yeoh et al., 2016). However, this result contradicts studies conducted in Pakistan (Aziz Ali et al., 2020) and Afghanistan (Stanikzai et al., 2024). The possible explanation for this may be that women who have never given birth often believe that ANC is only necessary for those with complications. This misconception can lead them to delay or skip checkups (Comfort et al., 2022). Additionally, since nulliparous women have never given birth before, they might underestimate the level of care they need compared to women who have previously experienced pregnancy and childbirth, knowing what to expect (Miranda et al., 2011).
Additionally, the study revealed that women who received home visits from HCWs during their pregnancy were 8.3 times more likely to attend the minimum required number of ANC visits than those who did not receive home visits. This coincides with previous findings conducted in India (Kusuma et al., 2024), Mali (Kayentao et al., 2023), and Uganda (Acup et al., 2023). A likely clarification for this might be that mothers who got home visits from health workers in their community were more likely to go to the suggested four checkups before giving birth. This is because the health workers cheered them on and helped them, which highlights how vital it is for moms and babies to go to the clinic regularly (Stansert Katzen et al., 2020). Visiting people at home can also help address issues that make it difficult to go to clinics, which include transportation problems, long wait times, and not understanding the importance of antenatal check-ups (Agarwal et al., 2019). This correlation underscores the importance of HCW engagement in promoting maternal health.
Moreover, the results indicated that the use of ANC services among pregnant women in Mogadishu City was negatively affected by the nature of their appointments. Women who felt their appointments were too short and rushed were 70% less likely to utilize ANC services adequately compared to those who thought they had ample time during their appointments. This finding was in line with a previous report from Australia (Penman et al., 2023), which indicates that feeling rushed during ANC appointments can hinder women's access to timely and adequate ANC. This might mainly happen because shorter appointment lengths may be inadequate for effectively addressing patient concerns, which may compromise the quality of care provided (Swanson et al., 2022). A woman's perception of how HCWs treat her greatly affects her overall experience and willingness to continue seeking prenatal care. If she feels disconnected, disrespected, unappreciated, or unsupported in expressing her feelings, it can significantly impact her engagement with the healthcare system (Penman et al., 2023). The well-being of healthcare providers is a crucial factor influencing the quality and utilization of ANC. Professional burnout can negatively impact the quality of care, resulting in hurried appointments and a weakened connection with patients (Pham et al., 2025). This is particularly relevant in resource-constrained settings like Mogadishu, where providers may face emotional and physical exhaustion. Women often feel less inclined to utilize ANC when appointments are brief. Improving working conditions, staffing, and mental health support for providers may enhance maternal healthcare services in such contexts.
The frequency of visits and the length of appointments are important, but the quality of antenatal counseling plays a crucial role in a woman's engagement with ANC services and her overall health outcomes (Hijazi et al., 2018; Saad-Haddad et al., 2016). Effective counseling goes beyond a quick check-up; it requires healthcare providers to spend adequate time educating women on various topics such as maternal nutrition, emotional and psychological support, warning signs during pregnancy, family planning and HIV prevention, birth preparedness, and newborn care (Boah et al., 2024; Pricilla et al., 2017). The study found that women who felt their appointments were rushed were less likely to complete their ANC schedule. This may be linked to their perception of the lack of quality counseling. If appointments are too brief, healthcare providers may lack sufficient time to address patient issues or to deliver comprehensive education. As a result, women may feel uninformed and disengaged, which defeats the purpose of the ANC visit.
In addition to addressing the barriers to general ANC attendance, it is essential to consider the specific needs of high-risk pregnancies, as these can significantly affect perinatal outcomes. Conditions such as twin pregnancies (Tran Thi et al., 2025), gestational diabetes (H. G. Nguyen et al., 2024), and abnormal placental location (P. N. Nguyen et al., 2024) require more frequent and specialized monitoring than standard pregnancies. These cases often necessitate care at specialized, well-equipped healthcare centers with expertise in maternal–fetal medicine (Van Otterloo & Connelly, 2018). The limited use of ANC services observed in this study indicates that many high-risk cases may not be receiving the intensive, specialized care they require, potentially leading to poor perinatal outcomes for both the mother and the baby. Therefore, future interventions in Mogadishu should focus not only on improving general ANC attendance but also on establishing clear referral pathways and educating both women and healthcare providers about the importance of specialized care for high-risk conditions.
Strengths and Limitations
This study has some limitations. The primary limitation is its cross-sectional design, which restricts the ability to establish cause-and-effect relationships among the variables. Furthermore, the research was conducted in healthcare facilities and may not account for pregnant women who remain in the community. Lastly, using consecutive sampling could lead to biased samples, limiting the broader applicability of the findings. As participants were selected based on their availability, the sample may not accurately represent the wider population, making the results less relevant beyond the specific group studied.
Despite these limitations, the study boasts several key strengths. First, it provides valuable insights into the factors influencing the uptake of ANC services during pregnancy, which is crucial today. Second, a diverse, population-based sample was utilized, enhancing the generalizability of the findings. Third, self-reported ANC attendance was validated by reviewing clinic records. This approach minimizes recall bias and social desirability bias, thereby strengthening the accuracy and trustworthiness of the data regarding the dependent variable. Finally, rigorous statistical methods, including descriptive and multivariable logistic regression, were employed, reporting both crude and adjusted odds ratios with 95% confidence intervals. This sophisticated methodology effectively controlled for confounding variables and identified significant factors.
Implications for Practice
The study highlights that many pregnant women in Mogadishu are not accessing ANC as recommended, which has significant implications for nursing practices. To address this issue, nurses should adopt a community-oriented approach by conducting home visits and providing health education at local centers to overcome barriers related to facility access. Enhancing training in patient-centered communication is essential to ensure respectful and responsive interactions that foster trust and increase attendance. The findings also indicate a need for reforms in healthcare education. Nursing and medical curricula should incorporate cultural competency and context-specific modules to better prepare future providers for the unique challenges in Mogadishu. Educational initiatives should prioritize community engagement, encouraging students to collaborate with local leaders on sustainable health interventions. Developing tailored educational materials to address the specific barriers faced by nulliparous women is also crucial.
While the study offers a quantitative overview, the identified barriers highlight the need for action-oriented nursing research. Future studies should move beyond descriptive analysis and focus on intervention trials that effectively apply findings in practice led by nursing professionals. These interventions should rigorously test the efficacy of nurse-led home visiting programs, determining the optimal frequency and content needed to improve ANC uptake. Additionally, it is essential to evaluate quality improvement interventions that enhance nurse training in patient-centered communication to improve perceived appointment quality and attendance. This research is vital for aligning local nursing practices with evidence-based strategies and helping healthcare systems meet the WHO's attendance targets. Furthermore, qualitative research is necessary to explore the lived experiences of both women and nurse–midwives, allowing for a better understanding of the systemic challenges (such as workload and resource allocation) that limit the quality of counseling provided. Finally, policymakers are urged to use these insights to allocate resources effectively and develop policies that strengthen community health programs, highlighting the pressing need for greater investment in ANC and for improving healthcare infrastructure to ensure services are accessible and responsive to community needs.
Conclusion
This study found a low attendance rate at ANC services, with only 14% of women attending as recommended by the WHO. Key factors influencing attendance include parity (the number of births a woman has had), home visits by HCWs, and the perceived quality of the appointments. This represents a public health concern, contributing to higher maternal and neonatal mortality rates. The findings suggest that improving both accessibility and quality of ANC is essential. Emphasizing patient-centered care, such as longer consultations and positive interactions with providers, is crucial. Home visits can also help overcome barriers to clinic attendance. To improve outcomes, practical interventions addressing logistical challenges and the perceived importance of care are necessary.
Supplemental Material
sj-docx-1-son-10.1177_23779608251391489 - Supplemental material for Factors Affecting Antenatal Care Attendance among Pregnant Women in Mogadishu, Somalia
Supplemental material, sj-docx-1-son-10.1177_23779608251391489 for Factors Affecting Antenatal Care Attendance among Pregnant Women in Mogadishu, Somalia by Walid Abdulkadir Osman, Aweis Ahmed Moallim Abdullahi, Hassan Muse Ahmed, Khalid Abdukadir Osman, Abdiwali Abdullahi Abdiwali and Ahmed Mohamud Hussein in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251391489 - Supplemental material for Factors Affecting Antenatal Care Attendance among Pregnant Women in Mogadishu, Somalia
Supplemental material, sj-docx-2-son-10.1177_23779608251391489 for Factors Affecting Antenatal Care Attendance among Pregnant Women in Mogadishu, Somalia by Walid Abdulkadir Osman, Aweis Ahmed Moallim Abdullahi, Hassan Muse Ahmed, Khalid Abdukadir Osman, Abdiwali Abdullahi Abdiwali and Ahmed Mohamud Hussein in SAGE Open Nursing
Footnotes
Acknowledgments
The authors express gratitude to the study participants for their time, effort, and contributions to the research.
Ethical Considerations
The Ethical Review Board of the National Institute of Health (NIH)—Somalia has approved the study (Ref: NIH/IRB/55/DEC/2024). An oral consent form was utilized, and the researchers obtained permission from the respondents before conducting the research. Participation was voluntary, and respondents were not pressured to complete the questionnaire. The researchers ensured that all personal information would be kept confidential. Since the study is purely observational, no additional risks are expected beyond those associated with the standard management protocol.
Author Contributions
Walid Abdulkadir Osman: conceptualization, methodology, data curation, formal analysis, writing—original draft, writing—review and editing, and supervision. Aweis Ahmed Moallim Abdullahi: conceptualization, methodology, data curation, software, and writing—review and editing. Hassan Muse Ahmed: conceptualization, methodology, formal analysis, and writing—review and editing. Khalid Abdukadir Osman: conceptualization, software, data curation, and writing—review and editing. Abdiwali Abdullahi Abdiwali: conceptualization, data curation, and writing—review and editing. Ahmed Mohamud Hussein: conceptualization, data curation, and writing—review and editing. All authors read and approved the final version of the manuscript for submission.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets used and analyzed in this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.