
Abstract
Background
Nursing care documentation, which is the record of nursing care that is planned for and delivered to individual patients, can enhance patient outcomes while advancing the nursing profession. However, its practice and associated factors among Ethiopian nurses are not well investigated.
Objective
To assess the level of nursing care documentation practice and associated factors among nurses working at public hospitals in Ethiopia.
Methods
An institutional-based cross-sectional study was conducted from May 1 to 30, 2022. A total of 378 nurses and corresponding charts were randomly selected with a multistage sampling technique. Self-administered structured questionnaires and structured checklists were used to collect data about independent variables and nurses’ documentation practice, respectively. Epi Data 4.6 was used for data entry and SPSS version 25 for analysis. Descriptive statistics and binary logistic regression analysis have been employed. The STROBE checklist was used to report the study.
Results
In this study, 372 nurses participated, and 30.4% (95% confidence interval [CI]: 26%–35%) of them had good nursing care documentation practice. Adequate knowledge about nursing care documentation(adjusted odds ratio [AOR] = 4.16, 95% CI: [2.36–7.33]), favorable attitude toward nursing care documentation (AOR = 3.43, 95% CI: [1.85–6.36]), adequacy of documenting sheets (AOR = 2.02, 95% CI: [1.14–3.59]), adequacy of time (AOR = 3.85, 95% CI: [2.11–7.05]), nurse-to-patient ratio (AOR = 2.78, 95% CI: [1.13–6.84]), and caring patients who had no stress, anxiety, pain, and distress (AOR = 3.56, 95% CI: [1.69–7.52]) were significantly associated with proper nursing care documentation practices.
Conclusion
Nursing documentation practice was poor in this study compared to the health sector transformation in quality standards due to the identified factors. Improving nurses’ knowledge and attitude toward nursing care documentation and increasing access to documentation materials can contribute to improving documentation practice.
Introduction
Nursing documentation, which is defined as the record of nursing care that is planned and delivered to individual patients, is an integral, vital, and important part of professional nursing practice (Hariyati et al., 2016; Osama et al., 2016). Nursing care documentation can be electronic-based or manual and has been accepted as an essential aspect of professional practice for nurses since the Florence Nightingale era (Nightingale, 1992).
Clear, accurate, and accessible documentation is an essential element of safe, quality, and evidence-based nursing practice (ANA, 2010). Additionally, it should be client-focused, chronologically written, confidential, and timely (Hameed & Allo, 2014). However, available pieces of evidence illustrated that nursing records are often incomplete, lack accuracy, and have poor quality (Gomes et al., 2016; Kebede et al., 2017; Lindo et al., 2016).
Adequate nursing documentation practice will benefit the patient, the health professionals, and the healthcare institution in various ways. Primarily, it is essential for clinical communication between healthcare teams and ultimately supports clinical decision-making, delivery of quality care, and continuity of care (Herisiyanto et al., 2020; Törnvall & Wilhelmsson, 2008; Zegers et al., 2011). It also provides information for other professionals, mainly for individuals and groups involved with accreditation, credentialing, legal, regulatory, legislative, reimbursement, research, and quality activities (ANA, 2010; Zegers et al., 2011). It improves the credibility of the institution and makes the nursing profession visible (Nakate et al., 2015).
As stated by Ethiopia's Federal Ministry of Health Operational Standard for Nursing Care, every nursing care given must be accurately and clearly documented (Federal Minister of Health, 2011). However, findings from some regions of the nation revealed a suboptimal documentation practice that ranges from 37.4% to 47.8% (Andualem et al., 2019; Kebede et al., 2017; Tamir et al., 2021; Tasew et al., 2019).
Inadequate nursing care documentation negatively impacted patient care, professional accountability, and the organization as a whole (Blair & Smith, 2012). It makes it difficult to determine the care that patients have received (Mamseri, 2012), results in a lack of support when ethical and legal problems arise (Kebede et al., 2017), makes it challenging to conduct retrospective audits and research activities (Mamseri, 2012), leads to errors like medication administration errors (Feleke et al., 2015; Khoo et al., 2012), and contributes to patient mortality (Rossetti et al., 2013; Rothman et al., 2012).
Review of Literature
Despite the importance of nursing care documentation, available evidence showed limitations in its practice (Kebede et al., 2017; Wang et al., 2011). Various studies conducted worldwide have reported varying degrees of documentation by nurses. A cross-sectional study conducted in European countries revealed that an adequately documented nursing care was only 28% (Ausserhofer et al., 2014). A study in Iraq showed that 50.7% of nurses had a weak documentation practice (Jebur & Mohammed, 2017). Another study conducted in long-term care settings in Canada found that the maximum proportion of symptoms documented in the nursing notes was found to be 53.5% (Voyer et al., 2014). A study in Iraq showed that the overall documentation level in nursing practice was poor (Al Hilfi et al., 2018).
In Africa, a study conducted in Nigeria showed that good nursing documentation was practiced by 70% (Taiye, 2015). Another study conducted in Ghana found that the most frequent documentation errors included unsigned entries (57.1%), undeclared late entries (53.1%), no time of procedure/intervention/event in nurses’ notes (51%), and cancellations not being clear and endorsed (46.9%) (Asamani et al., 2014). Specifically in Ethiopia, a study conducted in Gondar indicated that slightly more than one-third (37.4%) had good nursing care documentation practice (Kebede et al., 2017). Other studies done in Ethiopia, particularly in the West Gojjam zone, Tigray, and Eastern Ethiopia showed that 47.5%, 47.8%, and 47.5% of nurses had a good documentation practice, respectively (Andualem et al., 2019; Tamir et al., 2021; Tasew et al., 2019).
Different factors are associated with nursing care documentation. These include age, gender, work setting, length of employment, knowledge, and attitude of nurses about nursing documentation, increased patient admissions, and shortage of recording material (Alhawri et al.; Ball et al., 2016; Bijani et al., 2016; Jasemi et al., 2013; Mutshatshi et al., 2018; Nakate et al., 2015; Taiye, 2015; Tamir et al., 2021). Studies also identified that different nursing care models could improve the accuracy of nursing documentation (Blair & Smith, 2012). Models such as the primary nursing model (Cocchieri et al., 2023), team nursing care model (Fowler et al., 2006), and the VIPS model (Akhu-Zaheya et al., 2018; Björvell et al., 2003) facilitate accurate and consistent documentation. Each model offers distinct approaches, from standardized language usage to one-to-one care relationships, ensuring thorough and detailed documentation, promoting communication among healthcare teams, and ultimately improving the accuracy and completeness of patient records.
Even though research has been conducted to fill the evidence gap in some parts of Ethiopia, there are methodological and representation gaps such as failing to include information from chart reviews and failing to take into account some factors. Therefore, this research aims to assess the practice of nursing care documentation and its associated factors among nurses working at public hospitals in Ethiopia by considering unaddressed factors.
Methods and Materials
Study Area, Design, and Period
An institution-based cross-sectional study was conducted in May 2022 at public hospitals in the Central and North Gondar zones, which are two of the 12 zones of the Amhara Regional State. The Central Gondar Zone is located in Ethiopia's northwestern highlands and is part of the Amhara Regional State. It is 737 km from Addis Ababa, the capital city of Ethiopia's Federal government, and 168 km from Bahir Dar, the capital city of Amhara National Regional State. The North Gondar zone is located 836 km away from Addis Ababa and 270 km away from Bahir Dar in the northwest direction. The Central Gondar zone consists of nine primary hospitals and one comprehensive specialized hospital with a total of 1,104 nurses. The North Gondar zone consists of two primary hospitals with 27 nurses and one general hospital that consists of 95 nurses.
The research was conducted across eight hospitals, namely, Koladiba Primary, Guhala Primary, Delgi Primary, Sanja Primary, Tsegedie Primary, Aykel Primary, Debark General, and Gondar University Hospital. These selected healthcare facilities collectively comprise over 640 beds. It is noteworthy that these hospitals collectively admit approximately 21,000 patients annually.
Research Questions
What is the level of nurses’ documentation practice?
What are the factors that affect nurses’ documentation practice?
Inclusion and Exclusion Criteria
Inclusion Criteria
Nurses working in the inpatient departments of selected hospitals and those who have worked at least for 6 months were included in this study. The decision to include nurses with a minimum of 6 months’ work experience was influenced by the local context, where nurses typically attain permanent employment after this duration in Ethiopia. This milestone of 6 months often marks a point where nurses shift from temporary roles to secure permanent positions within the healthcare system.
The medical records included in the study were limited to those available in the inpatient departments of the selected hospitals during the data collection period. Additionally, only records documented by the specified nurses designated for this study were considered for inclusion.
Exclusion Criteria
Nurses who were on annual leave, maternity leave, and unable to participate in the study due to illness at the time of the data collection were excluded.
Sample
The sample size was determined using a single population proportion formula, taking the proportion as 38.5% from a previous study conducted in the Eastern Ethiopia Public Hospital (Tamir et al., 2021), with a 95% confidence interval (CI) and a 5% margin of error. Thus, based on the above formula, the sample size was calculated to be 364. Since the study population is less than 10,000, a correction formula was used resulting in a sample size of 229. Finally, by adding a 10% nonresponse rate and considering the design effect of 1.5, the final sample size was 378
A multistage sampling technique was used. Initially, a list of all public hospitals in the Central and North Gondar zones was obtained from the Amhara Regional Health Bureau. Eight hospitals (Koladiba Primary, Guhala Primary, Delgi Primary, Sanja Primary, Tsegedie Primary, Aykel Primary, Debark General, and Gondar University Hospital) were selected by a lottery method from 13 public hospitals found in the Central and North Gondar zone, Ethiopia. Then, the number of nurses working in the inpatient departments was obtained from each institution. Subsequently, a proportional allocation based on the number of nurses in each hospital and department was applied. Finally, nurses working in each inpatient department from each selected hospital were selected using a computer-generated simple random sampling system. The same number of patient medical record charts (total 378) was selected from each hospital and department. The selection process for medical records involved considering only charts available in the inpatient departments of the selected hospitals during the data collection period, specifically documented by the designated study nurses. Finally, one chart per sampled nurse was selected randomly.
Study Variables
Operational Definition
Data Collection Instrument
A structured self-administered questionnaire was developed in the English language to collect data regarding independent variables. Questions were adopted from the Ethiopian Hospital Reform Implementation Guideline (FMOH, 2010) and adapted from various literature related to the topic (Andualem et al., 2019; Ayele et al., 2021; Tamir et al., 2021; Tasew et al., 2019).
The questionnaire comprises five sections: (1) Questions regarding sociodemographic characteristics of the participants; (2) Questions concerning knowledge of nurses on documentation; (3) Questions assessing the attitude of the respondents toward nursing documentation; (4) Questions assessing organizational factors; and (5) Questions concerning patient-related factors.
A structured and pretested English version standard checklist was adopted from Health Sector Transformation in Quality guidelines (FMOH, 2010) to collect data regarding the documentation practice of nurses through chart review. The checklist contained 17 items with a score of “1” and “0” for “Yes” and “No” responses, respectively. Content validity was ensured by involving two experienced nursing instructors proficient in clinical and research domains. Internal consistency was checked that gave Cronbach's alpha values of 0.71, 0.78, and 0.88 for knowledge, attitude, and practice questions, respectively.
Data Collection Procedure
Data collection was facilitated by six nurses with Bachelor of Science (BSc) degrees (four data collectors and two supervisors) after taking a 1 day training to familiarize themselves with the data collection procedure and instruments on the objectives and relevance of the study.
The purpose of the study was clearly explained to the participants, and their verbal consent was obtained before data collection for the self-administered questionnaire. A similar number of charts of the selected nurses has been reviewed using a structured checklist to collect data regarding nursing care documentation practice, and finally, each checklist has been attached to each respective respondent's questionnaire for data entry.
Data Quality Assurance
Two senior professional nurses reviewed the self-administered questionnaire and checklist for content validity, and some changes were made in response to their feedback. Before the actual data collection, the items were tested on 19 (5% of 378) nurses working at the Addis Zemen Hospital, and the result was used to check the clarity and completeness of the questionnaire. Moreover, training was given to data collectors and supervisors, and the data collection process was supervised daily by the principal investigator to maintain the quality of data.
Statistical Analysis
Data were coded, entered into Epi Data version 4.6, and then exported to Statistical Package for Social Sciences (SPSS) version 25 after being thoroughly checked for completeness. After data had been cleaned, descriptive statistics such as frequency, percentage, and mean were used to analyze the data. The binary logistic regression analysis has been applied to identify the factors of the dependent variable. Variables with a P-value less than or equal to .25 in the bivariable analysis were taken as the candidates for the multivariable logistic regression model. The logistic regression model fitness was checked using the Hosmer–Lemeshow goodness of fit test with a P-value of .427. During the analyses, crude and adjusted odds ratios with a 95% CI and a P-value of 0.05 were considered. A P-value of less than .05 was taken to declare a significant association. Finally, the results have been presented in text and tables.
Ethical Consideration
Ethical approval was obtained from the institutional review board (IRB) of the Bahir Dar University, College of Medicine and Health Science (protocol number: 414/2022). A formal letter was submitted to each selected hospital, and approval had been obtained from the participating hospitals. Written informed consent was obtained from each respondent. This study implemented stringent data security measures to protect sensitive patient data, incorporating encryption, anonymization techniques, and access restrictions.
Results
Sociodemographic Characteristics of the Respondents
Out of the 378 sampled nurses, 372 returned the questionnaires, which made the response rate 98.4%. From a total of 372 nurses who participated in this study, 226 (60.8%) were females. The age of the study respondents ranged from 21 to 41 years with a median age of 27.5 years (IQR = 25–32). Most of the respondents (254, 68.3%) had bachelor's degrees; 83 (22.3%) had a college diploma, and the remaining 35 (9.4%) had MSc and above qualifications (Table 1).
Sociodemographic Characteristics of Nurses Working in Selected Public Hospitals, Central and North Gondar Zone, Ethiopia, 2022 (n = 372).

Organizational Factors
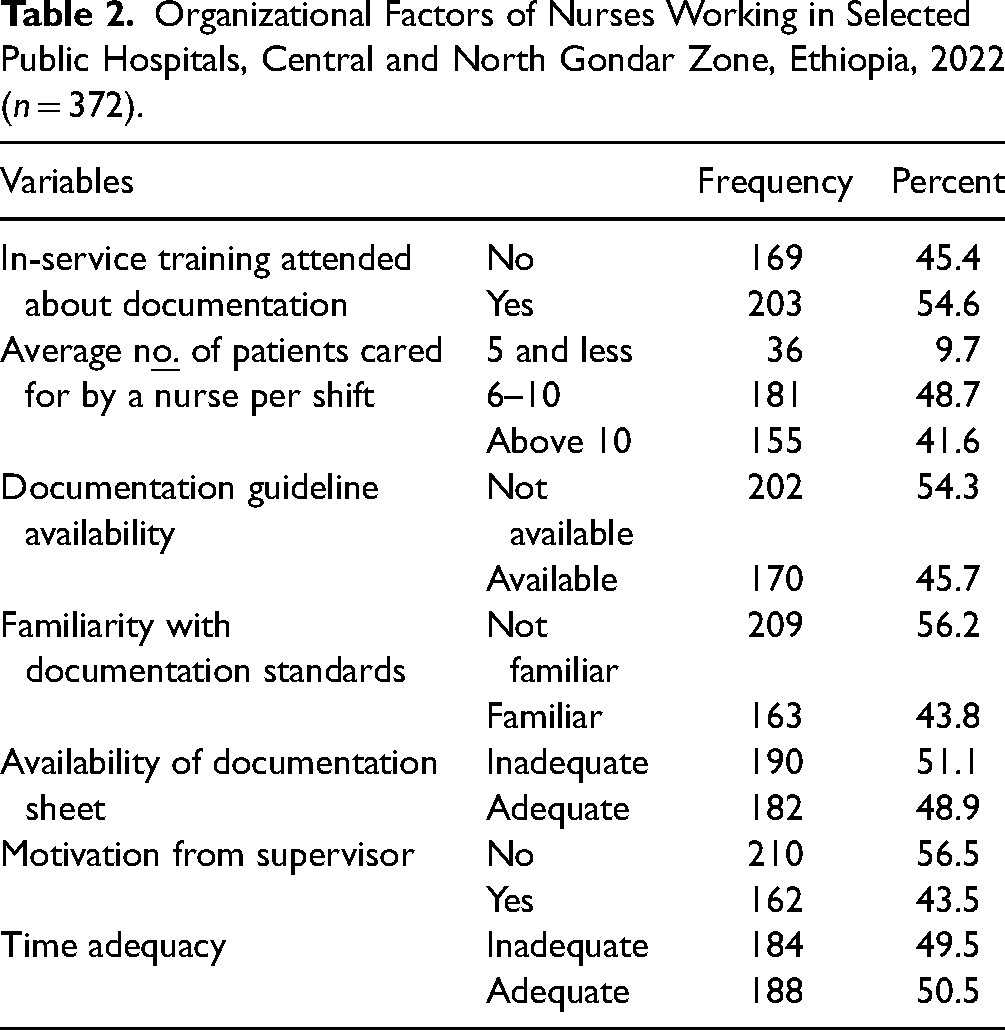
More than half of the respondents (203, 54.6%) had received in-service training on nursing care documentation. The majority of the respondents (336, 91.3%) were providing care to six or more patients per shift. In most of the inpatient wards, 190 (51.1%) of the respondents assured a shortage of nursing care documentation sheets (Table 2).
Organizational Factors of Nurses Working in Selected Public Hospitals, Central and North Gondar Zone, Ethiopia, 2022 (n = 372).
Nurses’ Knowledge and Attitudes of Nursing Care Documentation
Of the participants, 43% (95% CI: 37.9%–48.2%) of them had good knowledge regarding nursing care documentation. Out of the total respondents who participated in the study, almost all of them (364, 97.8%) knew that documentation is a professional responsibility.
On the other hand, 50.8% (95% CI: 45.6% to 56.0%) of the study participants had a favorable attitude toward nursing care documentation. Among all the respondents, 365 (98.1%) of them agreed that nursing documentation enhances the exchange of information between nurses and other healthcare providers. Similarly, 351 (94.4%) said proper documentation has a positive impact on patient safety. Additionally, 362 (97.4%) said that documentation makes nurses’ work visible.
Patient-Related Factors on Nursing Care Documentation
Patient-related factors that could potentially affect nursing documentation practice were assessed in this study. Similarly, more than two-thirds (263, 70.7%) of the study participants said that negative attitude of the patient toward nurses affect nursing care documentation (Table 3).
Patient-Related Factors Affecting Nurse's Documentation Practice Working in Selected Public Hospitals, Central and North Gondar Zone, Ethiopia, 2022 (n = 372).

Nursing Care Documentation Practice
Out of the total study participants, 30.4% (95% CI: 25.7% to 35.3%) had good nursing care documentation practices, and the remaining 69.6% had poor practices toward nursing care documentation.
Among the 372 charts reviewed, 247 (66.4%) had an attached nursing care plan format. Out of the charts with care plan format, 188(76.1%) had a nursing assessment for the patients, and out of the charts with a nursing assessment, almost two-thirds (63.2%) had an assessment that was completed within 8 hours of patient admission. Similarly, from the 247 charts that had attached the nursing care plan format, almost three-fourths (188, 76.1%) had the nursing diagnosis, nursing plans, and nursing interventions. Out of the charts with the nursing diagnosis, plans, and intervention, 136 (72.3%), 126 (67%), and 127 (67.6%) were completely documented, respectively. Moreover, out of the 247 charts that had attached the nursing care plan format, 141 (57.1%) had completed the nursing evaluation. But out of the total 372 reviewed charts, almost half (184, 49.5%) had no nursing assessment, diagnosis, plans, and intervention.
On the other hand, among all the charts reviewed, almost all (353, 94.9%) had attached a vital sign sheet, and out of those charts with a vital sign sheet, almost all (341, 96.6%) had documented vital sign components completely. Among all the reviewed charts, 236 (63.4%) nursing records were legible, dated, and signed (Table 4).
Documentation Practices of Nurses Working in Selected Public Hospitals, Central and North Gondar Zone, Ethiopia, 2022.

Factors Associated With Nursing Care Documentation
According to bivariable analysis, good knowledge, favorable attitude, educational level, years of experience, monthly income, motivation from supervisors, adequacy of documentation sheets, adequacy of time, familiarity with the operational standards of nursing documentation, availability of documentation guidelines, adequacy of nurse-to-patient ratio, in-service training attended regarding documentation, negative attitude of the patient toward nurses, and stress, pain, and distress of the patient were found to have a P-value of ≤ .25 subsequently; these variables were entered into the multivariable analysis.
Based on the findings from the multivariable binary logistic regression, in this study, nurses who had good knowledge and those who had favorable attitudes toward nursing care documentation were almost four times (AOR = 4.16, 95% CI: [2.36–7.33]) and three times (AOR = 3.43, 95% CI: [1.85–6.36]) more likely to practice good nursing care documentation compared to their counterparts, respectively. Nurses who were providing care for five or fewer patients per shift were almost three times (AOR = 2.78, 95% CI: [1.13–6.84]) more likely to have good nursing care documentation practice compared to those who provided care for six or more patients. Similarly, the respondents who had adequate time and adequate documenting sheets were almost four times (AOR = 3.85, 95% CI: [2.11–7.05]) and two times (AOR = 2.02, 95% CI: [1.14–3.59]) more likely to perform good nursing care documentation than those reported lack of time and lack of documentation sheets, respectively.
Additionally, the respondents who cared for patients who had no stress, anxiety, pain, and distress were almost four times (AOR = 3.56, 95% CI: [1.69–7.52]) more likely to have good nursing care documentation practice compared to their counterparts (Table 5)
Bivariable and Multivariable Logistic Regression Analysis Results in Selected Public Hospitals, Central and North Gondar Zone, Ethiopia, 2022.

Note: COR = crude odds ratio; AOR = adjusted odds ratio; CI = confidence interval.
*P-value < .05, **P-value < .01, ***P-value < .001.
Discussion
This cross-sectional study assessed nursing care documentation practices and associated factors among nurses in Ethiopia's Central and North Gondar zones public hospitals. Accordingly, the nursing care documentation practice of nurses was poor through chart review compared to the health sector transformation in quality standards. In this study, only 30.4% (95% CI: 25.7%–35.3%) of nurses have good nursing care documentation practice. In our context, poor documentation practice is too bold, which will lower the quality of patient care, put healthcare workers and institutions at risk of medical malpractice claims, and harm patient outcomes. Nurses’ credibility will be altered, and they won’t be able to demonstrate their level of performance. This will have an impact on how their future careers evolve (Kebede et al., 2017). More importantly, this substandard documentation practice is associated with prolonged hospital stays of the patients and increased patient mortality (Mathioudakis et al., 2016; Rossetti et al., 2013; Rothman et al., 2012). This finding is consistent with a study done in Indonesia (Motea et al., 2016), Iran (Aghdam et al., 2009), and European hospitals (Ausserhofer et al., 2014).
In contrast, this finding was lower than the results of the studies conducted in Jamaica (Blake-Mowatt et al., 2013), Yemen (Alhawri et al.), Nigeria (Taiye, 2015), West Gojjam zone (Andualem et al., 2019), and Tigray public hospitals (Tasew et al., 2019). The possible reasons for this discrepancy might be due to differences in workload and differences in familiarity with documentation guidelines because Jamaican nurses have a relatively low workload and are familiar with documentation guidelines compared to Ethiopia. There is a piece of evidence reporting that highly work-loaded nurses have poor nursing care documentation practice as compared to their counterparts (Andualem et al., 2019; Tasew et al., 2019). Another possible reason for the discrepancy might be due to the difference in data collection methods because the current study used a checklist, but the previous study in Yemen used a self-administered questionnaire to collect data, which may cause the documentation practices to be overestimated due to social desirability bias. In fact, data collected using a self-administered questionnaire are vulnerable to social desirability bias compared to those collected using a checklist. Another possible explanation for the discrepancy is the different cut-off points used in the research. This study employed a threshold of 100% as the cut-off point to indicate good documentation practice, but other studies conducted in West Gojjam and Tigray used mean.
The finding of this study was higher than the findings of the studies in Canada (Voyer et al., 2014) and Iran teaching hospitals (Jasemi et al., 2013). This contrary might be due to that the current study included both short and long-term care, but a previous study in Canada was conducted only on long-term care. Another possible reason for the contrary might be due to the differences in the size of the study samples and the number of departments included in the study. The current study included almost all wards from each hospital, but the study from Iran included study subjects only from medical-surgical wards (Jasemi et al., 2013).
In this study, the associated factors with nursing care documentation were also identified. Hence, the likelihood of having good documentation practice for nurses with good knowledge was high compared to those with poor knowledge. This result was supported by studies in Iran (Bijani et al., 2016), Nigeria (Taiye, 2015), Uganda (Nakate et al., 2015), and Addis Ababa (Hailu, 2017). This is possibly explained as knowledgeable nurses can have an awareness of how much documentation is important for good health outcomes. Also, they might be familiar with operational standards/guidelines and ask the responsible body to access the necessary documentation materials, which potentially increases their documentation practice. There is evidence that stated nurses who are familiar with documentation operational standard and guidelines have a good documentation practice (Hailu, 2017). Similarly, this study finding indicated that nurses with favorable attitudes toward nursing care documentation were more likely to have good nursing care documentation practice than those nurses who had unfavorable attitudes. This finding was consistent with the findings of studies in West Gojjam (Andualem et al., 2019) and Addis Ababa (Hailu, 2017). The possible explanation might be that nurses who were interested in their profession and nursing care documentation enhanced their nursing care documentation practice.
Another finding of this study was nurses who reported a shortage of time were less likely to have good nursing care documentation compared to nurses who had adequate time, which was supported by the study findings from Iran (Bijani et al., 2016), Jamaican hospitals (Blake-Mowatt et al., 2013), West Gojjam (Andualem et al., 2019), and Addis Ababa (Hailu, 2017). The explanation might be the fact that the comprehensive nursing care documentation practice needs sufficient time/low workload of nurses. There is evidence that reported nurses need sufficient time and low workloads to perform nursing documentation (Tasew et al., 2019).
Our study also showed that inadequate nursing documentation practice is negatively impacted by a lack of documentation formats, which was also confirmed by the studies done in Addis Ababa (Hailu, 2017) and Tigray (Tasew et al., 2019). Additionally, an adequate nurse-to-patient ratio was positively associated with good nursing documentation practice. This finding is consistent with the findings of the studies conducted in Western Jamaica (Blake-Mowatt et al., 2013), Eastern Ghana (Asamani et al., 2014), and Eastern Ethiopia (Tamir et al., 2021). This may be because nurses may have less work to complete and more time to document their activities with a lower nurse-to-patient ratio, which increases the likelihood that their documentation practice is good (Twigg et al., 2021). This implies how crucial it is to have a sufficient nursing workforce. Moreover, the respondents who cared for patients who had no stress, anxiety, pain, or distress were 3.56 times more likely to have good nursing care documentation practice compared to their counterparts. This finding is supported by the studies conducted at Debremarkos and Finoteselam hospitals (Abebe et al., 2014). This might be because patients are the primary data source, and patients with stress, anxiety, pain, and distress are not willing to give data for nursing care documentation. There is a piece of evidence that reported that patients coming with complicated complaints are not willing to give data for nursing documentation (Tadessa et al., 2017).
Strengths and Limitations
One potential strength of this study is the multicentral level at which it was carried out. As a limitation of this study, each study participant's nursing care documentation practice was measured by one randomly selected patient chart that was only documented by each study participant and from his/her bed distribution. The chosen chart may have been less representative of other charts even though the selection process was completely random. Moreover, the absence of the length of stay (LOS) variable in our study limits our ability to analyze its potential impact on the documentation practice. Future studies incorporating LOS data could offer a more comprehensive understanding of its influence on it.
Implication for Practice
The study's findings imply that nursing care documentation practices need a great deal of attention, necessitating interventions from a variety of stakeholders. Health institutions better provide sustained continuing training opportunities for nurses to enhance their knowledge and favorable attitudes regarding documentation. Hospitals also need to consider admitting patients who are stressed, anxious in pain, or distressed on high-dependency units or something similar, which requires a lower nurse-to-patient ratio and ultimately enhances nursing care documentation. Moreover, nursing leaders (matrons/nursing directors) better motivate and enhance the attitudes of nurses and avail the necessary documentation materials.
Conclusion
The nursing care documentation practice of nurses was poor compared to the health sector transformation in quality standards. This could cause incomplete records for further intervention and patient monitoring, poor service quality, inadequate information to show the work that nurses are contributing, and hinder professional and institutional growth that subsequently hampers patient outcomes. Favorable attitude toward nursing documentation, good knowledge of nursing documentation, lower nurse-to-patient ratio, adequacy of documenting sheets, adequacy of time, and caring patients who had no stress, anxiety, pain, and distress had a statistically significant positive association with nursing care documentation practice. Therefore, this study concludes that nursing care documentation practice remains a challenge. So, it is better to put further effort into improving nursing care documentation practice.
Footnotes
Acknowledgments
The authors would like to thank the study participants, data collectors, and supervisors who were involved in this study.
Author Contribution
FM, WA, and SK conceived and designed the study. DE and FM performed the analysis and write-up of the study. DE prepared the manuscript for publication, and all authors critically reviewed the initial draft of the manuscript. All authors read and approved the final manuscript.
Data Availability
All data generated or analyzed during this study are included in this published article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.