
Abstract
Background
Despite free maternal healthcare, about 50% of pregnant women in Ghana initiate their antenatal clinic (ANC) late.
Aim
This study aimed to identify the factors that contribute to the late initiation of ANC among pregnant women in the Jasikan District, Ghana.
Method
A cross-sectional study was conducted between December 2021 and May 2022 in multiple health facilities. Multistage sampling was employed to select 352 pregnant women attending ANC in selected health facilities. A structured questionnaire was used to collect the data. The data was analyzed using Stata version 14.0. Descriptive statistics was used to describe the study variables and multivariable logistic regression models were performed to determine the predictors of late ANC initiation at p < .05 and 95% confidence interval (CI).
Results
Approximately 45.7% of the participants initiated ANC late. Age less than 20 years, older age groups (40–49 [odds ratio (OR): 18.0, 95%CI: 3.68–88.0, p < .001]; 30–39 [OR: 6.4, 95%CI: 1.76–22.87, p = .005] and 20–29 [OR: 4.6, 95%CI: 1.30–15.98, p = .018]) were associated with late initiation of ANC. Having a higher number of children (4 [OR: 2.8, 95%CI: 1.36–5.79, p = .005] and 3 [OR: 2.5, 95%CI: 1.33–4.58, p = .004]) were predictors of late ANC initiation as compared to having one child. Women who sought for advice from women leaders (OR: 3.5, 95%CI: 1.18–10.12, p = .02) were about three (3) times more likely to initiate ANC late as compared to those who sought for advice from friends. Women who felt poorly received at ANC (OR: 7.7, 95%CI: 2.188–27.078, p = .001) were about eight (8) times more likely to initiate ANC late as compared to those who felt well received. Again, those who spent over six (6) hours during ANC visits (OR: 18.4, 95%CI: 4.246–79.734, p < .001) had an 18 times higher risk of initiating ANC late relative to those who spent less than 3 h.
Conclusion
The study findings highlight the need for interventions that addresses the social and cultural factors, negative perceptions of ANC, and long waiting times at health facilities to improve early initiation of ANC. Such interventions can assume health education and promotion to address the sociocultural and unfavorable perceptions toward ANC. The sector ministry and the health facilities may consider expanding ANC service centers to reduce long waiting times.
Introduction
Reducing maternal and neonatal mortalities are major global health priorities and top targets on the Sustainable Development Goal (SDG) 3.1 and 3.2 (UNSD & DESA, 2 017). The SDG target 3.1 entreats countries to aim at reducing maternal mortality ratio to 70 per 100,000 live births by 2030 and the SDG 3.2 is aimed at reducing neonatal mortality to at least 12 per 1,000 live births and under-5 mortality to at least 25 per 1000 live births by 2030 (UNSD & DESA, 2017). However, maternal and neonatal mortalities remain unacceptably high with global estimates of 0.3 million maternal deaths and 2.4 million neonatal deaths in 2020 (Boerma et al., 2023). Majority of maternal and neonatal mortality are reported from lower- and middle-income countries (maternal mortality ratio (MMR) of 479) as compared to high-income countries (MMR of 41) (Bauserman et al., 2020). A key strategy to resolve maternal and neonatal mortalities globally is through appropriate antenatal care (ANC) service initiation and uptake during pregnancy (Mlandu et al., 2022; Oduro et al., 2023). ANC is a special care that is provided for pregnant women to improve the health of the unborn baby and the mother (World Health Organization [WHO], 2018). According to WHO's recommendation, every pregnant woman should register for ANC before 12 weeks of gestation. Early initiation of ANC has the benefit of early detection and treatment of complications during pregnancy (WHO, 2019). Several studies have shown that late initiation of ANC (i.e., after 12 weeks) is a significant risk factor for maternal deaths (Lattof et al., 2019; WHO, 2016). The Ghana Health Service (GHS) also recommends that the first ANC attendance should preferably be in the first trimester for timely identification of problems and management, giving appropriate advice to protect the mothers’ health and fetus’ optimal development for best pregnancy outcomes (GHS, 2019; Pell et al., 2013). Early initiation of prenatal care by pregnant women and continuous monitoring of pregnancy by healthcare providers are key to helping in preventing and treating severe pregnancy-related complications (Krukowski et al., 2022; Woldesenbet et al., 2022).
Evidence has shown that providing timely and appropriate ANC leads to a reduction in maternal deaths (WHO, 2016). The burden of maternal mortality is high in developing countries, accounting for 99% of the global maternal deaths, with the sub-Saharan African (SSA) region contributing 66% of the mortality (Tessema et al., 2021). Most of the causes of maternal deaths are preventable, detectable, and treatable. Immediate action is however, needed to meet the ambitions of SDG 2030 for eliminating preventable causes of maternal death with special attention on SSA (Kassebaum et al., 2016; Tessema et al., 2021). Many low- and middle-income countries (LMICs) are using social health insurance schemes to increase access to maternal health services. In Ghana, pregnant women enroll in the National Health Insurance Scheme (NHIS) without paying premium and registration fees and have free access to the ANC and other services. The NHIS was introduced by government in 2004 to improve access to healthcare. It operates as a national system of service provision and financing without co-payment and requires an annual payment of registration fee of GHC 5.00 (about US$0.5 and GHC 30.00 (about US$3.00) as premium (National Health Insurance Authority [NHIA], Ghana-National-Health-Accounts-2005-2010, 2010; Kotoh & Boah, 2019).
Healthcare services including medicines are obtained from accredited public health, quasi-government, and some private health facilities, pharmacies, and chemist shops, which operate under contract with NHIA (Kotoh & Boah, 2019). With the free access to ANC and the expansion of health services especially Community-based Health Planning and Services (CHPS) compounds nationwide, it is expected that all pregnant women will initiate ANC early but this unfortunately has not happened. Although statistical data on late ANC initiation in the Oti Region is available in the District Health Information Management Systems (DHIMS II), the predictors of late ANC initiation over the years have not been empirically established in the Region. This study therefore was aimed at determining the predictors of late ANC initiation in the Jasikan District, in Oti Region of Ghana. Despite the modest gains from maternal and child healthcare interventions across the world, reproductive health issues remain a global challenge, particularly in developing countries. It is estimated globally that, more than 300,000 women died out of pregnancy or childbearing-related conditions in 2015, with about 3 million neonatal deaths and 2.6 million stillbirths (National Institutes of Health, 2019; Verstraeten et al., 2015; Welaga et al., 2017). A study conducted in Shai-Osudoku and Ningo-Prampram Districts of the Greater Accra Region of Ghana on factors associated with the timing of antenatal clinic attendance among first-time mothers found that, 43% registered late (Manyeh et al., 2020). A cross-sectional study, conducted in Northern Ghana, revealed that of the 431 participants, 8.9%, 8%, 25.4%, 45.3%, and 10.7% started ANC in the first, second, third, fourth, and fifth months of pregnancy, respectively, and this clearly shows that majority of them reported late (Kotoh & Boah, 2019). A similar trend was observed in the Volta Region where over 45% of all pregnant women reported late for ANC between 2018 and 2021 (Jasikan District Health Directorate report, District Health Information Management Systems, 2021). Facility data show that in 2019 and 2020, 3 and 4 maternal deaths were recorded, respectively. Also, in 2019 (0.62%), 2020 (0.97%), and 2021 (1.3%) of still births were recorded in the Jasikan District (DHIMS II, 2021). In Jasikan District, 2018 (49%), 2019 (47%), 2020 (40%), and mid-2021 (45%) of pregnant women being reported late for ANC (Jasikan District Health Directorate report, 2021). The factors that influence the late initiation of ANC have not been fully explored in the Oti Region of Ghana. The study therefore aimed at assessing the predictors of late ANC initiation in the Jasikan District, Oti Region, Ghana. Findings from the study will be beneficial for ANC planning and decision making in the study setting.
Literature Review
Globally, approximately 88% of pregnant women access ANC with a skilled healthcare worker at least once and 2 in 3 (69%) have at least four visits for the duration of the pregnancy (United Nations International Children's Emergency Fund, 2019). The WHO recommends eight ANC visits by pregnant women (United Nations International Children's Emergency Fund, 2019). ANC is recommended as a strategy to achieving the targets 3.1 and 3.2 of the SDG-3 by 2030. ANC service uptake and utilization has been associated with reduced pregnancy adverse outcomes and the provision of essential pregnancy services such as pregnancy care and health promotion, vitamin supplementation, infection screening, and counseling on healthy eating habits (United Nations International Children's Emergency Fund, 2019; Yu et al., 2013; Zeleke et al., 2022). Timely initiation of ANC is a major component of the ANC services and is recommended that pregnant women visit the ANC in the first trimester of pregnancy and usually before 12 weeks of gestation (Amoako & Anto, 2021; Tolossa et al., 2020). Initiation ANC early is known to enhance early detection and treatment for all pregnancy complications, provision of optimal care for pregnant women and the fetus (Dorji et al., 2019). The timely initiation of ANC allows for the early identification of pre-existing health conditions such as hypertensive disorders of pregnancy, sexually transmitted infections, and HIV, malaria in pregnancy, and anemia (Amoako & Anto, 2021; Oduro et al., 2023; Tolossa et al., 2020; Zeleke et al., 2022). Despite the benefits of early ANC initiation, previous studies, and reports continue to show late initiation of ANC service utilization by pregnant women across many regions of the world. Current evidence suggests that pregnant women who do not fully utilize ANC services do not fully benefit the intended purpose of ANC and do not receive all the required necessary care (Bauserman et al., 2020; Fenta et al., 2021; Mlandu et al., 2022). The late ANC initiation by pregnant women predisposes them and the developing fetuses to adverse pregnancy health outcomes (Wolde et al., 2018; Zeleke et al., 2022). For example, available evidence suggests that pregnant women with untreated HIV and Syphilis have a 70% to 100% chance of transmitting the infection to their fetus (Akhtar & Rehman, 2018; Gomez et al., 2013; Zeleke et al., 2022). About 15% pregnant women with untreated syphilis had clinical evidence of congenital syphilis (Akhtar & Rehman, 2018; Gomez et al., 2013; Zeleke et al., 2022).
The coverage of early ANC initiation is nearly 43% globally with significant disparities exist between high income countries (HICs) and LMICs (Gomez et al., 2013; Zeleke et al., 2022). In HICs, approximately 85% of pregnant women initiate ANC early in the first trimester compared to 45% of pregnant women LMICs (Gomez et al., 2013; Zeleke et al., 2022). In SSA countries early ANC coverage is nearly 25% (Moller et al., 2017). Demographic and Health Survey reports across SSA shows that early initiation of ANC ranges between 17.6% and 34% (Zeleke et al., 2022). The early ANC coverage in LMICs and SSA is unacceptably low, especially at a time where countries have less than a decade to meet the SDGs. Understanding the localized and national determinants of late ANC initiation is important to the design and development of targeted interventions. The predictors of late ANC initiation as emphasized in previous studies include age, parity, marital status, wealth, ANC timing, insurance cover, and cost of ANC services (Sakeah et al., 2014). Some studies have equally found factors as educational level, religion, ethnicity, area of residence, and transportation as important contributors to pregnant women's decision regarding ANC initiation and attendance (Sakeah et al., 2014). Other studies have also implicated poor male involvement in ANC services (Morgan et al., 2022; Muia et al., 2022). Some sociocultural practices and belief in supernatural forces has the potential to prevent early disclosure of pregnancy and may limit the chance of seeking early focused ANC (Baffour-Awuah et al., 2015).
The healthcare system equally plays a significant role in early ANC service initiation and uptake. A pregnant woman's decision to seek and initiate early ANC may extend beyond a matter of personal preference; the accessibility of services that either facilitate or impede utilization has an important influence (Ngongo, 2016). As outlined by the WHO, access to ANC services consists of several elements, including distance and/or time to a facility, the physical availability of services, cultural and social factors that may impede access, economic and other costs associated with the use of services, and the quality of the services offered (WHO, 2019). Some previous studies have shown that the health facility-related factors for ANC service initiation and uptake comprised unavailability of medications and skilled health workers, poor attitude, and unprofessional conduct of the health workers (Sinyange et al., 2016).
Materials and Methods
Study Design and Site Description
A multicenter health facility-based cross-sectional study was conducted between December 2021 and May 2022 to determine the predictors of late ANC initiation among pregnant women in the Jasikan District, Oti Region, Ghana. The study was conducted and reported in line with the STROBE checklist for cross-sectional studies. The data was collected using a pretested structured questionnaire among women who started ANC within the survey period from randomly selected health facilities. The Jasikan District is located in the southern sector of Oti Region of Ghana. It is bounded by three Districts and the Republic of Togo. In the south, by the Hohoe Municipality of Volta Region and Biakoye District of Oti region, in the north; by Kadjebi District of Oti region, in the west, by Biakoye District of Oti region and in the east by the Republic of Togo.
The District has a population of 60,949 according a recent population and housing census. The number of communities served is about 63 excluding numerous settled farming communities in the cocoa-growing land. The main occupation of the people is farming, trading, Kente weaving, and civil service.
There are 28 demarcated CHPS zones with 18 functioning CHPS compounds. Also, there are seven Health Centers comprising of six government and a private and a District Hospital.
Study Population
The study included confirmed pregnant women aged 15 to 49 years and resident in the Jasikan District, Oti Region, Ghana.
Inclusion and Exclusion Criteria
Inclusion Criteria
The inclusion criteria were:
Confirmed pregnant women in the Jasikan District who registered and were coming for ANC within the survey period. Pregnant women who have been residing in the District for more than 6 months and coming for ANC for the first time or subsequent visit. Pregnant women under 18 years of age who assented to be part as well as seeking their parents’ consent. Pregnant women aged 18 years and above who consented (written) to and volunteered to be part of the study.
Exclusion Criteria
The exclusion criteria were:
Pregnant women who were critically ill and physically or mentally disabled during the data collection period were excluded from the study.
Sample Size Determination
The sample size was calculated using Cochran's formula (Cochran, 1963) based on the following parameters: The proportion (P) of late initiation of ANC = 43% which was taken from a previous in Ghana (Manyeh et al., 2020). At 95% confidence level of Z α/2 = 1.96, and 5% of absolute precision, n = sample size.
The sample size of this study was determined as follows:




Therefore, using the finite population correction factor in the determination of the sample size (Berenson et al., 2013),





Sampling Procedure
Multistage sampling technique was used to select the final sample of the respondents in the study.
Sampling of Subdistricts
At the first stage, sampling was from the clusters (subdistricts). This was done by writing the names of the subdistricts on pieces of paper and folded and dropped in a basin. Four subdistricts were then selected from the total number of subdistricts in the district by a neutral person using simple random sampling without replacement technique until the required number was attained.
Sampling of Health Facilities
At the second stage, a total of 10 health facilities were selected using a simple random sampling technique by writing the names of all the health facilities on pieces of paper and mixed thoroughly and kept in a container. A neutral person was asked to select until the required number was attained based on the number of facilities in each subdistrict.
Sampling of Pregnant Women
Antenatal mothers attending ANC services were selected using simple random sampling technique. The data collection took place at the ANC clinics of the various facilities. The average ANC attendance was obtained from the health facilities. Sample sizes were then allocated proportionately to the selected health facilities based on the average ANC attendance. A list of all ANC registrants for each facility were obtained (sampling frame). Once the sampling frame was obtained, the number of antenatal mothers needed to be surveyed from each facility was known.
Two responses, “Yes” and “No” were written on pieces of paper and then folded. The folded pieces were placed in a basin and mixed with the hands to ensure that the mixing of the papers was uniform. The number of “yes” were equal to the number of antenatal mothers required to be sampled from each facility and the number of “no” were equal to the number remaining after subtracting the required number of antenatal mothers from the total number at each facility. All eligible antenatal mothers were allowed to randomly pick the papers from the basin. Those who picked “yes” and consented to participate in the study were involved in the study. In a situation where the number of antenatal mothers were less than or equal to the number of antenatal mothers required, all those present at the ANC clinic on the day of data collection were enrolled and interviewed upon consenting. The same procedure was repeated until the required number of participants was attained in each facility.
Data Collection Procedure
Data was collected using a structured interviewer-administered questionnaire to solicit information from participants on their sociodemographics, cultural barriers, and health system factors of antenatal care services. Secondary data on ANC initiation was collected using the ANC booklet. The questionnaire used in the data collection was derived from related questions used in similar studies (Mamba et al., 2017; Pell et al., 2013). Four research assistants were trained on the various components of the questionnaire and ethical issues relating to the study upon which they assisted in the data collection process.
Study Variables
The independent variables in this study was the sociodemographic characteristics of the participants and they included: age, educational level, number of children, marital status, religion, ethnicity, occupation, family size, and monthly income.
The dependent variable was the late initiation of ANC among pregnant women in the Jasikan Municipality.
Pretesting
The questionnaire was pretested on 5% of the total sample size in the ANC clinic at Kedjebi District with similar characteristics as the Jasikan District to ascertain the validity and reliability of the tool before the actual data collection for the study. This helped to provide useful feedback for the revision of the questionnaire.
Data Management and Analysis
The data was cleaned to ensure quality and accuracy. The data was recorded using the Epi Data manager version (4.6.0). Data analysis was done using the STATA (version 14.0). To maintain safety and confidentiality, the data was backed up, and password protected. The data were presented in tables and figures. Simple frequencies, percentages, and cross-tabulation using the Chi-square test was used for categorical variables. Binary logistic regression (95% confidence interval [CI] and p-value) analysis was used to determine the strength of the association between independent variables and the outcome. All factors associated with late ANC with p-value < .05 were considered statistically significant and were included in the multivariable logistic regression model.
Ethical Consideration
Ethical approval for this study was obtained from a research ethics committee of a public University. Permission was sought from the health directorate, and the selected health facilities in the District. Informed consent was obtained from participants prior to participation. Confidentiality/anonymity was ensured by not taking the names or any information to identify a participant in the questionnaire. Participants were assured of confidentiality and anonymity that their names and other details would not be linked to the data analysis and dissemination of findings of the study under any circumstance. All the participants were informed that the study was voluntary, and anyone could decide to withdraw from the study at any point in time without any fear or favor.
Also, there was a possibility that participants were at risk of COVID-19 by participating in the study. However, the data collectors were trained sufficiently to ensure strict observance of COVID-19 preventive protocols. Any item that was used for responding to the questionnaire was sanitized before and after usage. Also, appropriate social distancing protocols were observed. There were no direct benefits or risks for participating in this study. There was no form of monetary payment or other forms of compensation for participating in the study.
Results
Sociodemographic Characteristics of Study Participants
A total of 352 pregnant women took part in the study of which 58.5% (206) were aged 20 to 29 years. Among the participants, 36.4% (128) had at least 2 children and 13.4% (47) had at least 4 children. On marital status, 65.9% (232) were married at the time of the study. Among the participants, 41% (144) had primary education and 31.3% (110) were traders. Most of the 62.2% (219) participants were Christians and 41.8% (147) belonged to the Ewe ethnic group. Also, 73.3% (258) had a monthly income below GH¢1000 (Ghana cedis) and 52.3% (184) had a family size of 4 to 6 persons per household (Table 1).
Sociodemographic Characteristics of Study Participants.

Initiation of Antenatal Care
On ANC initiation, 45.7% initiated ANC late (Figure 1).

Antenatal clinic initiation.
Sociodemographic Predictors of Late ANC Initiation Among Pregnant Women
Some sociodemographic factors were associated with late initiation of ANC. Relative to age less than 20 years, older age groups (40–49 [odds ratio (OR): 18.0, 95%CI: 3.68–88.00, p < .001]; 30–39 [OR: 6.4, 95%CI: 1.76–22.87, p = .005], and 20–29 [OR: 4.6, 95%CI: 1.30–15.98, p = .018]) were associated with late initiation of ANC. Having a higher number of children (4 [OR: 2.8, 95%CI: 1.36–5.79, p = .005] and 3 [OR: 2.5, 95%CI: 1.33–4.58, p = .004]) were predictors of late ANC initiation as compared to having one child. Those who were not married (OR: 0.5, 95%CI: 0.34–0.85, p = .008) were less likely to initiate ANC late relative to those who were married. On religious grounds, Muslims (OR: 1.99, 95%CI: 1.28–3.10, p = .002) were more likely to initiate ANC late as compared to Christians. Also, compared to having no formal education, those who had primary (OR: 0.3, 95%CI: 0.15–0.63, p = .001), secondary (OR: 0.3, 95%CI: 0.16–0.67, p = .002) and tertiary levels of education (OR: 0.3, 95%CI: 0.11–0.61, p = .002) were less likely to initiate ANC late (Table 2).
Sociodemographic Predictors of Late ANC Initiation Among Pregnant Women.

Note. ANC: antenatal clinic; CI: confidence interval; COR: crude odds ratio.
Cultural Barriers That Predict Late ANC Initiation Among Pregnant Women
Those who sought for advice from women leaders (OR: 3.46, 95%CI: 1.18–10.12, p = .02) were more likely to initiate ANC late as compared to those who sought for advice from friends. Also, those whose pregnancy was approved by husband and family (OR: 0.12, 95%CI: 0.01–0.95, p = .045) and those whose husbands approved their initiation of ANC (OR: 0.12, 95%CI: 0.01–0.95, p = .045) were less likely to initiate ANC late (Table 3).
Cultural Barriers That Predict Late ANC Initiation Among Pregnant Women.
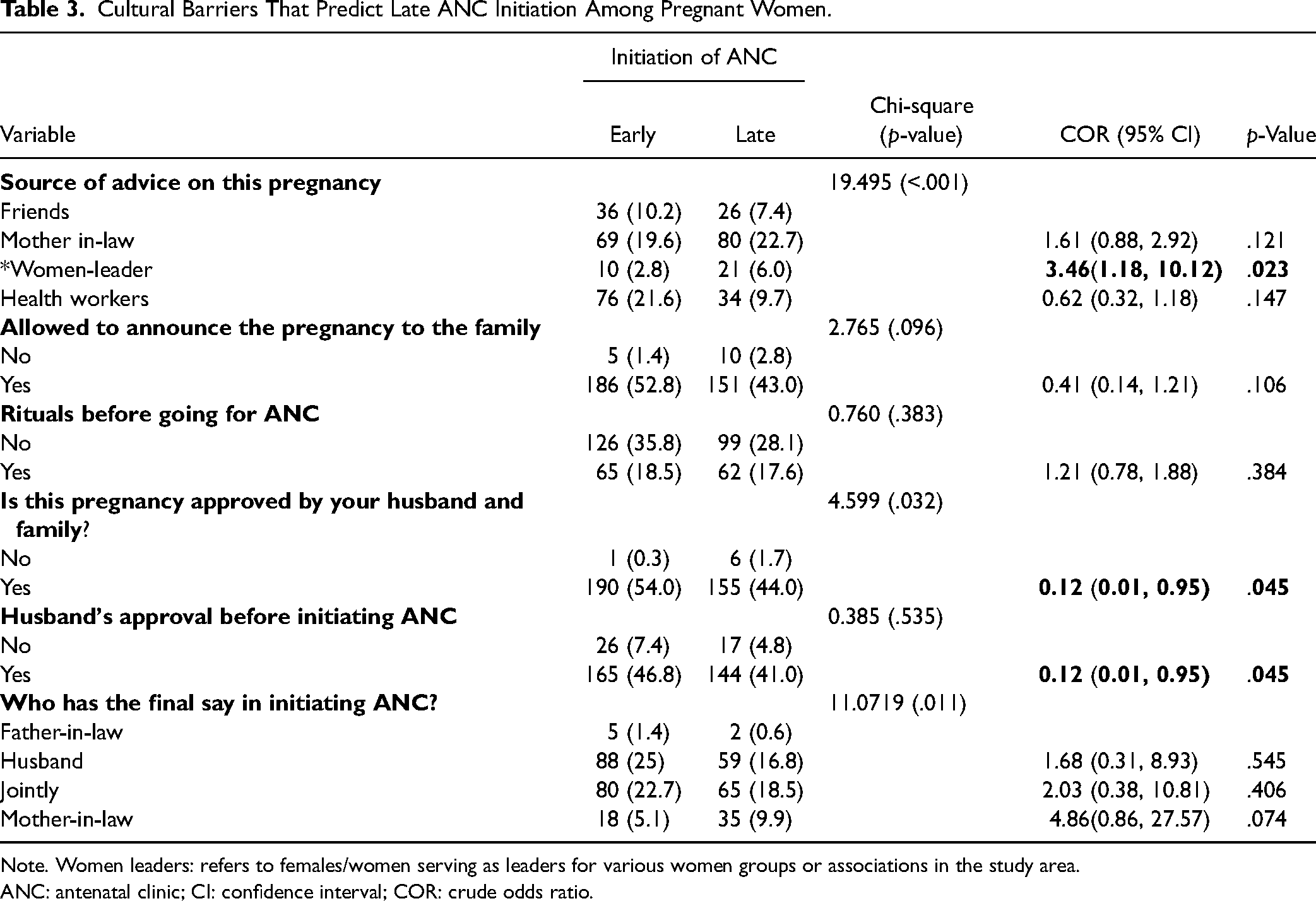
Note. Women leaders: refers to females/women serving as leaders for various women groups or associations in the study area.
ANC: antenatal clinic; CI: confidence interval; COR: crude odds ratio.
Health Systems Predictors of Late ANC Initiation Among Pregnant Women
Respondents who affirmed that health workers communicated with them freely and allowed questioning during ANC (OR: 0.2, 95%CI: 0.626–0.606, p = .005) were less likely to initiate ANC late as compared to those who posited otherwise. Also, those who felt poorly received at ANC (OR: 7.7, 95%CI: 2.188–27.078, p = .001) were more likely to initiate ANC late as compared to those who felt well received. Those who spent over 6 h (OR: 18.4, 95%CI: 4.246, 79.734, p < .001) and between 3 and 5 h (OR: 2.1, 95%CI: 1.22, 3.61, p = .008) during ANC visits were more likely to initiate ANC late relative to those who spent less than 3h. Moreover, respondents who agreed that health workers related with them sometimes friendly (OR: 2.5, 95%CI: 1.578, 3.882, p < .001) were more likely to initiate ANC late as compared to those who posited that health workers were always friendly (Table 4).
Health System Predictors of Late ANC Initiation Among Pregnant Women.

Note. ANC: antenatal clinic; CI: confidence interval; COR: crude odds ratio.
Multivariate Results of All Predictors of Late ANC Initiation
In a multiple regression analysis, those who were not married (adjusted OR [AOR] = 0.5, 95% CI 0.26–0.79, p = .005) were less likely to initiate ANC late as compared to those who were married. Again, those who had secondary education (AOR = 0.3, 95% CI 0.10–0.62, p = .003) and tertiary education (AOR = 0.2, 95% CI 0.05–0.49, p = .001) were respectively less likely to initiate ANC late relative to those who had no formal education. Also, those who sought advice from women-leaders during the pregnancy (AOR = 4.8, 95% CI 1.42–15.87, p = .011) were more likely to initiate ANC late relative to those who sought advice from friends. Moreover, those who had perception of poor reception at ANC (AOR = 8.8, 95% CI 2.08–37.15, p = .003) were more likely to initiate ANC late as compared to those who had perceived good reception by health workers at ANC and those who encountered delays over 6 h at ANC (AOR = 11.5, 95% CI 2.37–55.51, p = .002) were more likely to initiate ANC late as compared to those who spent less than 3 h during ANC (Table 5).
Multivariate Results of All Predictors of Late ANC Initiation.

Note. ANC: antenatal clinic; AOR: adjusted odds ratio; CI: confidence interval; COR: crude odds ratio.
Discussion
In this study, late initiation (first ANC visit after 12 weeks of gestation) of ANC was 45.7% among pregnant women in the Jasikan District. The finding reinforces reports of other studies that have found that many pregnant women initiate ANC late in Ghana. A similar study by Nonterah et al. (2019) reported that 49.0% of the pregnant women initiated ANC late in Navrongo, Upper West Region, Ghana. Similar studies conducted in Accra (Manyeh et al., 2020) and Yendi Municipality (Ziblim et al., 2018) also revealed that 43% and 57% of mothers booked ANC after 12 weeks of gestation, respectively. In the Ashanti Region of Ghana, a study reported that in 2019 to 2021 the Ahafo Ano South West District showed a marked burden of late ANC booking with 55% of pregnant women initiation ANC in the second and third trimesters of pregnancy in 2019. The proportion of late initiation of ANC in the District significantly declined to 48% in 2020 and 2021(Oduro et al., 2023). The current study's finding of late ANC initiation and that of the related studies shows that more work needs to be done to achieve the quest for early initiation of ANC. With the exception of Manyeh et al. (2020) study which has urban characteristics, the current study, Ziblim et al. (2018) and Oduro et al. (2023) are of peri-urban characteristics. Studies in other African countries show that pregnant women initiate ANC late with 42.2% in Ethiopia and 28.0% in South Africa (Ebonwu et al., 2018; Tufa et al., 2020). Though the observed differences in the late initiation of ANC service uptake and utilization by pregnant women may not be wide, however the findings underline the universality of the problem (late ANC initiation) in Ghana and may have adverse implication on maternal health outcomes including anemia in pregnancy, malaria in pregnancy preterm births and maternal mortality(Gebrekidan & Worku, 2017). Addressing late initiation of ANC should be of concern to everyone to be able to reduce maternal and neonatal mortalities in Ghana and across the globe.
In this study, certain sociodemographic factors including marital status (married) and educational level (no education) were associated with late ANC initiation. The reason might be high chance of not exposed to information in case of noneducated mothers. Those who were not married were less likely to initiate ANC late as compared to those who were married. This finding is somewhat surprising, as a previous study found that unmarried women were more likely to attend ANC regularly (Sakeah et al., 2014). This finding is consistent with a previous study that found that married women in South Africa were more likely to initiate ANC late (Ebonwu et al., 2018). The reason for this difference may be that married women are more likely to seek support and approval from their partners before initiating ANC as compared to unmarried women. Women who had higher levels of education were more likely to initiate ANC early. This finding is consistent with a previous study that found that women with higher levels of education were more likely to attend ANC regularly (Tayie & Lartey, 2008). This finding is consistent with a previous study that found that women with higher levels of education were more likely to attend ANC regularly (Sakeah et al., 2014).
Previous studies have explained the association between sociocultural factors and late ANC initiation (Mlandu et al., 2022; Wolde et al., 2018). In this study we found that late initiation of ANC was associated with seeking advice from women-leaders. Women who sought advice from women-leaders were more likely to initiate ANC late than women who sought advice from friends. This finding is consistent with a previous study that found that some women in Ghana may be hesitant to seek ANC if they are not married or if they have had previous pregnancies outside of marriage (Mamba et al., 2017). This suggests that pregnant women may be more likely to seek advice from people they know and trust, such as friends, family members, or community leaders.
Several factors related to the health system were associated with late initiation of ANC, including poor reception from healthcare providers and long wait times. Women who perceived that they were treated poorly by health care providers were more likely to initiate ANC late. This finding is consistent with a previous study (Nachinab et al., 2019). Some nurses and midwives acknowledged that they both intentionally and unintentionally maltreated pregnant women when providing care (Sumankuuro et al., 2017). The finding of this study may be contextually understood to be that the perception of the attitude of health staff by pregnant women could affect the early ANC initiation and subsequent utilization of ANC services.
Also, those who encountered delays over 6h at ANC were more likely to initiate ANC late as compared to those who spent less than 3 h during ANC. Similar to this finding, Kilowua and Otieno (2019), reported from a study that those who were satisfied with the waiting time were more likely to have attended ANC. This finding could be due to a higher number of ANC attendance at the time of the data collection compared to number of health facilities and staff. The implication of this finding is that, general ANC attendance may as well be affected by delays at service delivery points.
Study Limitations
We acknowledge that this is a cross-sectional study where data was taken at one point in time, therefore, the responses given can vary with time. However, the study provides important information that can be relied on for interventional purposes in the study setting. Again, the study included CHPS compounds, which are important health facilities that provides primary care to smaller communities in Ghana. Therefore, the findings of this study are important to guide the planning of ANC services in rural settings of Ghana.
Implication for Practice
The study presents significant findings that can influence public health and ANC practice. Significant number of respondents initiated ANC late, indicating a major health concern that needs immediate attention. We found important factors that influenced the initiating of ANC late and included age, parity, sources of advice to pregnant women, the duration of the ANC visit and the sort of reception pregnant women receive at ANC. It is important that when government health agencies are designing interventions to address late ANC and encourage pregnant women to initiate ANC early, the identified factors must be paid attention to. For example, our study noted that older women were more likely to initiate ANC late. It is equally not surprising that women with large number of children are likely to initiate ANC late. Interventions such as health education and promotion should be designed to consider the age and parity differences among women seeking ANC services. An interesting finding of the study is the influence of the elderly advice on ANC initiation among pregnant women. This finding could be leveraged on to increase early ANC initiation, and service optimal uptake. However, it is important ascertain the quality of the content of the advice or information the elderly offer to pregnant women on ANC related issues. Deliberate efforts could be made to train significant number of the elderly in communities as health volunteers to offer important health education on pregnancy care. Conventionally, the elderly commands some level of respect in our communities and therefore, using them to promote health could impact the uptake of maternal health services.
Health customer care services have long been known to influence the health seeking behavior of clients. The study found that mother who's experiences at ANC was poor are likely not to initiate ANC early. Again, mothers who spend several hours waiting to receive ANC service(s) are likely to initiate ANC late. These findings may have negative implications on the healthcare seeking behavior of pregnant women. It is important to emphasize the need to reorient the provision of healthcare to a more patient-centered and respectful care approach to improve customer care services and general healthcare seeking behavior. Interventions geared toward the improvement of waiting times is highly recommended. Expanding existing ANC infrastructure and human resources could strategies to reduce the long waiting time periods. However, in the short term, streamlining appointment systems for ANC services could reduce the long waiting periods to improve and promote early ANC initiation for better maternal health outcomes.
Conclusion
The prevalence of late initiation of ANC was high and raises a concern for concerted efforts toward addressing it, taking into consideration the social and cultural factors combined with unfavorable perception toward ANC and delays at service centers. The study underlines a need to carefully design interventions that addresses these factors to maximize ANC service utilization.
Ethical Consideration
Ethical approval for this study was obtained from the University of Health and Allied Sciences (UHAS) Research Ethics Committee (UHAS-REC A.2 [3]21–22). Permission was sought from the Oti Regional Health Directorate, Jasikan District Health Directorate, and subsequently, from the selected health facilities in the District. Copies of the clearance letter and approval to proceed with the study from the University were made available to the appropriate authorities before the start of the study.
Confidentiality/anonymity were ensured by not taking the names or any information to identify a participant in the questionnaire. Participants were assured of confidentiality and anonymity that their names and other details would not be linked to the data analysis and dissemination of findings of the study under any circumstance. All the participants were informed that the study was voluntary, and anyone could decide to withdraw from the study at any point in time without any fear or favor.
Also, there was a possibility that participants were at risk of COVID-19 by participating in the study. However, the data collectors were trained sufficiently to ensure strict observance of COVID-19 preventive protocols. Any item that was used for responding to the questionnaire was sanitized before and after usage. Also, appropriate social distancing protocols were observed. There were no direct benefits or risks for participating in this study. There was no form of monetary payment or other forms of compensation for participating in the study.
Footnotes
Acknowledgments
The authors first of all express their sincerest gratitude to the Almighty God for his continuous blessings and protection, they also acknowledge the priceless contribution of the Heads of Department and staff of the Population and Behavioral Science and Family and community Health. Further they wish to thank the Oti Regional Director of Health, Dr Osei Kuffour Afreh and his team and the Jasikan District Director of Health, Mr. Isaac Anobel for granting us permission to conduct the study in the Jasikan District. Finally, appreciation goes to all who contributed in various ways to make this study see the light of the day.
Authors’ Contributions
JG, EET, and AMT contributed to conceptualization and data collection. JG and EKD were involved in data curative; JG, WAA, and ASH in formal analysis; EET and AMT in project supervision; VA in writing the manuscript; JG, AMT, EKD, JAA, and VA in original draft; and EET, AMT, WAA, and ASH in review and editing. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The authors declare that no potential conflicts of interest exist with respect to the research, authorship, or publication of this article.
Funding
The authors received no financial support for the research, authorship, or publication of this article.