
Abstract
Introduction
Postnatal care (PNC) is critical for the newborn and the mother, as it offers the opportunity to examine the mother and child to ensure early and timely intervention of any obstetric anomalies that might have gone unnoticed during delivery. However, there is a lack of data on PNC utilization and associated determinants in Ghana. Meanwhile, it is suspected that the PNC service should be more patronized by mothers, particularly within the first 2 days after delivery; therefore, investigating PNC utilization and associated factors could inform policies to enhance PNC uptake.
Objective
The objective is to determine the level of utilization of PNC service and associated factors in the Savannah region of Ghana.
Methods
The study used a facility-based analytical cross-sectional study design. The study was carried out in 311 postnatal mothers using consecutive sampling. Data collection was carried out using a questionnaire. Univariate and multiple logistic regression was performed to establish the determinants of PNC. Variables/variable categories with P < .05 were significantly associated with PNC. The significance level is anchored at P < .05.
Results
The study showed that almost all respondents (98.7%) have heard about PNC services through health workers (39.7%), media (13.0%), and friends and relatives (47.2%). Most of the respondents (88.7%) have used PNC services within 48 h. Mothers aged 25–39 years were about seven times more likely to utilize PNC compared to those who were less than 25 years old (AOR [adjusted odds ratio] = 7.41, 95% CI [confidence interval]: 1.98–7.71); mothers with high school education (SHS) and above were also approximately four times more likely to use PNC compared to those who had no formal education (AOR = 3.65, 95% CI 1.97–13.66). In the same vein, married mothers were 10 times more likely to use PNC compared to those who are single mothers (AOR = 10.34, 95% CI: 3.69–28.97), whereas mothers who had at least four antenatal care (ANC) visits during pregnancy were approximately seven times more likely to use PNC compared to those who had less than four ANC visits (AOR = 6.92, 95% CI: 1.46–32.78). Reasons for not attending PNC include waiting time (40.5%), health workers’ attitude (32.4%), being attended by a student (16.2%), being busy (27.0%), inadequate information on PNC (24.3%), and no family support (18.9%).
Conclusion
All mothers knew about the PNC services, with a higher proportion patronizing the services. The increasing age, the level of mothers, marital status, and participation in ANC were significant determinants of the use of PNC. More education during ANC on the importance of PNC service is required to achieve universal coverage of PNC.
Keywords
Introduction
The essential component of the continuum of essential obstetric care (EOC) that can help reduce maternal, neonatal, and infant morbidity and mortality in developing countries is the PNC service, as it is with prenatal care, labor, and delivery care services (Say & Raine, 2007). According to the World Health Organization (WHO), postnatal care (PNC) is defined as the care provided to a woman and her newborn child within hours after placenta birth and during the first 42 days (6 weeks) of life (World Health Organisation, 2010).
The available literature shows that more than half of the 585,000 maternal deaths worldwide yearly occur on the first day after giving birth (Hordofa et al., 2015). Maternal death rates are still unacceptably high in the world. For example, in 2017, around 295,000 women died during pregnancy and/or after delivery. Therefore, every day, nearly 810 unnecessary deaths of women related to pregnancy and delivery were recorded around the world (WHO & UNICEF, 2019). Although there has been a significant reduction in the maternal mortality rate (MMR) globally, including in Sub-Saharan Africa (SSA) and southern Asia, about 86% (254,000) of global maternal deaths in 2017 occurred in SSA and Southern Asia alone. Of this, two-thirds (196,000) of maternal deaths occurred in SSA alone, while one-fifth (58,000) occurred in Southern Asia (WHO & UNICEF, 2019).
From those mentioned above, it is envisaged that appropriate PNC can prevent the majority of maternal and neonatal morbidity and death in the first days and hours after delivery (World Health Organization, 2015). Despite this important recommendation, the availability and utilization of PNC services in several African nations are reportedly hindered by several factors, including the 40-day window after birth, during which mothers and babies are only allowed to spend the first month indoors, misunderstandings about the importance of PNC, the cost of health services and transportation, accessibility, and distances (Appiah, Djan et al., 2021; Appiah, Kannor et al., 2021; Chaka et al., 2019; Gessesse, 2015; Munabi-Babigumira et al., 2021; Sagawa et al., 2021; Sisay et al., 2019). Furthermore, the relevant literature within the African context observed that the attitudes of healthcare professionals constitute a barrier to the use of PNC (Munabi-Babigumira et al., 2021; Munnaya et al., 2015).
Although PNC is crucial, PNC is typically the least prioritized in underdeveloped nations (Tiruneh et al., 2020), including Ghana. Maternal mortality ratios are still high in Ghana, with approximately 310 deaths per 100,000 live births in 2017 (Ghana Statistical Service (GSS), Ghana Health Service (GHS), 2018). This high MMR can be curbed if postnatal mothers follow the WHO PNC guidelines of at least three visits within the first 6 weeks (Okawa et al., 2015; Saaka et al., 2018). This will eventually lead to Ghana's effort to achieve Sustainable Development Goal 3 (SDG3). Although the benefits of PNC services are enormous and well documented, the use of PNC services in Ghana is not appreciable. According to the 2014 Ghana Demographic and Health Survey (GDHS), compared to other categories, 74% of women residing in rural regions were less likely to have an early postnatal checkup (Ghana Statistical Service (GSS) ICF International, 2015). This is partly due to the long distance to access PNC facilities (Dotse-Gborgbortsi et al., 2020) and the disproportionate distribution of health facilities and human resources between urban and rural areas in Ghana (Dickson et al., 2016).
Various studies in Ghana have reported the factors that influence the utilization of PNC services with varied outcomes, including the age and the nature of birth (be it C-section or vaginal delivery). The place of birth (whether hospital or home), the level of education, ethnicity, financial situation, the location of residence, and religion (Abor et al., 2011; Appiah, Djan et al., 2021; Appiah, Kannor et al., 2021; Sakeah et al., 2018). Furthermore, access to health facilities and awareness of PNC services could improve attendance (Ndugga et al., 2020).
Although the attendance of PNC services is not encouraging in Ghana, the utilization of PNC may be more difficult for women living in rural communities. Despite the correlation between the area of residence and the use of PNC, a comprehensive study on the use of PNC and associated factors has yet been conducted among Ghanaian women in dominant rural areas. For example, Adu et al. (2018) studied the impact of individual- and community-level determinants on maternal health outcomes in Ghana. They discovered that residency was a determinant because rural residents were less likely than urban residents to give birth in health facilities and have PNC. In rural Builsa and the West Mamprusi districts in Northern Ghana, Sakeah et al., (2018) investigated the impact of Community-based Health Planning and Services (CHPS) on PNC visits. They discovered that women who attended prenatal clinics (four times) and married to higher education levels were associated with at least three visits to the PNC.
The specific determinants of PNC utilization vary from one region of the country to another, and there is a shortage of information on PNC services, particularly in the newly created Savannah region of Ghana. The West Gonja Municipality is part of the Savannah region. Therefore, this study investigated the use of PNC services and associated factors in the West Gonja Municipality of the Savannah region of Ghana. Being a new region, these data are essential for policy planning and implementation. It could serve as a reference for the Savannah Regional Health Directorate and the GHS Family Health and Health Promotion Divisions as they prepare and plan maternal and child health promotion programs focusing on using maternal health services in rural Ghana.
Review of the Literature
Knowledge and Associated Factors That Influence PNC Services
Most women in Nepal did not patronize PNC, and therefore, the Nepal government should raise awareness of the uptake of PNC services (Khanal et al., 2014). In Nepal, approximately 43.2% of mothers were at the PNC services center within 42 days of birth, while approximately 40.9% showed that mothers are seen to have reported immediate PNC (Khanal et al., 2014).
In Africa, the utilization of PNC service is increasing, but there is still a need to improve. For example, a study conducted by Angore et al. (2018) in Ethiopia revealed that 83% patronized PNC services. Contrary to above, another study conducted in the same geographic location showed that about 30% of postnatal mothers attended PNC services (Akibu et al., 2018). Surprisingly, a study in Ethiopia still reports that PNC usage among mothers is as low as 6.9% (Sisay et al., 2019). In a systematic review and meta-analysis, the estimated use of PNC services is approximately 32% (Chaka et al., 2019).
So far, Uganda has recorded the lowest utilization rate of PNC services, with only about 15% of postnatal women attending PNC services (Izudi & Amongin, 2015). In Kenya, the utilization of PNC services is improving year by year at a slow pace. Asem (2016) revealed that nine in 10 women with children under 2 years of age were satisfied with the services provided by the PNC department of LEKMA Hospital in Accra.
Existing global research has shown that a variety of factors, including the age of the mother, the degree of education, the job, the location and the method of delivery, the total number of pregnancies, and the awareness of obstetric-related warning signs, along with knowledge of PNC services, frequently influence the use of PNC services. It is important to remember that the variables affecting the use of PNC services vary by culture and sociocultural elements within a specific community (Berhe et al., 2013; DiBari et al., 2014; Worku et al., 2013).
In Ethiopia, a study showed that unmarried mothers were unlikely to use PNC compared to their married counterparts who were married and stayed with their spouse. Furthermore, the level of knowledge was considered a crucial factor the utilization of PNC (Angore et al., 2018). Similarly, a study in northern Shoa, Ethiopia, revealed that the type of delivery, parity, and education were statistically significant factors related to higher uptake of PNC services (Akibu et al., 2018). Sisay et al. (2019) also report that mothers with very low or no educational status, with increasing age, in the poorest wealth quantile, and having a history of antenatal care (ANC) visits were statistically associated with patronization of PNC services.
A systematic and meta-analysis of the utilization of PNC showed that the use of ANC, the availability of healthcare workers, and residents of urban areas were associated with the use of PNC in Ethiopia (Chaka et al., 2019).
In Nigeria, a study conducted on the determinants of utilization of PNC services in Nigeria revealed that the determinants of PNC services can be categorized into household and community levels, which include the level of education, financial status, living in urban or rural areas, religion or faith, source of information and its accessibility, parity, mother's age, and previous experience with services (Iyanda, 2017).
In India, some mothers view PNC as unnecessary, but distance to PNC service centers, poor knowledge of PNC, and financial burden were cited as reasons for not attending PNC services (Kaur & Kaur, 2018).
In Malaysia, factors associated with full PNC service utilization including higher educational status, income level of financial independence, involvement of the male partner, being of low birth order and knowing about the danger signs in newborns, and the hearsay and myths about postnatal practice were observed to be a strong barrier to the higher patronage of PNC (Mon et al., 2018).
Analysis of the 2014 GDHS showed that women residing in Savannah areas patronize PNC services compared to those in the coastal zone; also, Guan tribes used PNC services more than the Akan (Appiah, Kannor et al., 2021). Analysis of the 2014 GDHS further revealed that working women and those closer to PNC centers were more likely to patronize PNC services (Appiah, Kannor et al., 2021). Browne et al. (2016) opined that ownership of the National Health Insurance Scheme card among mothers is pivotal in utilizing maternal, neonatal, and child health continuum of care service.
Methods
Study Setting
The West Gonja Municipality, located in the Savannah region of Ghana, is one of the seven administrative districts. It can be found at latitudes 80 321 and 100 21 north and longitudes 10 51 and 20 581 west. The municipality has a total land area of about 4,700 km2, with Mole National Park and forest reserves accounting for 30% of the territory. The city is bounded to the south by the Central Gonja District, to the west by the Bole and Sawla Tuna Kalba Districts, to the northwest by the Wa East District, and to the east by the North Gonja District. According to the 2021 population and housing census, the municipality has 63,449 residents, including 32,270 men and 31,179 women, with expected pregnancies of 3,173. A total of 27 health facilities (22 CHPS, three health centers, one maternity home, and one district hospital) are distributed in the municipality.
Study Design
This study used a facility-based analytical cross-sectional design with a quantitative research approach.
Study Population
This includes all postnatal mothers within the West Gonja District of the Savannah region of Ghana.
Inclusion and Exclusion Criteria
The study included mothers whose children were older than 6 weeks but less than 12 months and who resided in the West Gonja Municipality of the Savannah region of Ghana. However, women with physical or mental illnesses who could not communicate effectively were excluded.
Sample Size Determination
The sample size (n) was calculated using the Snedecor & Cochran (1989) formula for a point estimate sample;
Sampling
In the sampling strategies, 10 health facilities were chosen, two from each of the five health submunicipalities (Damongo, Busunu, Dass, Larabanga, and Canteen submunicipalities). All are mostly rural except the Damongo submunicipal which is primarily urban. The health facilities were selected through simple random sampling with the lottery. Each of the health facilities serves a cluster of communities. To ensure greater participation, the weighing days of each health facility were collated. Mothers who met the inclusion criteria for each health facility were recruited by simple random sampling. Mothers who attended or presented child welfare care services were asked to pick a piece of paper. These pieces of paper had “yes” or “no” written on each. Those who chose “yes” were recruited into the study. The process was repeated until the sample size was reached.
Data Collection Tools and Procedures
A semistructured questionnaire was developed and used in the data collection process. The questionnaire was developed after reviewing the relevant literature, which included previous questionnaires that had been applied to other research projects on the subject field (Appiah, Djan et al., 2021; Appiah, Kannor et al., 2021; Hordofa et al., 2015; Sakeah et al., 2018).
The questions were prepared in English (S1 Questionnaire) and translated into Gonja and other local languages. Before actual data collection, four midwives were recruited as field enumerators. The principal investigator trained these field enumerators on the study’s purpose, the questionnaire's administration, the sampling procedures, and the use of smartphones to collect data. To ensure consistency, 10% of the sample size (32 mothers) within the inclusion criteria was recruited from two health facilities for pretesting. These two health facilities were excluded from this study. Based on the pretest outcomes, modifications to the questionnaire's order and language were made. Mothers who agreed to participate in this study could choose a suitable time and venue for the interview. This was done to ensure that these mothers were comfortable answering the questionnaire. In addition, a private area was identified in each of the facilities to conduct interviews so that the conversation would not be heard by a third party and would not be distracted by others. Each interview lasted between 15 and 20 min. The principal investigator examined the data obtained daily to ensure that they were accurate and consistent. Data collection began in February 2022 and ended in April 2022.
Study Variables
The dependent variable is using PNC services within 2 days of delivery. According to relevant literature (Abuka Abebo & Jember Tesfaye, 2018; Angore et al., 2018; Khanal et al., 2014; Mon et al., 2018) and WHO recommendations (World Health Organisation, 2010), for a mother to have said that she had used PNC services, the mother must have attended at least one postnatal visit within 24–48 h after birth.
However, independent variables include sociodemographic characteristics such as age, religion, educational status, family size, average monthly income, and marital status; maternal characteristics such as age at first pregnancy, parity, gravida, place of delivery, mode of delivery and ANC attendance; and knowledge and awareness of PNC services. These were arranged in sections of the questionnaire: Section A had items on sociodemographic characteristics, Section B had things on maternal traits, Section C included items on knowledge of PNC services, Section D included utilization of PNC items, and Section E had challenges of PNC questions.
Data Cleaning and Analysis
To verify accuracy and missing values, data were cleaned. Recoding and categorization were done. Stata/SE version 14.0 was used for the analysis. Background characteristics of the participants and knowledge and use of PNC were explored using descriptive statistics. Binary logistic regression was used to determine the single effects of each explanatory variable on the outcome measure (PNC service utilization).
Multiple logistic regression analysis was performed to account for confounders and discover factors related to the use of PNC services. Only variables with a P-value less than .25 in the chi-squared test (Tables 1 and 2) were included in the multivariate analysis. Statistical significance was assessed at a P-value less than .05. The tables and graphs presented the results as frequencies, percentages, and ratios.
Sociodemographic Characteristics of the Respondents, West Gonja Municipal, 2022 (n = 311).

Maternal Characteristics of the Respondents, West Gonja Municipal, 2022 (n = 311).

Ethical Considerations
The principles of the Declarations of Helsinki were strictly followed when conducting the study. First, the approval of the study's ethical practices was received from the Committee on Human Research, Publications & Ethics (CHRPE) of the Kwame Nkrumah University of Science and Technology (KNUST), Kumasi, Ghanawith reference number (CHRPE/AP/039/22). Additionally, permission was granted by the Savannah Regional Health Directorate to conduct the study. Each respondent expressed their consent before participating in the study. Participants gave their informed and oral permission after obtaining all study information. All participants were informed that participating in the study was completely voluntary and that they could decide not to do so at any point during the process if they wanted. They were also informed that the study results would be made public.
Results
Sociodemographic Characteristics of the Respondents
A total of 311 postnatal mothers were included in this study. Most of the respondents (63.7%) were between 25 and 39 years old, and a minor age group (13.5%) was those <40 years. A higher proportion of the respondents (45.0%) had no formal education. The majority of the respondents (74.9%) were Muslims, and 80.7% were married. Also, 78.5% of the respondents had 3–5 children. More than half (57.9%) of the respondents reside in rural areas (Table 1).
Maternal Characteristics
More than half of the respondents (54.0%) had their first pregnancy before 25, with the mean age at the first pregnancy reported at 24.44 ± 4.81. Most mothers (93.6%) had at least four ANC visits (ANC), and nearly 80.0% had vaginal delivery in their last pregnancy. Only 6.1% of the respondents had experienced neonatal death, and 94.5% of the respondents were delivered to the hospital (Table 2).
Knowledge of PNC Services
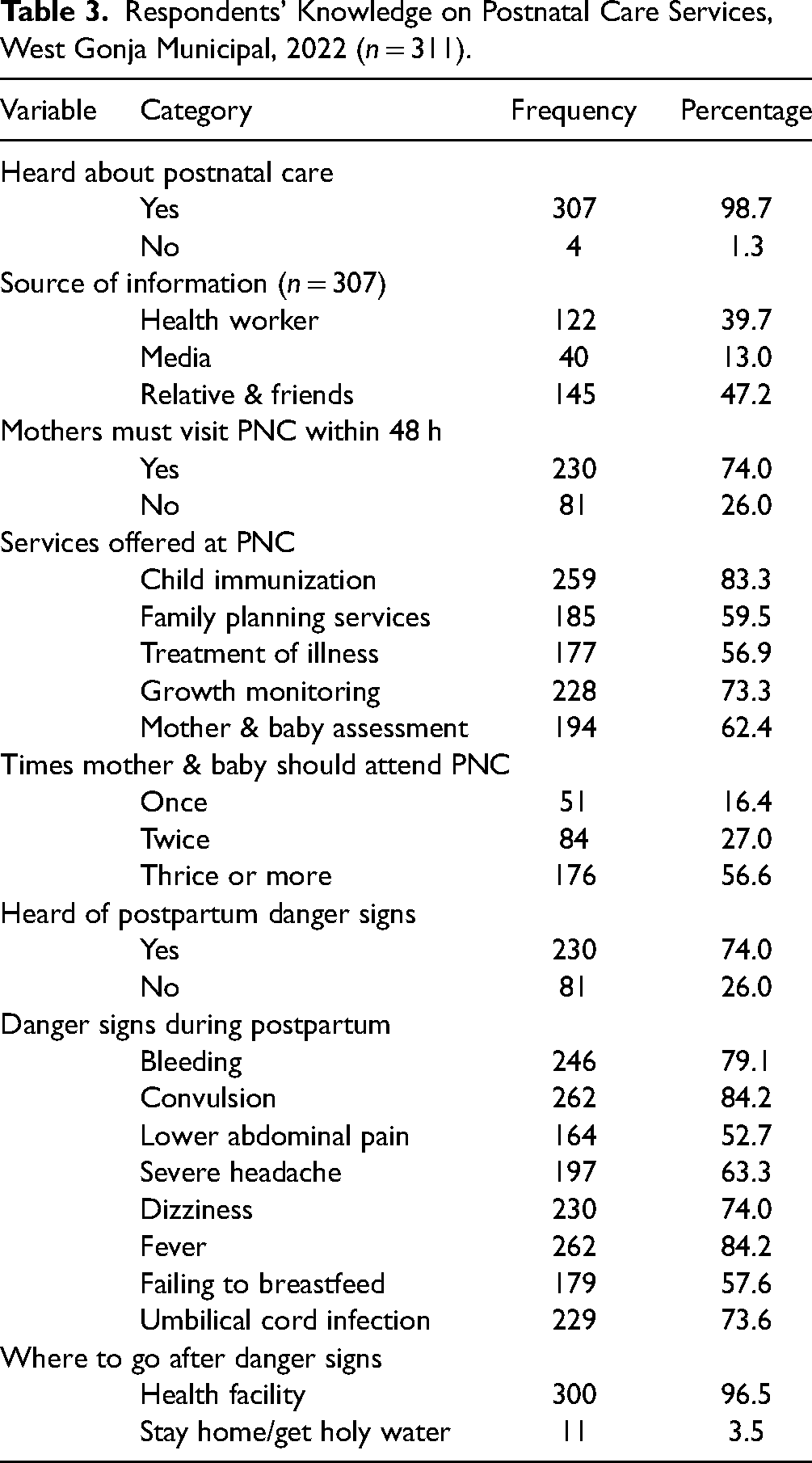
Almost all the respondents (98.7%) have heard about PNC services through healthcare workers (39.7%), the media (13.0%), and friends and relatives (47.2%). Most mothers (74.0%) knew that they had to visit the PNC within 48 h after delivery. The respondents knew that the following services were offered in the PNC centers: child welfare (83.3%), family planning (59.5%), treatment (56.2%), growth monitoring (73.3%), and mother and baby evaluation (62.4%). Most mothers (56.6%) indicated that the mother and baby should attend PNC three times or more, 74.0% have heard postpartum danger signs, and 97.0% of mothers will go to the hospital if they see danger signs (Table 3).
Respondents’ Knowledge on Postnatal Care Services, West Gonja Municipal, 2022 (n = 311).
The Utilization of PNC Services
Most of the respondents (88.7%) used PNC services within 2 days (48 h) after delivery, while 11.9% visited PNC facilities for care after 2 days (>48 h). Reasons for not attending PNC include long waiting time (40.5%), poor attitude of health workers (32.4%), being attended by a student (16.2%), being busy (27.0%), no information on PNC (24.3%), and no family support (18.9%) (Figure 1).

Reasons for not using PNC services within 48 h (West Gonja Municipal, Ghana. 2022).
Factors Influencing the Utilization of PNC Services
In the univariate analysis (Table 4), the study showed that respondents 25–39 years (crude odds ratio [COR] = 16.40, 95% confidence interval [CI] 7.0–38.41) and those who were 40 years and above (COR = 28.31, 95% CI: 3.68–43.58) had the highest probability of using PNC compared to those less than 25 years. Being married (COR = 21.09, 95% CI 19.37–37.44), having children between 3 and 5 (COR = 4.66, 95% CI: 1.94–11.16), children above 5 (COR = 10.82, 95% CI: 2.04–15.90), mothers who had four or more ANC visits during pregnancy (COR = 7.39, 95% CI:2.83–19.32), and having first pregnancy after 24 years (COR = 4.40, 95% CI: 1.87–10.32) had a higher probability of using PNC.
Factors Influencing Postnatal Care Service Utilization, West Gonja Municipal, 2022.
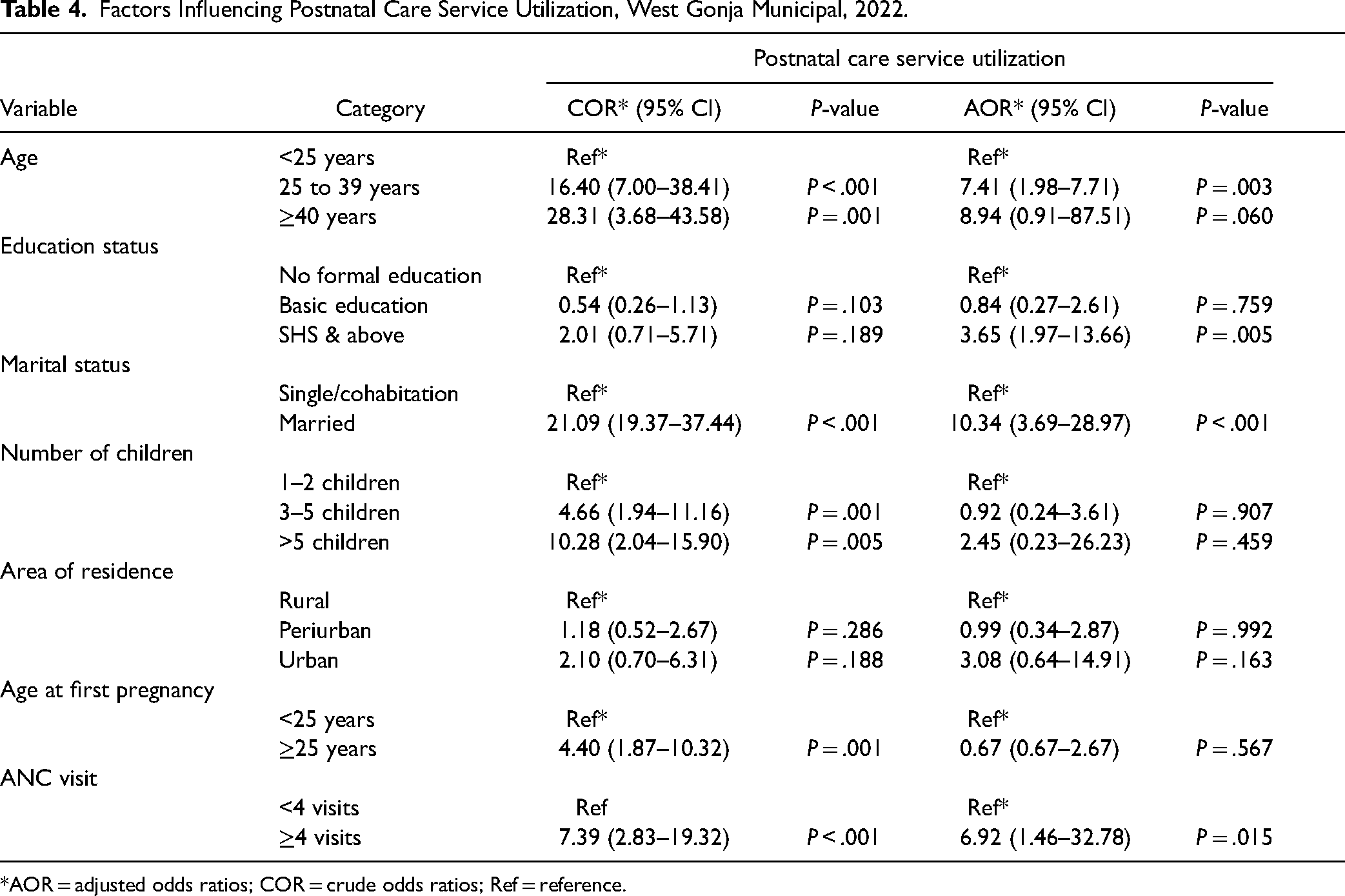
*AOR = adjusted odds ratios; COR = crude odds ratios; Ref = reference.
In the multiple logistic regression model (Table 4), the study showed that respondents who were 25–39 years of age had a higher probability of using PNC services compared to their counterparts who were less than 25 years of age (adjusted odds ratio [AOR] = 7.41, 95% CI: 1.98–7.71). Mothers with high school (SHS) education and above were 3.65 times more likely to patronize PNC services within 48 h than mothers without formal education (AOR = 3.65, 95% CI: 1.97–13.66). Additionally, married mothers are 10.34 times more likely to use PNC services within 48 h than single or cohabitation mothers (AOR = 10.34, 95% CI: 3.69–28.97). Finally, the study showed that mothers who attended ANC at least four times during pregnancy were 6.92 times more likely to go for PNC services within 48 h compared to those mothers who had less than four ANC visits during pregnancy (AOR = 6.92, 95% CI: 1.46–32.78).
Discussions
Studies have shown that maternal healthcare services (MHSs), such as PNC, can reduce maternal deaths. Most motherhood deaths occur during the postpartum period. Despite the importance of PNC, there is currently a low usage level of PNC services, even though there are regional variations, particularly in low- and middle-income nations. This study aimed to determine the knowledge, utilization, and determinants of PNC utilization in the West Gonja Municipal. The study showed that all mothers were aware of PNC services, with a higher proportion utilizing these services within 48 h (2 days) after delivery. Also, age, formal education, marital status, and ANC attendance during pregnancy were identified as significant sociodemographic and maternal characteristics influencing the use of PNC services. Despite these determinants, factors such as long waiting times and bad attitudes of health personnel also serve as barriers to utilizing PNC services.
Almost all respondents were aware of PNC services. This agrees with a study in Malawi in which most women have reported having heard about the PNC services (Olajubu et al., 2019; Sagawa et al., 2021). These similarities could be attributed to efforts by all African countries to reduce maternal and child mortality. The GHS has implemented strategies to reduce infant and maternal morbidity and mortality using MHS utilization. Friends, relatives, health workers, and the media were the informants on PNC services. This differs from other study fields (Ghiasi, 2021; Vogels-Broeke et al., 2022) where health workers were considered the main informants about pregnancy and childbirth-related information. The current study was conducted in an area predominately rural where community volunteers are being used to do health advocacy, especially on maternal and child health. Since these volunteers are known faces in the community, the mothers tend to appreciate health concepts better from these volunteers. Therefore, this could account for the differences. Consequently, to reach a more comprehensive coverage of MHS, a varied source of information is encouraged to increase awareness and use.
Furthermore, the study revealed that 88.1% attended PNC services within 48 h after delivery. This is an improvement over the utilization of 74.1% of PNC of rural women in Ghana (Appiah, Kannor et al., 2021) and slightly higher than the 84.8% reported in Malawi Field (Sagawa et al., 2021) and about 84.0% in Ethiopia (Angore et al., 2018). On the contrary, relatively low utilization of PNC services was reported in western Ethiopia (23.6%) (Beyene et al., 2022), 25.2% in Myanmar (Mon et al., 2018), 22.0% in Nigeria (Olajubu et al., 2019), and about 25.0% in Mali (Ahinkorah et al., 2021). The wide variety of these findings may be attributed to the various research contexts, study periods, and other relevant factors, including access to health facilities, deliberate government interventions, differences in geographical location, and the culture of people. Furthermore, in the current study, PNC services were used 48 h following the WHO recommendation (World Health Organisation, 2010), while the other studies restricted PNC to 24 h. This could also explain differences in the utilization rates.
The study on the determinants of using PNC services showed that mothers aged 25–39 had higher chances of PNC utilization compared to those under 25 years of age. This is corroborated by a study in Ghana (Appiah, Djan et al., 2021). The possible reasons for these similarities could be that older mothers may have been introduced to the information about PNC at delivery, improving their understanding of the need for PNC. This is further strengthened by the idea that familiarity with certain healthcare services is crucial in how often those services are used (Hochbaum et al., 1952).
The study revealed that women with higher educational levels (SHS and above) were more likely to use PNC services than those without formal education. This finding is consistent with the vast literature in Africa (Akunga et al., 2014; Beyene et al., 2022; Kanté et al., 2015; Sagawa et al., 2021; Sakeah et al., 2018; Sisay et al., 2019). These similarities can be ascribed to the fact that education acts as a stand-in for knowledge, cognitive abilities, and values, encouraging health-seeking behavior by raising awareness of available health services (Beyene et al., 2022). Another likely explanation is that education gives women more control over their lives and makes it easier for them to interact with their families and seek MHS.
In addition, being married is associated with increased odds of using PNC compared to single mothers. This finding is consistent with other findings (Angore et al., 2018; Appiah, Djan et al., 2021). Several factors might explain this finding. Firstly, married women who live with their spouses may receive help from them compared to unmarried women. Another point is that, unlike married couples, gender responsibility is not well structured. Skinner et al. (2002) argue that cohabiting faces more misunderstandings than married people. As a result, it can be inferred that single mothers making decisions about PNC services may result in miscommunication and decreased partner support. Cohabiting women may be less likely to disclose their use of various MHSs, such as PNC, as a precaution against stigma and scorn because giving birth outside of marriage is less desirable in most Ghanaian communities (Appiah, Djan et al., 2021).
In the determinants of PNC, ANC visits (at least four visits) during pregnancy was found to increase the use of PNC significantly. This finding is supported by other studies elsewhere (Beyene et al., 2022; Chaka et al., 2019; Sisay et al., 2019; Tesfahun et al., 2014). The possible explanation for these results is that pregnant women who attended ANC services may have had a higher probability of being exposed to various types of services, counseling, and support about their health and that of the baby. Women may learn crucial information about health problems that arise before, during, and after childbirth during their ANC visits. This raises women's awareness of possible complications and motivates them to use the PNC service.
Consequently, the nonuse of PNC increases unfavorable consequences such as postpartum bleeding, adverse birth outcomes, and poor breastfeeding habits. These fallouts could further worsen the subregion's maternal and child mortality rates. The use of PNC services is significant, and healthcare professionals must take note, since it underscores the urgent need to ensure that women receive official appointments to evaluate the baby and the mother before they are sent home after birth. However, a limiting element is that some women give birth outside of official healthcare facilities. In terms of this, most women reported that obstacles such as long waiting times, negative attitudes of health personnel, being attended by a student, being busy, lack of information on PNC, and lack of family support could hinder their attendance at PNC. Other research has corroborated some of these concerns. In Indonesia, for example, a study indicated that a lack of understanding of the significance of PNC services could hinder its utilization field (Probandari et al., 2017). Furthermore, studies in Ghana (Dapaah & Nachinaab, 2019) and Nigeria (Idris et al., 2013) show that the negative attitude of health workers has been linked to poor utilization of MHS among mothers. Long distance has also been cited as a barrier to MHS utilization (Dapaah & Nachinaab, 2019).
Strengths and Limitations of This Study
Since women were asked to recall incidents from 6–12 months before the survey and women's quest to create a good impression about their PNC attendance, this study may be exposed to recall and social desirability bias, respectively. Furthermore, because the study has a quantitative approach, it ignores the sociocultural concerns. Despite these limitations, this study is unique, as it is among the few studies to unravel the predictors of the utilization of PNC services in the Savannah region. The robustness of the findings was guaranteed by the careful analytical processes used to estimate the predictors of PNC utilization.
Implications for Practice
Educating women and providing equitable access to healthcare services is imperative to improve maternal and child health outcomes. Local government officials should request more healthcare funding to appoint more health professionals to reduce long waiting time, and more promotion campaigns should be organized to educate women and their family members about available services to avoid negative consequences for mother and child's health. More empirical research is needed to evaluate the effectiveness of current services and the gaps in the services to implement new strategies.
Conclusion
Almost all mothers were aware of the PNC services, and a higher proportion patronizes the services. Increasing age, mother's educational level, marital status, and ANC attendance have been identified as significant determinants of PNC utilization. Although the benefits of PNC services are enormous, some challenges, including lack of support from home, being busy, the negative attitude of health workers, and long waiting times in PNC centers, could thwart the efforts to achieve SDG3. Therefore, to increase the utilization of PNCs and MHSs at large, there is a need to reduce waiting time, promote a good attitude among health workers, increase the workforce, and expand health infrastructure. It is recommended that policies that enforce women's training in higher degrees should be strengthened, as these could expose women to information on the benefits of PNC utilization. During ANC visits, more attention and education should be given to mothers about the need to continue with PNC after the birth of the child. Long waiting times and attitudes of the health worker must be checked through staff recruitment and motivation and supportive supervision of the health workers. Finally, policies on family support during PNC must be enforced.
Footnotes
Acknowledgments
We thank very much all the study participants who took advantage to be part of the study at will.
Authors’ Contributions
Conceptualization was performed by MNA, AA1, FAW, and RK. Data collection was performed by MNA and FAW. Data curation was performed by MNA, AA1, and AA2. Formal analysis was performed by MNA, AA1, CK, and BKP. Project supervision was performed by AA1, AA2, FA, and CK. Contribution to the writing of the manuscript (original draft) was performed by MNA, RK, BF, and RNN. Review and editing were performed by AA1, FA, AA2, CK, RK, and BKP. All authors proofread and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The principles of the Declarations of Helsinki were strictly followed when conducting the study. First, approval of the study's ethical practices was received from the Committee on Human Research, Publications & Ethics (CHRPE) of the Kwame Nkrumah University of Science and Technology (KNUST), Kumasi, Ghana, with reference number (CHRPE/AP/039/22). Also, permission was granted by the West Gonja Municipal Health Directorate to conduct the study. Each respondent expressed their consent before participating in the study. Participants gave oral and written informed permission after obtaining all study information. All participants were informed that participating in the study was completely voluntary and that they could decide not to do so at any point during the process if they wished. They were also informed that the study results would be made public.
Data Availability
The data used to support this study are available from the corresponding author upon request.