
Abstract
Introduction
In a pandemic, the risk of infection and mortality for nurses can increase substantially. This study analyzes the information reported on the mortality of nursing personnel from different countries due to COVID-19.
Methods
We performed a scoping review by searching information available in PubMed, Scielo, and Google Scholar databases using concepts related to nursing, mortality, COVID-19, etc. The studies were searched from September 1 to October 30, 2021. This review included 12 articles were selected among 73 identified for the scope search because they included nurses.
Results
Nursing personnel presented a high mortality rate after physicians and health personnel. The average age of the deceased nurses was 43 years, being higher in men than in women. Higher mortality rates were reported in services attending COVID-19, nursing homes, and psychiatric centers.
Conclusion
Contagion and deaths are attributed to lack of planning and inadequate personal protective equipment.
Introduction
Healthcare workers have faced coronavirus disease 2019 (COVID-19) caused by the new severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Nursing personnel are a key agent in interdisciplinary healthcare teams, providing direct care to individuals, families, and communities in hospitals, community centers, at home, in ambulatory care centers, in vaccination centers, and nursing homes, among others. Several of these centers concentrate subjects potentially infected with COVID-19. This group of professionals constitutes a segment of approximately 28 million workers in the world, which represents more than half of the health professionals, who carry out their work under physical and psychological pressure (Bandyopadhyay et al., 2020).
Ensuring the safety of nursing staff is essential to plan the strategic response of any country to the current health crisis; otherwise, a country’s response to the COVID-19 pandemic may be seriously disrupted, with great consequences for the population. Social and economic disparities, particularly in hospital and community healthcare settings, have been widespread, including developed countries, like shortage of trained personnel, migration of skilled labor, and uneven geographic distribution of healthcare personnel, even before the pandemic (Bandyopadhyay et al., 2020; Mao & Chen, 2020).
Another important aspect in nursing staff care for COVID-19 is adequate access to Personal Protective Equipment (PPE) (Forrester et al., 2020). The World Health Organization and other regulatory agencies have published recommendations and guidelines on the rational use of hospital and community PPE to reduce the risk of COVID-19 transmission in healthcare areas (European Centre for Disease Prevention and Control, 2021; Occupational Safety and Health Administration, 2020; World Health Organization, 2021).
Since the beginning of the outbreak, studies have reported different proportions of nurses affected, ranging from 3.8% in China and the United States to 10% in Italy (Antonio-Villa et al., 2020). The International Council of Nurses (ICN) reported that as of September 2020, 1,500 nurses had died from COVID-19. Figure 1 includes nurses from just 44 countries, which is known to be an underestimation of the true number of deaths. In Mexico, there have been 283,122 cases of COVID-19 and 4,517 deaths in health personnel (doctors, nurses, laboratory specialists, dentists, and other health workers) as of October 25, 2021.

Flow diagram of the bibliographic selection process and results.
According to Secretaría de Salud (2021), 39% of COVID-19 deaths correspond to healthcare workers. Of this percentage, physicians rank first (45%), followed by other healthcare workers (31%) and nurses (19%). This means that 0.8% of all deaths in Mexico correspond to nursing personnel, which represents a notable occupational hazard. Therefore, it is important that the government or health entities have a record of the number of cases and deaths due to COVID-19 among nursing personnel to build protocols and protection strategies for future epidemiological contingencies. The purpose of this study is to analyze the information reported on nursing staff mortality during the COVID-19 pandemic and to compare mortality rates around different regions of the world.
Methods
To search for information on the mortality of nursing staff due to COVID-19, a scoping review was carried out following the methodology proposed by Peters et al. (2015), to provide a general description of the existing evidence on a certain topic regardless of the quality of the studies. This method consists in determining the objective of the review, the inclusion criteria, the focus to be investigated, searching the databases, including gray literature, and selecting and extracting the relevant information for the review and presentation of the results that can be arranged in a logical, schematic, or tabular form, and/or in a descriptive format that aligns with the objective/s and the scope of the review. Scoping reviews are a “preliminary assessment of potential size and scope of available research literature” (Grant & Booth, 2009); therefore, this review does not include a formal assessment of the methodological quality of the included studies.
An Internet search of the information published during the period from March 2020 (declaration of the COVID-19 pandemic by the WHO) to October 2021 was carried out, in English, Spanish, Portuguese, and Italian. Only studies providing data on the subject were included. The databases used were PubMed, Scielo, and Google Scholar. Indexed terms in Medical Subject Heading (MeSH) and Descriptors in Health Sciences (DeCS) were used as Health Professional, Health Personnel, Health Worker, Death, Dying, Mortality, Nurse, Nursing, and COVID-19 terms and SARS-CoV-2. Inclusion criteria terms consist of health personnel, nursing, mortality, COVID-19, nursing home, death, and COVID. Documents that did not refer to nurses or those in which the data for this group were not clearly broken down were excluded.
The search was carried out from September 1 to October 30, 2021. We use “AND” between healthcare personnel and nursing because healthcare personnel include physicians, radiologists, laboratory chemists, clinical nutritionists, and other healthcare professionals. Table 1 shows the strategies and terms used for each database and the results obtained.
Document Search Strategies.

Note. This table shows the search strategies with the highest frequency.
The new PRISMA flow diagram (Figure 1) (Page et al., 2021) was used as a guide to select the reports. Once the articles were identified in the databases and duplicates eliminated, the selection process was carried out by three reviewers who analyzed titles and abstracts. Subsequently, two reviewers extracted the data from the articles including author, year, country, objective, sample size, design, and main results (age and sex, comorbidities, and work area) from the full manuscript, using a format approved by the project team.
Results
The literature review includes one systematic review, two case reports, six retrospective epidemiological reviews, one opinion article, and two letters to the editor. Evidence found with detailed information is limited to data reported by Brazil, China, Germany, Italy, Malaysia, Mexico, the United Kingdom, and the United States. However, it should be noted that the data extracted are not homogeneous, possibly because there are few reports on nurse mortality. This made it impossible to organize the information in a specific data table (Table 2).
Characteristics of Nursing Staff Mortality due to COVID-19.

Of the 73 articles identified in the scoping search, only 12 studies met the inclusion criteria for analysis, as seen in the flow chart. The selected studies were published between 2020 and 2021 and corresponded to reports from China (2), Brazil (2), Mexico (2), Italy (1), the United States (1), Germany and Malaysia (1), and the United Kingdom (1) and international reports (2). Some articles inform on nursing mortality figures in various countries. Erdem and Lucey (2021) reported morbidity and mortality in 37 countries; Mao and Chen (2020) analyzed mortality in China and the United States; and Barretto and Phillips (2020) reported data for Brazil, the United States, and the United Kingdom.
The scope review shows that there is a predominance of women in regional reports (Table 3), but the percentages are inverted in international studies (Erdem & Lucey, 2021; Keles et al., 2021). Data by country or region show a higher number of nurse deaths in the United Kingdom: 35 according to Erdem and Lucey (2021); 48 according to Kursumovic et al. (2020); 102 according to Keles et al. (2021); and 77 according to Barretto and Phillips (2020). The United States reported: 75 according to Mao and Chen (2020); 363 according to Keles et al. (2021); 146 according to Barretto and Phillips (2020); and 259 according to Bandyopadhyay et al. (2020). Brazil: 292 according to Scherlowski et al. (2021); 127 according to Keles et al. (2021); and 157 according to Barretto and Phillips (2020). Finally, Mexico presented 42 deaths in nurses according to Guerrero-Torres et al. (2021); 274 according to Erdem and Lucey (2021); 132 according to Robles-Pérez et al. (2021); and 192 according to Keles et al. (2021). High mortality rates for nurses are reported in developed countries such as England and the United States, as well as in developing countries such as Brazil and Mexico, implying that the number of deaths similarly affected these countries, despite their socioeconomic and health system disparities.
Result of Nursing Staff Mortality due to COVID-19.
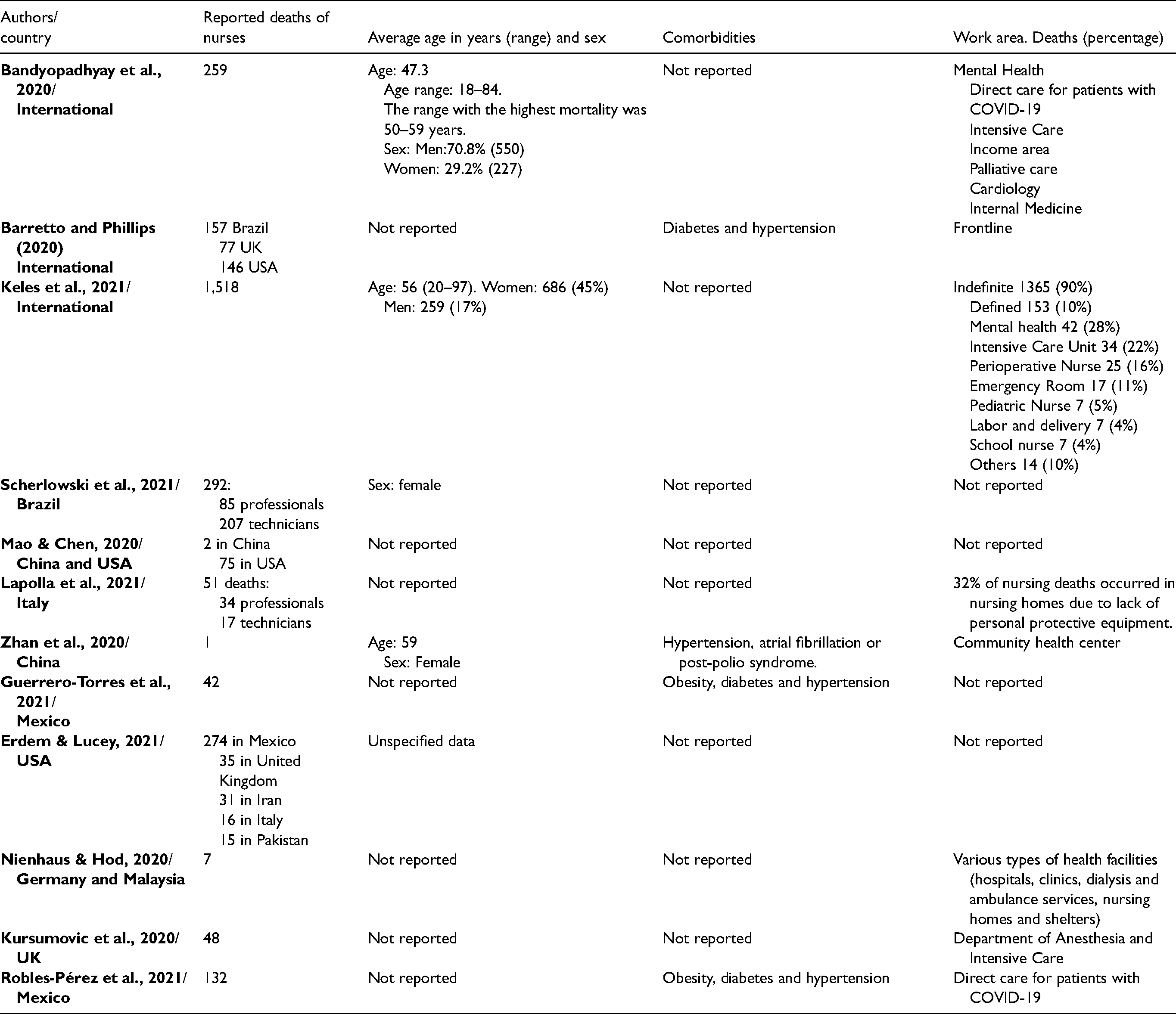
To date, few demographic and clinical descriptions of deceased nursing personnel have been found (age and sex, comorbidities, professional or technical training, work area, etc.). As reported by Robles-Pérez et al. (2021), Scherlowski et al. (2021), Barretto and Phillips (2020), Zhan et al. (2020), comorbidities such as obesity, diabetes, and hypertension increase the risk of death. Other less frequent comorbidities in healthcare personnel such as atrial fibrillation, post-polio syndrome, hemolytic anemia, and HIV also increase the risk of death (Robles-Pérez et al., 2021; Zhan et al., 2020).
From the literature data, it was identified that the mean age at death of nursing staff was 42.62 years. Age over 60 years was considered as a factor associated with the risk of death (Lapolla et al., 2021). Even though nursing is practiced mostly by women in the world, it was identified that there is a higher death rate in men (Bandyopadhyay et al., 2020; Guerrero-Torres et al., 2021). In addition, there is a difference in deaths according to the level of nursing specialization. For example, in Brazil 85 graduate nurses and 207 technical nurses died (Scherlowski et al., 2021), while in Italy 34 graduate nurses and 17 nursing technicians were reported (Lapolla et al., 2021). Regarding the work area, some articles report an increase in the proportion of deaths in direct care services for COVID-19 (Nienhaus & Hod, 2020; Robles-Pérez et al., 2021), in nursing homes (Lapolla et al., 2021; Nienhaus & Hod, 2020), and in the areas of psychiatry (Bandyopadhyay et al., 2020; Keles et al., 2021). In all cases, the causes of contagion and death are attributed to the lack of information and inadequate protective equipment.
Discussion
It can be assumed that nurses were heavily affected in the early stages of the pandemic due to high occupational exposure and that deaths among these workers were substantial. However, the review of the nursing mortality reports compiled for this study shows limited, fragmented, incomplete, and difficult to analyze information. These difficulties are set out below.
The sources of the data extracted for this scoping review are very broad, ranging from isolated case reports to systematic studies (Bandyopadhyay et al., 2020; Zhan et al., 2020); and from official epidemiological databases (Nienhaus & Hod, 2020) to information from the mass media (Keles et al., 2021; Kursumovic et al., 2020). In most cases, the databases that support the information are inaccessible and it is not easy to corroborate or complete the data; in other reports, sources are recognized as “gray literature,” based on information that is difficult to trace.
Another issue is that the information was difficult to classify and harmonize, as well as the variables to be analyzed for an observational study, such as sex, age, comorbidities, intra- or extramural exposures, types of work, unit or area, access to personal protective equipment, etc. Although some studies show raw data (Erdem & Lucey, 2021; Nienhaus & Hod, 2020; Robles-Pérez et al., 2021), in others the articles data is presented as percentages or proportions (Lapolla et al., 2021; Mao & Chen, 2020; Zhan et al., 2020). Finally, other reports only categorize general variables such as profession, number of infections, deaths, among others, data that is difficult to use and consolidate (Bandyopadhyay et al., 2020; Keles et al., 2021; Kursumovic et al., 2020).
It is likely that some health systems have systematically collected information on deaths of nurses from COVID-19 in the first year of the pandemic. However, it is difficult to deduce the reasons why the administrators of this information restrict the access. It is also important to mention that there is a gap in reports on deaths on healthcare workers in 2021. The records of health systems on morbidity and mortality from COVID-19 in nursing staff would be useful to empower the nurses themselves, as well as other health workers and researchers, about what happened in all healthcare centers to better prepare for future pandemics and plan the resources and best practices of care and containment of highly contagious and lethal diseases (Pan American Health Organization, 2021).
The evidence shows that the majority of deaths according to sex are women, which is proportional to the number of women in the nursing profession in the world (Erdem & Lucey, 2021; Keles et al., 2021). Likewise, a study reports that the average age of deaths is 56 years (Keles et al., 2021), this coincides with the average age of people with comorbidities such as hypertension and other cardiovascular diseases (Guerrero-Torres et al., 2021; Guo et al., 2020). COVID-19 in conjunction with comorbidities such as hypertension, diabetes, and obesity were identified to be associated with coronary plaque destabilization or aggravated hypoxia leading to death (Zhan et al., 2020). Regarding the literature comparison between regions on the mortality of nursing personnel, the information provided by current studies by region is scarce, making an analysis from this perspective complicated (Bandyopadhyay et al., 2020; Keles et al., 2021).
Furthermore, due to the nature of the publications, there may be discrepancies in the information extracted from the studies included for this review. In the Americas, we only found data registered in retrospective and prospective studies of longitudinal cohorts in healthcare centers of the United States, Mexico, and Brazil, reporting 815 deaths (Erdem & Lucey, 2021; Guerrero-Torres et al., 2021; Scherlowski et al., 2021). The foregoing contrasts with data from the European continent, where we find data reported for Germany, Italy, and the United Kingdom that add up to 106 deaths, corresponding to studies performed from data published in the mass media (Kursumovic et al., 2020; Lapolla et al., 2021). In China we only detected three deaths, but the nature of the publications, a letter to the editor, and an opinion article, may explain this figure (Mao & Chen, 2020; Zhan et al., 2020).
One of the relevant points highlighted in the consulted bibliography were the shortage of PPE (Guerrero-Torres et al., 2021; Keles et al., 2021; Lapolla et al., 2021; Nienhaus & Hod, 2020; Scherlowski et al., 2021) and negligence in work practices related to a large part of COVID-19 deaths in nursing personnel (Lapolla et al., 2021). Despite the efforts of health institutions to provide PPE during the pandemic, (Robles-Pérez et al., 2021), the high demand for such equipment caused a shortage of these equipment and forced the use of disposable masks and homemade protective clothing by the nursing staff (Mao & Chen, 2020). Not only is it important to have the necessary and adequate PPE for more effective protection (Nienhaus & Hod, 2020), but also training on the protocols for the correct use and disposal of this equipment (Pan American Health Organization, 2021).
Implications for Practice
This review found that nurses are the third most at risk group for infection among healthcare workers (Guerrero-Torres et al., 2021). This may be due to their direct contact with patients. Therefore, effective health strategies need to be developed for nurses.
Conclusions
This review presents relevant data to understand the general situation in which nursing personnel face the COVID-19 pandemic, despite the lack of concise information on countries and regions. It is observed that there are access restrictions to the databases of the health authorities. It can be concluded that there is no accurate and up-to-date data on the mortality of nursing personnel due to COVID-19 at the national or regional level. We have detected that data on nursing staff deaths are not adequately recorded, which makes it difficult to collect and correctly classify. Restrictions on access to databases of national or regional imposed by health authorities make it difficult to carry out observational studies of interest to the nurse workers and compromise the transparency of the analyzes.
While it is difficult to maintain records during the pandemic due to understaffing or inconsistent information, national and international strategies are required to facilitate access to this information for a more planned and effective response to the crisis by health workers, including nurses. In the case of Mexican health authorities, the information offered to the community on their portals should show more concise and stratified raw data on the morbidity and mortality of the different groups of health workers and official measures to reduce occupational risks.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.