
Abstract
Introduction
Occupational stress among nurses poses a significant challenge to healthcare systems, particularly in under-resourced and high-demand settings such as Palestine. Despite their critical role, limited research has addressed the prevalence and contributing factors of occupational stress among Palestinian nurses.
Objective
This study aimed to assess the level of occupational stress among nurses working in Hebron hospitals and identify key stressors and associated demographic and occupational risk factors.
Methods
A cross-sectional descriptive study was conducted between December 2023 and March 2024 involving 140 nurses from four hospitals in Hebron, West Bank, Palestine. Data were collected using the 34-item Health and Safety Executive (HSE) Occupational Stress Scale. Descriptive statistics, t-tests, ANOVA, and regression analysis were applied using SPSS version 23.
Results
All participants (100%) reported moderate levels of occupational stress, with a mean score of 92.47 (SD = 5.92). The highest stressors were related to workload and role conflict, including excessive job demands and conflicting responsibilities (M = 4.07 and 3.81, respectively). Moderate stressors included time pressure and limited autonomy, while low-stress areas were associated with interpersonal respect and role clarity. No statistically significant associations were found between occupational stress scores and demographic variables such as age, gender, marital status, job title, or work experience (p > 0.05). The uniform moderate-stress scores may reflect cultural response tendencies toward avoiding extreme ratings, desensitization to chronic stress, or potential limitations in the sensitivity of the HSE scale in this context.
Conclusion
Nurses in Hebron face moderate occupational stress primarily due to systemic and organizational factors rather than personal demographics. These findings should be interpreted cautiously in light of study limitations, including the use of convenience sampling, a relatively small sample size, and possible cultural or contextual influences on self-reported stress. Interventions targeting workload management, supportive leadership, and work autonomy are recommended to mitigate stress and promote well-being.
Introduction
Occupational stress, broadly defined as the psychological and physiological strain experienced when the demands of the job exceed an individual's ability to cope, is increasingly recognized as a significant issue in the healthcare sector (Daniel, 2019; WHO, 2018). Nurses, as frontline caregivers, are particularly vulnerable to occupational stress due to the emotional, physical, and cognitive demands of their role. They are required to manage patient care, respond to emergencies, communicate effectively with patients and families, and adapt to high-stakes environments—all while maintaining composure and professionalism. Globally, factors such as excessive workload, staff shortages, lack of organizational support, and the emotional toll of caregiving contribute significantly to stress levels among nurses (Jeffery et al., 2023; Layali et al., 2019).
The consequences of occupational stress among nurses are profound. Chronic exposure to stress can lead to burnout, emotional exhaustion, reduced job satisfaction, absenteeism, and even attrition from the profession. Moreover, high levels of occupational stress can negatively impact the quality of patient care, increasing the likelihood of medical errors, impaired communication, and reduced patient satisfaction (Fang et al., 2022). These outcomes not only compromise the health and well-being of nurses but also affect the safety and efficacy of healthcare delivery.
In Palestine, the nursing workforce faces stressors that go beyond the typical challenges encountered in more stable healthcare systems. Nurses in the West Bank, including Hebron, work within a health infrastructure that is often under-resourced, understaffed, and heavily impacted by political instability and economic constraints. According to the Palestinian Ministry of Health (2021), the nurse-to-population ratio remains significantly below global recommendations, with approximately two nurses per 1,000 people. This shortage places excessive demands on existing staff and compromises the overall quality of care.
Furthermore, Palestinian nurses often operate in high-pressure environments marked by limited access to medical supplies, overcrowded wards, and inadequate administrative support. The cumulative effect of these stressors, exacerbated by the broader socio-political climate, can lead to chronic occupational stress. Nurses may also face moral distress when they are unable to provide adequate care due to resource limitations or are forced to work under conditions that conflict with professional standards.
Cultural and gender-related expectations may add further complexity. Female nurses, who comprise a substantial portion of the nursing workforce in Palestine, often bear dual responsibilities as healthcare providers and primary caregivers at home, adding to their emotional and physical burden. These stressors may remain unrecognized and unaddressed within the system, further perpetuating workplace dissatisfaction and mental health issues among nursing staff.
Despite the well-documented consequences of occupational stress in nursing, there is limited empirical evidence on the phenomenon within the Palestinian context, particularly in the city of Hebron. While international studies have extensively explored work-related stress and its correlates among nurses, the majority focus on high-income or politically stable settings. Research from conflict-affected regions, such as Palestine, remains scarce and fragmented.
Existing Palestinian studies have generally focused on broader occupational health issues, often overlooking the specific stressors unique to the nursing profession. Furthermore, most available data do not sufficiently explore the potential influence of demographic and workplace factors—such as age, gender, experience, job position, or work shifts—on the prevalence and intensity of occupational stress. This lack of localized research limits the ability of healthcare policymakers and administrators to develop effective interventions tailored to the realities of Palestinian nurses.
Given these gaps, there is a critical need to examine occupational stress among nurses in Hebron hospitals. Hebron is one of the largest and most populous cities in the West Bank, home to several major healthcare facilities that serve a large and diverse patient population. Nurses working in these hospitals face considerable workload pressures and challenging conditions that likely contribute to high stress levels.
The present study aims to assess the prevalence of occupational stress among nurses in Hebron hospitals and to identify key stressors contributing to this phenomenon. Additionally, the study explores potential associations between occupational stress and various socio-demographic and work-related factors, such as age, gender, marital status, academic qualifications, job title, years of experience, and work schedule.
By providing context-specific data, this study seeks to fill a critical gap in the literature and offer evidence-based recommendations for reducing stress and improving the work environment for nurses in Palestine. Understanding the unique stressors faced by Palestinian nurses is essential to ensuring their well-being, enhancing job satisfaction, and ultimately improving the quality of care delivered to patients.
Literature Review
Occupational stress among nurses has been widely researched across different healthcare contexts, highlighting its multifactorial origins and adverse implications. Globally, studies report that nurses are disproportionately affected by occupational stress compared to other healthcare workers due to the intensity and emotional labor inherent in their roles (Kakemam et al., 2019). Various frameworks have been developed to assess work-related stress, including the Health and Safety Executive (HSE) model, which identifies key dimensions such as workload, control, support, role clarity, and interpersonal relationships as critical determinants of stress (Akbari et al., 2017).
Workload consistently emerges as one of the most prominent stressors. Nurses often operate under time pressure with high patient-to-nurse ratios, leading to physical exhaustion, emotional fatigue, and compromised patient care (Asseri et al., 2021; Qtait, 2025). Fang et al. (2022) noted that newly recruited nurses experience higher levels of stress due to performance expectations and inadequate preparation. Meanwhile, more experienced nurses face burnout from sustained overwork and limited career advancement opportunities.
Autonomy and decision-making control are also significant contributors to stress. Lack of authority in clinical decisions, rigid institutional hierarchies, and limited involvement in organizational planning can lead to frustration and a diminished sense of professional fulfillment (Layali et al., 2019). Nurses who feel disempowered often report lower job satisfaction and increased intention to leave the profession.
Interpersonal dynamics within the workplace play a dual role. Support from colleagues and supervisors has a protective effect against stress, while poor communication, bullying, or lack of recognition exacerbates it (Jeffery et al., 2023). Studies in low- and middle-income countries indicate that peer support is often informal and inconsistent, particularly in overburdened public health settings.
Work schedules and shift patterns have also been linked to stress outcomes. Night shifts and irregular rotations are associated with disrupted sleep, increased fatigue, and higher levels of occupational stress (Opoku Agyemang et al., 2022). Moreover, the cumulative effect of overtime hours—often unpaid or undercompensated—contributes to long-term dissatisfaction and emotional distress.
Despite a robust body of literature in high-income countries, fewer studies have examined occupational stress among nurses in politically fragile or resource-constrained settings. In the Middle East and North Africa (MENA) region, research is growing but remains limited in scope and depth. A study by Al-Amer et al. (2022) in Jordan found high prevalence rates of stress, particularly among nurses working in public hospitals, and emphasized the impact of systemic inefficiencies on mental health.
In Palestine, available studies tend to focus broadly on healthcare workers or students rather than nurses specifically. Qaraman et al. (2022) highlighted knowledge gaps in occupational health and safety among nursing students in Gaza, suggesting inadequate training as a contributing factor to future workplace stress. However, empirical studies focusing on practicing nurses—especially in cities like Hebron—are lacking.
This absence of localized data represents a critical gap. Without region-specific evidence, policymakers cannot develop effective interventions tailored to the actual stressors affecting Palestinian nurses. Therefore, further research is essential to quantify stress levels, identify primary risk factors, and inform workforce policies in fragile healthcare systems such as Palestine's.
Aim of the Study
This study aimed to assess the level of occupational stress among nurses working in Hebron hospitals and identify key stressors and associated demographic and occupational risk factors.
Methods
Study Design and Setting
This study utilized a cross-sectional descriptive design to assess the prevalence and contributing factors of occupational stress among nurses. Data were collected between December 2023 and March 2024 across four hospitals in Hebron, West Bank, Palestine. These hospitals—Hebron Governmental Hospital, Al-Muhtaseb Governmental Hospital, Al-Mezan Hospital, and the Palestinian Red Crescent Hospital—represent both governmental and non-governmental healthcare sectors and serve diverse patient populations.
Study Population and Sampling
The target population consisted of registered nurses employed at the selected hospitals, with a minimum of one year of clinical experience. Nurses on extended leave during the data collection period were excluded.
A non-probability convenience sampling technique was employed due to logistical constraints and the lack of access to a complete registry of hospital nurses. While this method enabled practical and timely data collection, it introduces potential selection bias, limiting the generalizability of findings to the broader population of nurses in Palestine. This limitation is further discussed in the study's discussion section.
A sample size of 408 nurses was initially calculated using Cochran's formula with a 95% confidence level and 5% margin of error. However, due to administrative restrictions and participant availability, 140 nurses were ultimately recruited, yielding a response rate of approximately 34.3%. No formal power analysis was conducted for the final sample size, which may affect the statistical power and robustness of the inferential analyses. Readers are advised to interpret subgroup comparisons with caution, particularly where effect sizes are small or statistically non-significant.
Instrument and Cultural Adaptation
Data were collected using a structured, self-administered questionnaire comprising two sections: demographic and work-related variables, and the 34-item Health and Safety Executive (HSE) Stress Scale. This scale assesses multiple dimensions of work-related stress using a 5-point Likert format (1 = never to 5 = always). A higher score indicates a greater level of occupational stress.
Given the bilingual context of Palestine, the questionnaire was made available in both English and Arabic. The HSE scale was translated into Arabic following standard translation-back translation procedures by bilingual experts in nursing and psychology. To ensure translation equivalence, the Arabic version underwent pilot testing with a small group of nurses (n = 10) not included in the final sample. Feedback was used to refine ambiguous items and ensure cultural relevance and conceptual clarity. The final Arabic version achieved acceptable internal consistency (Cronbach's alpha = 0.78).
Ethical Considerations
Ethical approval was obtained from the institutional review board of the College of Nursing at Palestine Polytechnic University and the Palestinian Ministry of Health. Informed consent was secured from all participants. Confidentiality was ensured through anonymous data collection, and no identifiable information was recorded.
Data Collection and Analysis
Participants received paper-based questionnaires in sealed envelopes. Each respondent completed the form in a quiet setting, requiring approximately 10–15 min. Completed questionnaires were collected and stored securely.
Data were analyzed using IBM SPSS version 23. Descriptive statistics (frequencies, percentages, means, and standard deviations) were used to summarize participant characteristics and occupational stress levels. Inferential statistics included independent sample t-tests and one-way ANOVA to explore group differences. Multiple linear regression was employed to identify predictors of occupational stress. A p-value of < 0.05 was considered statistically significant.
Results
From Table 1 presents the demographic profile of 140 participating nurses. The majority were young adults ( ≤ 35 years, 77.9%) and female (57.9%). Most held bachelor's degrees (66.4%), were married (75%), and worked in government hospitals (62.9%). Over half had more than five years of experience and 41.4% reported working overtime.
Demographic Variables of the Participants (n = 140).

Prevalence of Work Stress Levels among Participants
Based on the 34-item HSE Occupational Stress Scale, all 140 participants (100%) scored within the moderate stress range (M = 92.47, SD = 5.92), with no respondents scoring in either the low ( < 80) or high ( > 125) stress categories. The minimum and maximum scores ranged from 80 to 107. This lack of score variation raises important considerations regarding the sensitivity of the instrument, potential ceiling or floor effects, and the influence of cultural norms on response patterns. It is possible that participants may have avoided extreme ratings due to cultural tendencies toward moderation, or that the scale, despite prior validation, lacked nuance in detecting individual differences within this population as in Table 2.
Total Mean Sum Score of Work Related Stress (N = 140).

Thematic Grouping of Stressors
As in Table 3 originally presented item-by-item mean scores in isolation. For clearer interpretation, stressors have been regrouped into five subdomains aligned with the HSE framework: workload, role clarity and conflict, autonomy and control, managerial and peer support, and interpersonal environment.
Thematic Grouping of Stressors.

Demographic Variables and Occupational Stress
Despite analyzing a wide range of demographic and work-related variables, no statistically significant differences in occupational stress scores were observed across groups (all p > 0.05). However, notable trends merit discussion, especially in the context of a limited sample size as in Table 4.
Demographic Variables and Occupational Stress.
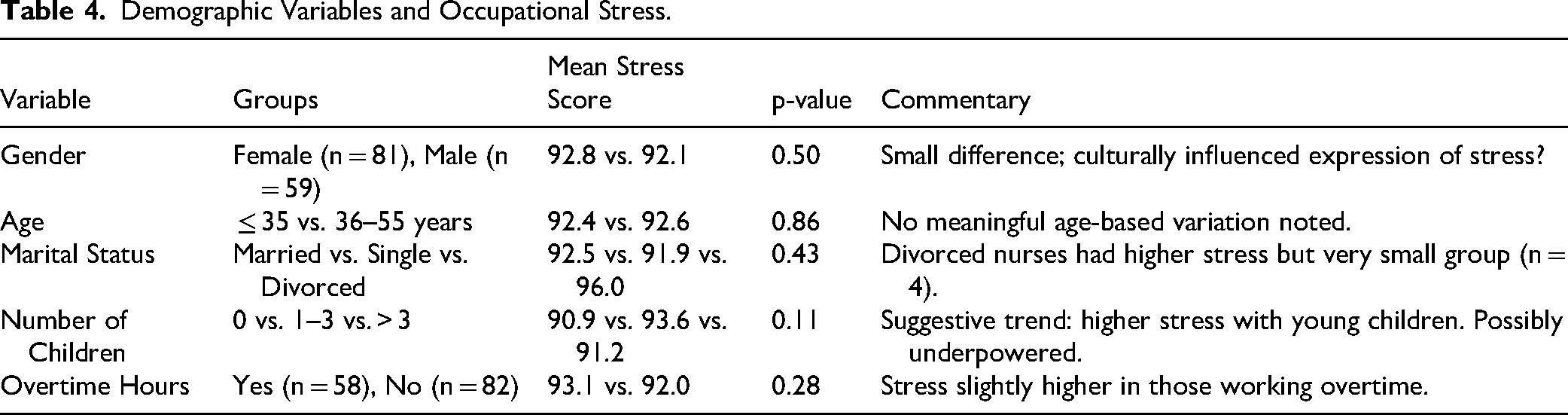
Although none of the p-values reached the standard threshold of 0.05, several were approaching significance (e.g., number of children at p = 0.11), suggesting the potential for meaningful effects that may be masked by limited statistical power.
Regression Analysis
A multiple linear regression model was applied to assess whether any demographic or work-related characteristics significantly predicted stress scores. The model included gender, age, marital status, children, academic level, job title, work schedule, and overtime in Table 5.
Regression Analysis.

The model was not statistically significant overall (F = 1.24, p = 0.28), and no single variable independently predicted occupational stress. However, beta values for number of children and overtime hint at small but possibly real effects. With a larger sample, these trends may reach significance.
All nurses reported moderate stress, with no low or high scorers—raising questions about scale sensitivity, social desirability, or cultural response patterns. Workload and role conflict were the most prominent stressors. Supportive interpersonal relationships were seen as relatively low stress factors. No demographic variables significantly predicted stress, but children and overtime showed noteworthy trends. Regression analysis did not identify any significant predictors, but effect sizes suggest potential associations.
Discussion
This study found that nurses working in Hebron hospitals experience moderate levels of occupational stress, with no respondents falling into low or high stress categories. While moderate stress is commonly reported in nursing literature, the complete absence of variation in stress levels in this sample warrants critical examination. One explanation may be cultural response bias or a tendency to avoid extreme answers in self-report tools due to social norms emphasizing modesty or emotional control (Al-Amer et al., 2022). This phenomenon may also reflect desensitization to chronic stress in high-pressure environments, where nurses have adapted to systemic challenges and report stress as a normalized part of their professional life.
Another possible explanation lies in instrument sensitivity. Although the Health and Safety Executive (HSE) scale is widely validated, it may have ceiling or floor effects when applied in politically fragile or culturally unique contexts such as Palestine. Limited variation in scores suggests that while the tool captures generalized stress, it may lack sensitivity to more nuanced experiences of psychological strain among nurses in conflict-affected areas (Akbari et al., 2017; Qaraman et al., 2022).
The study's findings align with Qaraman et al. (2022, stress and coping theory, which highlights that stress arises from the interaction between environmental demands and an individual's perceived capacity to cope. Nurses in Hebron face high workloads, role conflict, and time pressure, but may rely on emotion-focused coping strategies such as normalization or compartmentalization, especially in the absence of institutional support. Similarly, (Layali et al., 2019) job demand-control model helps explain the high-stress environment: the combination of high job demands with low decision-making autonomy and control is strongly predictive of occupational strain. In this study, nurses reported limited autonomy regarding rest breaks and work flexibility, suggesting low job control.
Notably, interpersonal relationships, including peer and supervisor support, were rated as lower stressors. This may reflect strong professional solidarity among Palestinian nurses, which can serve as a buffering factor against burnout (Jeffery et al., 2023). Despite this, supportive relationships alone may not compensate for the systemic stressors inherent in understaffed and under-resourced healthcare systems.
Although no significant associations were found between occupational stress and demographic variables, several non-significant trends merit further discussion. For example, female nurses and those with children reported slightly higher stress levels. This aligns with research indicating that female nurses—especially in patriarchal or conservative societies—often experience dual burdens of professional duties and family caregiving roles, increasing their vulnerability to stress (Albelbeisi et al., 2021; Opoku Agyemang et al., 2022). These findings also resonate with the Person–Environment Fit model, which suggests that a mismatch between personal demands (e.g., caregiving responsibilities) and workplace resources contributes to strain and dissatisfaction (Daniel, 2019).
Overtime work also correlated with higher stress scores, although not significantly. This trend is consistent with global literature emphasizing that excessive work hours and staff shortages are key contributors to emotional exhaustion and job dissatisfaction among nurses (Asseri et al., 2021; Kakemam et al., 2019). In the Palestinian context, this issue is compounded by political instability, limited mobility, and inadequate healthcare infrastructure, which place additional strain on nurses’ roles and performance (Albelbeisi et al., 2021; Ministry of Health, 2021).
The findings underscore the need for systemic, not just individual-level, interventions. Hospital managers and healthcare policymakers in Hebron should prioritize the implementation of workload reduction strategies, including improved nurse-to-patient ratios, scheduled rest breaks, and realistic shift rotations. Leadership training for supervisors, coupled with stress management workshops and peer support programs, may also foster a healthier work environment (Jeffery et al., 2023; WHO, 2018). Importantly, policies should be gender-sensitive, recognizing and accommodating the caregiving burdens faced by many female staff members.
In summary, this study reveals a healthcare environment where nurses operate under persistent, moderate stress, shaped more by institutional and systemic constraints than by personal or demographic differences. It calls attention to the complex interplay of cultural, organizational, and contextual factors influencing occupational stress and highlights the limitations of universal tools and models when applied without cultural adaptation. Addressing these challenges requires tailored, context-specific strategies that account for the unique socio-political and cultural realities of Palestinian nurses.
Strengths and Limitations
Several limitations should be acknowledged. The use of convenience sampling and the limited sample size reduce the generalizability of the findings. Additionally, the uniform moderate stress scores suggest potential measurement issues, including cultural response tendencies and linguistic ambiguities in the translated tool. Future studies should ensure stronger cultural adaptation of instruments through methods such as cognitive interviewing and should consider qualitative or mixed-method approaches to gain richer insights into how nurses conceptualize and cope with occupational stress. Further research should also explore coping mechanisms, gender-specific challenges, and the impact of systemic constraints—such as resource shortages and political instability—on nurse well-being. Longitudinal designs may help track how stress levels evolve in response to interventions or changing healthcare conditions.
Despite these limitations, this study has notable strengths. It addresses a critical gap by examining occupational stress among nurses in Hebron, Palestine—a politically unstable and under-researched setting. The use of a culturally adapted and pilot-tested version of the validated HSE Stress Scale ensured relevance to the local context. Data were collected from both governmental and non-governmental hospitals, enhancing representativeness. The inclusion of demographic and work-related variables, combined with comprehensive statistical analyses, provided nuanced insights. Ethical rigor, a high response rate, and transparent reporting further strengthen the credibility and applicability of the findings for nursing policy, workforce planning, and targeted interventions.
Practical Implications
Despite these limitations, the study's findings provide several actionable insights for hospital administrators. The consistently moderate stress levels observed among participants indicate that occupational stress is a systemic issue, rather than one confined to specific departments or individuals. This underscores the need for institutional reforms that address organizational factors, rather than relying solely on individual-focused stress management strategies.
Hospital managers should consider implementing staffing policies aimed at reducing excessive workloads and overtime, thereby alleviating one of the most common sources of nurse burnout. Increasing nurses’ decision-making autonomy—such as involving them in scheduling and operational decisions—may foster a greater sense of control and job satisfaction. Additionally, providing on-site psychological support, including peer counseling and debriefing sessions for high-stress units, can offer immediate relief and build resilience.
Conclusion
This study found that nurses working in Hebron hospitals experience moderate levels of occupational stress, with an average stress score of 92.5. The most significant stressors were related to workload, role conflict, time pressure, and limited decision-making autonomy. Conversely, factors such as interpersonal respect and role clarity were perceived as lower stressors. Despite the moderate stress level, no statistically significant associations were found between stress scores and demographic variables such as age, gender, marital status, years of experience, or job title. However, trends indicated slightly higher stress among female nurses, nurses with children, and those working overtime hours.
The results suggest that organizational and systemic factors, rather than individual characteristics, are the primary contributors to occupational stress in this population. These findings are consistent with previous studies conducted in similar healthcare settings facing resource limitations and staffing shortages.
To mitigate the impact of occupational stress, healthcare administrators and policymakers should focus on reducing nurses’ workload, improving staffing ratios, and implementing stress management interventions. Additionally, promoting supportive leadership and providing nurses with greater autonomy and sufficient rest time could further improve their well-being and work performance.
Future research should explore broader factors such as organizational culture, leadership practices, and coping mechanisms to provide deeper insights.
Supplemental Material
sj-docx-1-son-10.1177_23779608251374155 - Supplemental material for Occupational Stress and Associated Risk Factors Among Nurses in Hebron Hospitals: A Cross-Sectional Study from the West Bank, Palestine
Supplemental material, sj-docx-1-son-10.1177_23779608251374155 for Occupational Stress and Associated Risk Factors Among Nurses in Hebron Hospitals: A Cross-Sectional Study from the West Bank, Palestine by Yousef Jaradat and Mohammad Qtait in SAGE Open Nursing
Supplemental Material
sj-doc-2-son-10.1177_23779608251374155 - Supplemental material for Occupational Stress and Associated Risk Factors Among Nurses in Hebron Hospitals: A Cross-Sectional Study from the West Bank, Palestine
Supplemental material, sj-doc-2-son-10.1177_23779608251374155 for Occupational Stress and Associated Risk Factors Among Nurses in Hebron Hospitals: A Cross-Sectional Study from the West Bank, Palestine by Yousef Jaradat and Mohammad Qtait in SAGE Open Nursing
Footnotes
Acknowledgements
The authors would like to express their gratitude to the nurses who participated in this study and to the management of Hebron hospitals for their support and cooperation.
Ethical Statement
This study was conducted in accordance with ethical principles outlined by Palestine Polytechnic University ethical board. Ethical approval was obtained from Palestine Polytechnic, and informed consent was secured from all participants number (105,ppu.2024).
Author Contribution Statement
Yousef Jaradat and Mohammad Qtait contributed equally to the conception, design, data collection, analysis, and manuscript preparation of this study. Both authors reviewed and approved the final version of the manuscript.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.