
Abstract
Background
Occupational stress is a prevalent health issue that can have both clinical and psychological repercussions, impacting the quality of care of emergency nurses. However, more research is required to better understand the prevalence of this condition and its implications for the work capabilities of nurses in emergency departments.
Objective
To examine the relationship between occupational stress and the quality of care among emergencydepartment nurses at government hospitals in the Gaza Strip, Palestine.
Methods
A descriptive cross-sectional design was used to examine stress levels and quality of care using the convenience sampling technique between July and September 2023. Nurses completed a questionnaire comprising three parts: Emergency nurse stress questionnaire with 12 items, professional quality of life scale with 10 items, and demographic data with 9 items in three governmental hospitals in the GazaStrip. Statistical analysis was carried out using SPSS version 25.
Result
A total of 80 emergency nurses were included. The study showed an equal distribution of emergency nurses according to gender 50%. Furthermore, 42% of the nurses working at Al Shifa Medical Hospital, more than half 54%, had less than 5 years of experience. The overall average mean score for the level of stress among emergency nurses was 4.83 (SD = 1.078), Also, the overall average mean score quality of care for among emergency nurses was 2.51 (SD = 0.984).
Conclusion
This study indicates that there was a significant negative relationship between occupational stress at work and quality of care, indicating that as stress levels increase, factors that restrict quality of care also increase. Furthermore, the findings highlighted statistically significant differences in the mean score of occupation stress and age, sex, years of experience and shift of work. Based on these results, it is essential that health policymakers address the high levels of OS among emergency nurses to improve quality of care.
Introduction
Occupational stress (OS) in nursing is a very common health problem that affects physical, psychological, and social equilibrium Richardson & Rothstein (2008). Occupational stress has various factors that cause a high level of stress among emergency nurses, leading to negative significances such as absenteeism from work, general fatigue, anxiety, agitation, and low productivity, leading to a lack of quality of care Al-Nuaimi et al. (2021). Occupational stress or job pressure was defined as “harmful physical and emotional responses that occur when the requirements of a job do not match the resources, capabilities, and needs of the worker” Steinhoff, (2015).
Globally, emergency departments (ED) are the front line of the healthcare system, dealing with a wide range of trauma, damage, and agitation Nasr-Esfahani et al. (2017). Therefore, emergency nursing is known as a stressful occupation Jacobs & Lourens, (2016); Kordi et al. (2014). Emergency nurses (EN), who provide care in emergency departments (ED), are exposed to a comprehensive variety of stressors, including working under excessive pressure in active, volatile, war, accidents, and explosive environments Gholamzadeh et al. (2011). The results of several studies have shown that nurses working in hospital emergency departments experience varying degrees of psychological problems and social stress and may feel that their efforts are not acknowledged, appreciated, or rewarded Kordi et al. (2014); Nasiry Zarrin Ghabaee et al. (2016); and Ogińska-Bulik & Michalska, (2021). Occupation stress in nurses can affect both their quality of life and the quality of care they provide. The quality of care of emergency nurses, who are entrusted with human lives, is crucial, as it directly correlates with their ability to provide more effective services and better quality of care Layali et al. (2019). Occupational stress has now become the norm since the profession of contemporary nursing is evolving and while moderate levels of stress may be useful, the constant presence of chronic stress can take its toll on the health of nurses. This continuous stress can cause hypertension, resulting in cardiovascular diseases such as myocardial infarction (MI), ventricular fibrillation (VF), in addition to migraines, and irritable bowel syndrome (IBS). Some of these health problems can ultimately reduce the quality of the services that nurses offer to patients Bahrami, (2016); Steinhoff, (2015).
It is crucial to identify key stressors and assess the level of work stress experienced by nurses in emergency departments García-Izquierdo & Ríos-Rísquez, (2012). These stressors can lead to a significant reduction in nursing performance, resulting in a decrease in the quality of care provided by nurses in emergency departments due to secondary traumatic stress, nursing burnout, overtime, and the loss of experienced and skilled nurses (Xu et al., 2020). On the contrary, the ability to recognise these types of stressors and their causes can have implications for managing these stressors, and future studies can use this information to reduce job stress. Several studies have shown that it impacts care provision and patient outcomes, either directly or indirectly Babapour et al. (2022), Esmaiel Hajinezhad and Azodi (2014).
Emergency nurses in government hospitals in the Gaza Strip (GS) in Palestine are affected by stress that affects them physically, psychologically and socially. This stress arises from constant demands from superiors, high-demanding routine procedures, lack of human resources, absence of salaries and motivation, shortage of medical equipment, noise, current war, Israeli aggression due to the occupation siege, and the potential for death. These factors may create work conditions that are not suitable for nursing activities, leading to mood disorders, headaches, depression, agitation, and other symptoms. Additionally, the study intends to raise awareness among health decision makers to support these nurses in improving quality of care and to provide recommendations to health organisations for implementing preventive measures to reduce OS among emergency nurses. Furthermore, the study will propose additional research to intervene in stress among emergency nurses and examine its impact on quality of care.
Review of the Literature
Research by (Park & Kim, 2013) indicates that occupational stress is commonly experienced among nurses. In a related study by Lee et al. (2015), 27% of nurses were found to have psychophysiological stressors. Emergency department (ED) nurses reportedly exhibit higher levels of psychiatric symptoms compared to their counterparts in other hospital units. The emergency department serves as the front line of healthcare care, characterised by a wide range of trauma, agitation, and high levels of stress. Nurses in this environment often face significant daily stress and emotional stress, which adversely affects their health and decreases their work performance and overall productivity Abou Hashish & Ghanem Atalla, (2023) and Dall’Ora et al. (2020). A growing body of research highlights the direct and indirect effects of psychosocial elements on various metrics for nurses, including absenteeism, sickness absence, and general low quality of care (Li et al., 2019).
In a study involving 222 emergency department nurses, it was found that 27% of participants who reported high stress tended to use avoidant conflict management styles Johansen & Cadmus, (2016). Another investigation suggested that elevated work demands and limited job control correlate with higher educational levels among emergency department nurses Trousselard et al. (2016). Furthermore, workload emerged as a consistent predictor of perceived stress in a cross-sectional study involving French emergency department staff, revealing a more significant impact on physicians compared to nurses. Some junior physicians also reported related substance misuse issues (Lala et al., 2016).
After reviewing the literature, numerous studies have focused on the stress and exposure to violence experienced by emergency department nurses Su et al. (2009) and Talas et al. (2011). Furthermore, there have been few studies that examined the occupational health problems of nurses Aladini et al. (2023), Kilic et al. (2016). However, in (GS), Palestine, the number of studies that examine occupational health problems of nurses is very limited Alhajjar, (2013) and Jaradat et al. (2016). This gap in the literature highlights the need for more research. Consequently, the current study aims to examine the relationship between OS and quality of care among emergency department nurses in governmental hospitals in GS, Palestine.
Methods
Study Design, Period, and Setting
A multicenter institutional-based cross-sectional descriptive study was conducted among nurses employed working in the emergency department (ED) of three governmental hospitals, namely the “Al Shifa Medical Hospital”, “Al-Aqsa Martyrs Hospital” and “Nasser Medical Hospital”, GS, Palestine, from July to September 2023. The STROBE cross-sectional reporting guideline was followed.
Study Participants and Sampling Method
The target population of nurses employed consisted of 93 nurses working in emergency departments in three government hospitals in the GS, Palestine. The nurses were selected using a convenience sampling technique. The study sample included 80 nurses of both sexes, aged 25–60 years, who completed the questionnaire. An online sample size calculator tool of Raosoft software (Calculator, 2010). The sample size was determined through a power analysis. A significance level was established at 0.05, and a statistical power was established at 0.80. With an accepted error margin of 5%, a confidence interval of 95%, and a response distribution of 50%, the analysis indicated that a sample size of 80 would be adequate to detect meaningful effects within the nursing population. Consequently, the achieved response rate to the questionnaire was 90.2% of the population because the sample was collected using convenient techniques and face-to-face interviews, allowing us to exclude any nurse who refused to participate from the beginning of the data collection process. An informed consent option was displayed on the first page of the questionnaire, explaining the objectives and significance of the study. Emergency nurses were informed that participation in the study was voluntary and that the anonymity of the information was confirmed.
Inclusion and Exclusion Criteria
All eligible nurses who had worked in emergency departments in three government hospitals, received regular monthly salaries with at least one year of work experience, and had contact with patients, were eligible and available during the period from the beginning of July 05, to September 05, 2023, and were included in the study after accepting to participate. However, nurses who did not receive regular monthly salaries were newly recruited into the emergency department or were unpaid volunteers, as well as head nurses, excluded from the current study to avoid possible bias. Additionally, nurses who had worked in paediatric ICUs or were unable to participate due to their serious illnesses were excluded.
Data Collection
After obtaining approval from the general administration of the hospitals of the (Palestinian) Ministry of Health, a face-to-face interview with nurses was conducted to collect research data. Data were collected by five student nurses who distributed Arabic questionnaires in paper form to nurses who agreed to participate in the study, along with their instructions. The questionnaire took approximately 15–20 min to complete. The questionnaire data were collected over three months (from July 2023 through the end of September 2023).
Study Instrument
Data were collected using two primary tools:
The Emergency Nurse Stress Questionnaire
In the study, a self-report questionnaire was used designed to examine stress in emergency department nursing. The Emergency Nurse Stress Questionnaire, modified from the Operational Police Stress Questionnaire developed by Steinhoff (2015). It was composed of 12 questions. The scale consists of seven items and is scored on a seven-point Likert scale, with the score for each question ranging from one score (1- No stress at all) to seven scores (7- a lot of stress). The lowest possible score in this tool is 12, while the highest possible score is 84. Because this tool has been rewritten, a post hoc reliability analysis was performed as part of the study. The post hoc analysis indicated good reliability with Alpha Cronbach coefficients α = (0.84),
Professional Quality of Life Scale (Pro QOL) version V
In our study, the last part of the quality of life scale was used. This scale was initially created by Flanagan (1978) and measured a person's sense of well-being by Burckhardt and Anderson (2003). The tool has since been adapted to assess different residents as care providers. The scale used for this study is the fifth version. It has been used in various nursing research. The Professional Quality of Life Questionnaire Scale (Pro QOL) is a 10-question scale. The scale consists of six items and is scored on a 6-point Likert scale, the score for each question ranging from one score (0 = never) to six scores (5 = very often). The lowest possible score on this tool is 0, while the highest score is 50. The internal consistency of the version V Professional Quality of Life Scale (Pro QOL) was achieved using the Alpha Cronbach coefficients α = 0.859, which means that the Arabic version of this questionnaire is a reliable instrument for use with Palestinian nurses in the emergency department. The validity of the content of the translated instruments was reviewed by a panel of seven experts, including academic and specialist emergency nurses, to verify the validity of the content.
In addition to the tools mentioned above, the demographic and professional information of the emergency nurse included sex, age, marital status, qualification, years of experience, nature of shift, number of shifts at night, and work hours at night. It was made up of 9 items.
Pilot Study
A pilot study was carried out on 10% of the total study sample of emergency nurses 8 before the data collection technique, to confirm the acceptance of the survey. In this sense, acceptance means the nurses’ understanding of the survey questions, the perceived importance of the survey, and their willingness to participate in the study. The findings of this pilot study informed the final survey instrument to ensure clarity and appropriateness for the target population.
Ethics Approval
The study protocol was approved by the Palestinian Health Research Council (Departmental Health ResearchUnit of the Palestinian Ministry of Health, Gaza Strip) (Code No.: MOH 1264358/2023). Additionally, written informed consent wasobtained from each of the emergency nurses prior to the study.
Statistical Analyses
After data collection, the responses were coded according to the questions to facilitate statistical analyses. The Statistical Package for Social Sciences software, version 25 was used. Descriptive and inferential statistics were used to summarise the demographic data of emergency nurses. Frequencies and percentages were used to describe different categorical variables, while means and standard deviations (SD) were used to represent continuous variables. The chi-square (χ2) test was used to examine the relationships between categorical variables, an independent samples t-test was applied to compare the means of two groups, and a one-way ANOVA test was used to compare the means between three or more groups. Furthermore, the researchers used Pearson's correlation to establish the correlation between occupational stress and quality of care, with a significance level of p < 0.01 as highly significant. The mean scores were taken as a deadline, as was used in similar preceding research Steinhoff, (2015), which means that the score for the mean is considered as low levels of quality of life and the score above the mean is considered as high levels of quality of life. A p-value less than 0.05 was considered statistically significant.
Results
Characteristics of Emergency Department Nurses
The statistical population of the study consisted of 80 emergency department nurses (92%) response rate with a mean (SD) age of 30.78 (7.305) years, The characteristics of the samples are presented in Table 1. Equal distribution of emergency nurses according to sex, since 50% were male and 50% were female nurses, (47%) were in the age group between 20 and 25 years old. In terms of marital status, more than half of the nurses (58.8%) were married and nearly half (48.8%) had a bachelor's degree, and 42.4% of the nurses worked at Al Shifa Medical Hospital, 23.8% at Al-Aqsa Martyrs Hospital and 33.8% at Nasser Medical Hospital. More than half of the nurses (53.7%) reported having less than 5 years of experience in their current roles. In terms of employment status, more than two thirds of nurses (81.2%) work rotating shifts, including day, evening, and night shifts. Furthermore, 65.0% of the nurses reported working 4-night shifts and more in the last month and 58.8% worked 12 h at night shifts (Table 1).
Demographic Characteristics of Nurses in the Emergency Department in Government Hospitals.
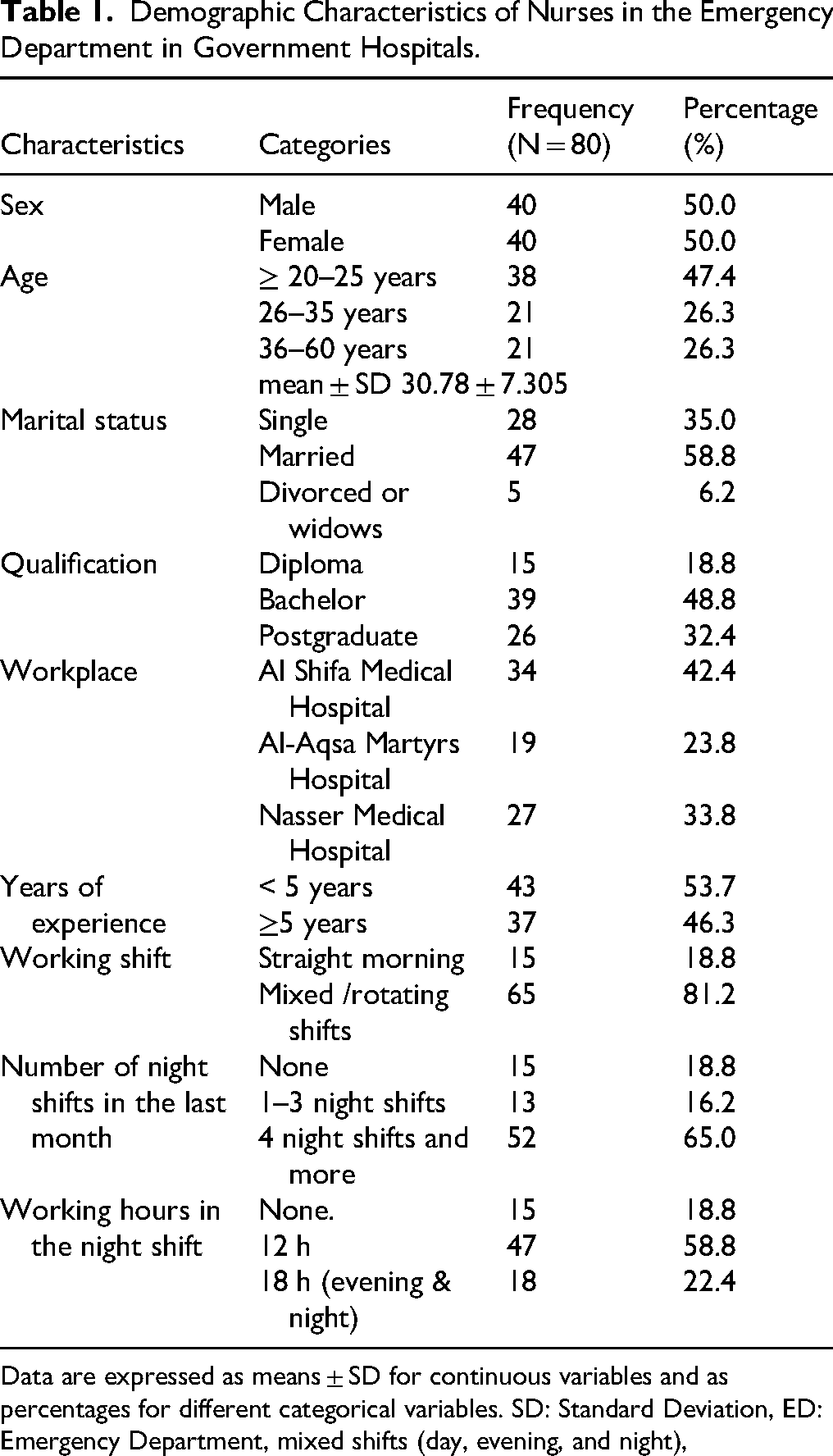
Data are expressed as means ± SD for continuous variables and as percentages for different categorical variables. SD: Standard Deviation, ED: Emergency Department, mixed shifts (day, evening, and night),
Level of Stress among Emergency Department Nurses
The highest score was “feeling like you are always on the job”, which had a mean score of 5.33 (SD = 1.734) and a mean percentage of 76.1%. On the other hand, the lowest score was in “making friends outside of work,” with a mean score of 4.54 (SD = 1.821) and a mean percentage of 64.8%. The overall average mean score for occupational stress was 4.83 (SD = 1.078), resulting in a mean percentage of 69%, which indicated a moderate level of OS among the nurses surveyed (Table 2).
Level of Stress among Emergency Department Nurses.

Data are expressed as means ± SD for continuous variables and as percentage (%) for different categorical variables.
Abbreviations SD: Standard Deviation; MVA: Motor vehicle accident.
Quality of Care among Emergency Department Nurses
As shown in Table 3, the highest score was associated with the statement “I’m preoccupied with more than one person I help”, with a mean score of 4.08 (SD = 1.156), which corresponds to a mean percentage of 81.6%. In contrast, the lowest score was found for the statement “As a result of my help, I have intrusive, frightening thoughts”, which had a mean score of 2.04 (SD = 1.571) and a mean percentage of 40.8%. These scores collectively highlight an overall average mean score of 2.51 (SD = 0.984), with a mean percentage of 50.2%, indicating a moderate level of restricting factors to quality of care among emergency nurses (Table 3).
Quality of Care among Emergency Department Nurses.
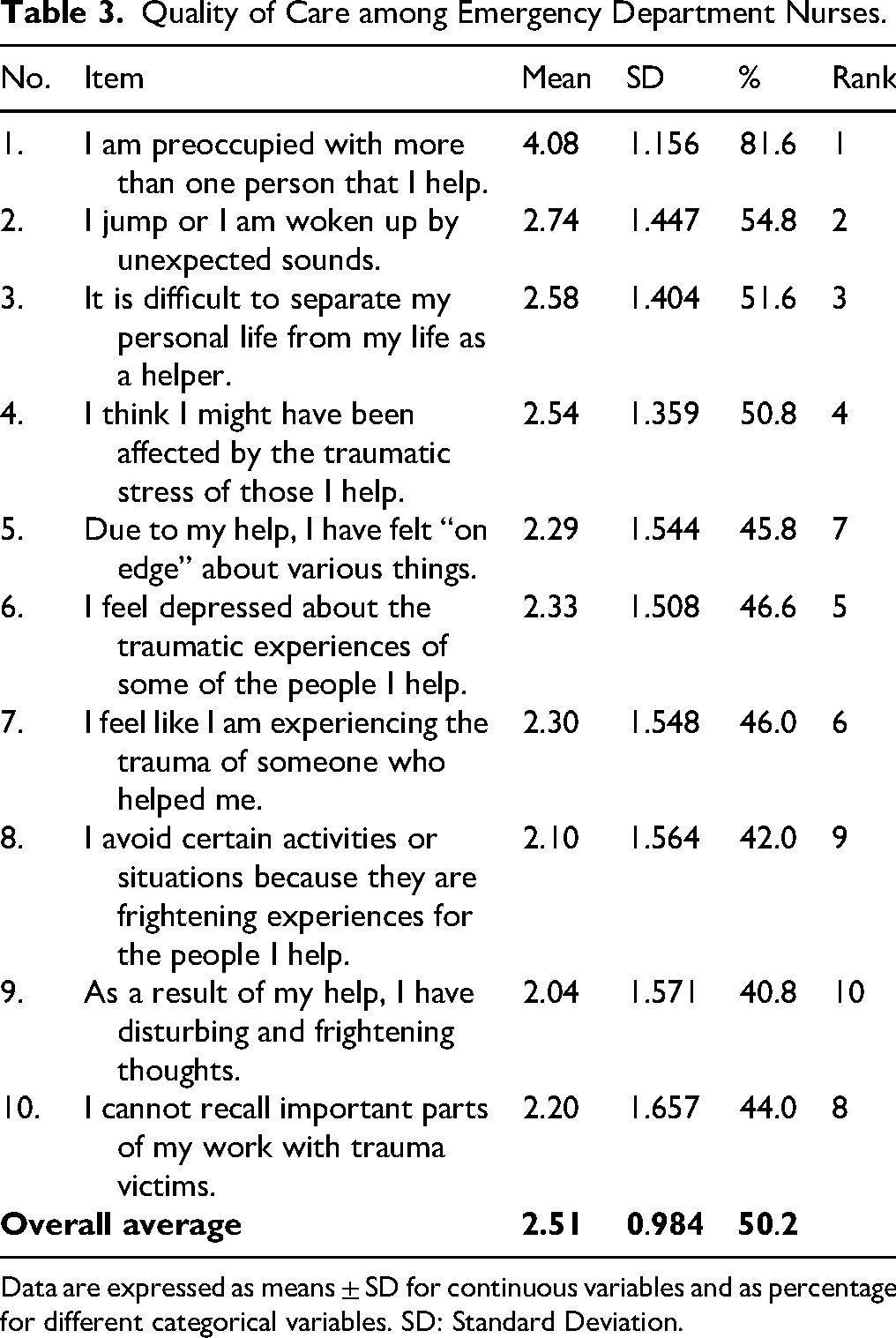
Data are expressed as means ± SD for continuous variables and as percentage for different categorical variables. SD: Standard Deviation.
The Correlation Between Occupation Stress and Quality of Care
To find the relationship between occupational stress (OS) and quality of care among emergency nurses, the authors used Pearson's correlation test as presented in Table 4, which shows that there was a significant negative relationship between OS at work and quality of care. Specifically, Pearson's correlation coefficient was found to be 0.539 (p < 0.01), this means that as occupational stress levels increase, factors that restrict quality of care also increase (Table 4).
Correlation Between Occupation Stress and Quality of Care.

Note. Values reported using Pearson's correlational, abbreviations: SS = statistically significant (*p = <0.05), HS = highly significant (**p = <0.01).
Differences in Occupation Stress and Quality of Care Related to Demographic Characteristics of Emergency Department Nurses
The authors used the (t) test and the one-way ANOVA test to find differences in nurses’ perception of stress at work and quality of care. As presented in Table 5, there were statistically significant differences in OS level related to the age of the nurses (F = 3.865, P, 0.025), while there were statistically no significant differences in quality of care (F = 1.274, p = 0.286), which shows that there were statistically significant differences in the mean OS score (–2.831, p = 0.006) and quality of care (m = -2.373, p = 0.020) related to sex. These results indicated that female nurses had significantly higher OS and significantly higher factors that restrict their quality of care. This finding indicated that there were no statistically significant differences in mean occupational stress scores (OS) (F = 0.091, p = 0.913) and quality of care (F = 0.336, p = 0.715) related to marital status, relative to marital status. This suggests that marital status does not affect occupational stress or quality of care. Furthermore, it showed that there were statistically no significant differences in the mean OS score (F = 0.287, p = 0.751) and quality of care (F = 0.515, p = 0.599) between hospitals, which means that the place of work has no effect on OS and quality of care. Regarding the qualifications, the results indicated that there were no significant differences in the mean OS score (F = 0.240, p = 0.787) and quality of care (F = 0.502, p = 0.607) related to the level of education, which means that the level of education does not have an effect on OS and quality of care. Additional findings with respect to years of experience showed that there were statistically significant differences in the level of OS related to years of experience (t = 2.072, P, 0.042), which means that nurses with a 5-year experience of < 5 years experienced greater stress compared to nurses with more years of experience. The results also showed that there were statistically no significant differences in quality of care related to years of experience (t = 0.865, p = 0.390). This finding indicated that there were statistically significant differences in the mean OS score (−5.252, p = 0.000) and quality of care (m = -2.062, p = 0.043) related to the type of shift of work. These results indicated that nurses who work mixed shifts (day, evening, night) had significantly higher OS and significantly higher factors that restrict their quality of care. The results also showed that there were statistically no significant differences in the mean OS score (t = -1.203, p = 0.233) and quality of care (t = 0.032, p = 0.975) related to the number of night shifts in the last month, which means that the number of night shifts does not have an effect on OS and quality of care. The last finding indicated that there were statistically no significant differences in the mean OS score (1.419, p = 0.161) related to the length of the working hours. The results also showed that there were statistically significant differences in quality of care (m = 2.024, p = 0.047) related to the length of work hours, which means that nurses who work 12 h shifts had significantly higher factors that restrict their quality of care compared to nurses who work 18 h shifts (Table 5).
Differences in Occupation Stress and Quality of Care Related to Demographic Characteristics of Emergency Department Nurses.

Data are expressed as means ± SD for continuous variables. The chi-square test was used to examine differences in the prevalence of different categorical variables. Differences between means were tested using an independent sample t test and one-way analysis of variance (ANOVA). SD: Standard deviation. ED: Emergency Department. A P-value less than 0.05 was considered statistically significant.
Discussion
Globally, occupational stress (OS) was defined as “harmful physical and emotional responses that occur when the requirements of a job do not match the resources, abilities, and needs of the worker” Richardson & Rothstein (2008). In Palestine, several factors, such as anxiety, agitation, fear of being injured due to ongoing conflicts or genocide, lack of adequate medical equipment, continued siege, and a shortage of caregivers, were identified as the most common causes of OS, which in turn leads to a decrease in quality of care among nurses in the emergency department. This study was to examine the relationship between OS and quality of care among emergency department nurses in government hospitals in GS, Palestine.
The general average mean stress level among emergency department nurses was 4.83 (SD = 1.078), with a mean percentage of 69%, indicating that nurses generally reported a moderate level of OS at work in the emergency department. These results were similar to studies reported in Southern California by Steinhoff, (2015), who found a high level of OS among emergency nurses, with a mean of 162.28 (SD = 35.28), and by Alshammari et al. (2022), who found generally moderate to high levels of OS among emergency nurses at King Fahd Specialist Hospital in Saudi Arabia. Similarly, a study conducted in Libya by Eltarhuni (2016) reported that the overall level of stress among nurses is relatively high. Therefore, it can be concluded from previous and present studies that healthcare managers should develop successful plans to improve the quality of life at work. This will help improve both the home and work environments. Dzeng (2016) in his study explained that the nurse's work to balance the interference relationship systematically improved satisfaction with familial relativity. The study affirms that when nurses can effectively manage their professional and personal lives, they have less stress and more commitment to home care.
According to another finding in the present study, the overall mean quality of care score among emergency department nurses was 2.51 (SD = 0.984), with a mean percentage of 50%, indicating a moderate level of factors that restrict factors to quality of care. This finding is consistent with the results of other studies (Kordi et al., 2014; Nasiry Zarrin Ghabaee et al., 2016) in Mashhad, Iran.
A review of the literature revealed that the mean overall quality of care scores in this study were lower than those of other studies conducted by (Kordi et al., 2014; Nasiry Zarrin Ghabaee et al., 2016). Furthermore, factors contributing to this decline in quality of care, such as heavy workloads, long work hours, lack of support, inability to quit work, and lack of rest, can cause physical harm to nurses, diminish their quality of care, and increase stress and tension on the job. The reason for this stress can be due to the workload of nurses during the day, as they are responsible for multiple patients simultaneously.
This study revealed a reverse correlation between OS and quality of care; the current study showed that a significant negative correlation was found between the level of OS stress at work and quality of care, which means that as OS levels increase, the factors that restrict quality of care also increase. The findings of this study were consistent with the findings of several studies by Knezevic et al. (2011) and Golubic et al. (2009) and in Iran by Mosadeghrad et al. (2011). They reported that nurses with severe OS had lower quality of care scores. Therefore, improving the quality of care of nurses will ultimately lead to reduced job stress. To address these issues, it is recommended that coping strategies, such as stress management training and employee assistance programmes, be used to improve and support emergency nurses.
Regarding the demographic characteristics of emergency department nurses, the finding of the present study illustrates that a significant difference was found between the age of nurses, gender, years of experience and working shift, and the level of OS stress (p = 0.025, 0.006, 0.042, and 0.000), respectively. These findings were similar to studies conducted by Alenezi et al. (2018), which revealed that the age of a nurse is the most significant factor contributing to increased stress in government hospitals. On the other hand, this finding was inconsistent with that of a study by Mehrabi et al. (2008) and several studies Gheshlagh et al. (2017); Mojdeh et al. (2008) and Mortaghi, (2011) there was no significant relationship found between age and job stress.
These findings were consistent with studies conducted by Adeb-Saeedi (2002); Babapour et al. (2022); and Jafari et al. (2012) showed that work stress had a significant relationship with gender. However, this finding was inconsistent with those of a study conducted in Saudi Arabia (Alshammari et al., 2022) and another study in Kampala, Uganda Nabirye et al. (2011), which indicated that there were no significant differences between gender and the level of stress among emergency nurses. Perhaps the difference between the roles of men and women in Palestinian society explains this finding. Men can also be stated to be less stressed because they have more experience with explosive injuries in emergency crises due to recurrent war crimes in GS, making them feel more responsible towards patients.
The current study showed that a significant difference was found between the years of nursing experience and the level of OS (p = 0.042). These findings were similar to studies conducted by Kebapçı and Akyolcu, (2011); Moustaka and Constantinidis, (2010) who reported that nurses experience more job stress in emergency departments due to the high workload and care given to critically ill patients. Emergency departments are particularly stressful work environments; Healy and Tyrrell (2011). Furthermore, with increasing work experience, the level of OS was higher, indicating a relationship between OS and years of experience.
In the findings of the present study, a significant difference wa found between the different shifts (p = 0.000). These findings indicate that working a night or a rotational shift leads to higher stress levels for emergency nurses compared to the straight morning shift. This result is consistent with (Ameri et al., 2021), who identified different work shifts as sources of stress among nurses. Previous studies have also reported high levels of stress in rotational shift nurses, Gheshlagh et al. (2017). However, this finding contradicts other studies by Ameri et al. (2021; Rocha & Martino (2010), in which high stress levels were reported in nurses on straight morning shift nurses rather than in nurses on rotational shifts. In fact, in GS, many factors contribute to the increase in stress levels among nursing staff. For example, most of the current wars in GS occur suddenly at night. Consequently, stress levels increase during night shifts due to the heavy workload. They are responsible for caring for several patients with various critical conditions, including explosive cases or casualties. Furthermore, nurses often have to handle a large volume of cases simultaneously, despite challenges such as equipment shortages and a shortage of nursing managers in government hospitals during night shifts. All of these factors contribute to the elevated levels of stress experienced by nursing staff.
Regarding the demographic characteristics of emergency department nurses and their quality of care, the analysis revealed that only gender, working shift and length of night shifts had a significant relationship with quality of care (p = 0.020, 0.043, and 0.047), respectively. In the findings of the present study, a significant difference was found between the gender of emergency department nurses and the quality of care provided, these findings are similar to those reported by Al Mutair et al. (2022). This highlights the need for the government hospital to develop suitable policies that support the dependent individuals of the nurses in the emergency department. This may increase their responsibilities and, in turn, encourage their stabilisation and job satisfaction, thereby improving the quality of care. Interestingly, the current study did not reveal a significant relationship between quality of care and marital status. which is consistent with the findings of Dehghan Nayeri et al. (2011) also reported that there was no significant relationship between marital status and quality of care.
In terms of work shifts, the length of the night shift had a significant relationship with the quality of care. These findings are similar to those reported by Alharbi et al. (2019); and Venkataraman et al. (2018). Staff nurses working in emergency departments and those without night shifts exhibited better quality of care than nurses working in other units. Similarly, a study conducted in Taiwan revealed that nurses working in outpatient departments exhibited a better quality of care than nurses working in other units Venkataraman et al. (2018). This could be related to the fact that emergency departments generally require participation in shift duty at night and weekends, direct patient care, and work overload, which could result in a lower quality of care.
Nurses who work fewer hours per shift can have more time for family and social life and in return can lead to higher levels of quality of care. These findings could be explained by the fact that the participants in this study came from different sex groups. The diversity of the location of a sample could have impacted the appreciation of factors that nurses perceive as motivating or demotivating.
Strengths and Limitations
The main limitations of the current study were the design of the cross-sectional study and the convenience sampling technique, which involved a relatively small number of emergency nurses. Furthermore, this study was conducted in the Gaza Strip, Palestine, which is a region under siege, occupation, political instabilities, and ongoing conflict. These factors may have restricted the ability of this study to include a broad range of hospitals, possibly affecting the generalisation of the findings obtained. Despite that, the main strength of this study lies in its status as the first to include the use of the Emergency Nurse Stress Questionnaire and the Professional Quality of Care Scale, both of which were developed exclusively for staff nurses. Furthermore, the study involved a group of participants in the Palestinian context.
Implications for Practice
In light of that, the present study has established the importance of addressing OS among emergency nurses, as high OS levels are significantly correlated with reduced quality of care. Understanding clinical competence is crucial to improving patient outcomes in emergency contexts, and this study identifies factors that impact nursing performance. Various hospital administrators, health policymakers, nursing associations, and other stakeholders should focus on activities that promote clinical proficiency and general well-being among emergency nursing staff.
Stress regulation programmes such as engaging participants in self-care workshops, training, and access to mental health instruments make it possible to prevent the impacts of OS. Additionally, other possibly more specific interventions, while taking into account demographic characteristics- age, gender, years of experience, work shifts - could also help nurses cope with OS effectively. If implemented in healthcare institutions, such a policy will provide not only the well-being of emergency nurses, but also beneficial outcomes for patients as well.
Conclusion
This study indicates that the overall mean percent of the level of occupational stress among emergency nurses was 69%. Furthermore, the overall mean percentage of quality of care was 50%. A significant negative relationship between OS and quality of care, indicating that as stress levels increase, the factors that restrict quality of care also increase. Furthermore, the findings highlighted statistically significant differences in the mean OS score related to age, years of experience, and work shift, as well as gender differences in both OS and quality of care. However, no statistically significant differences in quality of care were found based on these variables. Based on these results, it is essential that health policymakers address high levels of OS among emergency nurses to improve the quality of care they provide. Therefore, more research is necessary in this critical area to refine these interventions and ensure that emergency nurses can operate at their optimal levels, which benefits both their well-being and patient care outcomes.
Data Collection
After obtaining approval from the general administration of the hospitals of the Palestinian Ministry of Health, a face-to-face interview with nurses was conducted to collect research data. Data were collected by five student nurses who distributed Arabic questionnaires in paper form to nurses who agreed to participate in the study, along with their instructions. The questionnaire took approximately 15–20 minutes to complete. The questionnaire data were collected over three months (from July 2023 through the end of September 2023).
Supplemental Material
sj-docx-1-son-10.1177_23779608251348827 - Supplemental material for The Relationship Between Occupational Stress and Quality of Care Among Emergency Department Nurses in Government Hospitals
Supplemental material, sj-docx-1-son-10.1177_23779608251348827 for The Relationship Between Occupational Stress and Quality of Care Among Emergency Department Nurses in Government Hospitals by Sae’d M. Abu El-Kass, Lama Abu El-Kass, Nasayem Alswarka, Sabah Abu Behiri, Aysha Alderawy, Tahreer Abu El Khair, Maram Alaraj and Nibal Aldahdouh in SAGE Open Nursing
Footnotes
Acknowledgements
The authors thank the general directors of hospitals of the Ministry of Health of GS, Palestine, as they paved the way for the study by giving approval for data collection. In addition to the University and College of Applied Sciences (UCAS), Faculty of Nursing and Health Sciences, Department of Nursing. We also thank emergency nurses who have agreed to participate in our study.
Ethics Approval
The study protocol was approved by the Palestinian Health Research Council (Departmental Health Research Unit of the Palestinian Ministry of Health, Gaza Strip) (Code No.: MOH 1264358/2023). Additionally, written informed consent was obtained from each of the emergency nurses prior to the study.
Authorship Statement
All authors listed meet the authorship criteria. All authors approved the final version and agreed with the content of the manuscript for submission. The exact authors’ contributions were as follows:
S.K. Conceptualization, Investigation, Formal Analysis, methodology, Project Administration, Validation, Original Draft, Writing-review & Editing.
L.K. Conceptualization, Investigation, Methodology, Validation, Original Draft, Writing-review & Editing.
N.A. Methodology, Investigation, Writing-review & Editing.
A.A. Methodology, Investigation, Writing-review & Editing.
T.K. Methodology, Investigation, Writing-review & Editing.
N.A. Methodology, Investigation, Writing-review & Editing.
S.B. Investigation, Methodology, Validation Original Draft, Writing-review & Editing.
M.A. Investigation, Methodology, Validation Original Draft, Writing-review & Editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author on reasonable request.
Informed Consent
Written informed consent was obtained before completing the questionnaire, participants were informed that participation in the study is voluntary, and confidentiality and anonymity of the information was confirmed.
Consent for Publication
All authors have reviewed and approved the final version for publication and agree on the content.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.