
Abstract
Introduction
Occupational stress affects health professionals; however, no literature was found on the middle-range theory for this outcome in health professionals.
Methods
Methodological study for the theoretical validation of a nursing diagnosis using the theoretical framework of Walker and Avant and the Betty Neuman systems models. The research was conducted in five stages: comprehension of the system model; selection and review of studies; development of the conceptual–theoretical–empirical structure; elaboration of a diagram and proposition of a nursing diagnosis; and evaluation of the empirical adequacy of the theory and validity of the system model. These steps were conducted using a scoping review and a sample of 138 articles selected in the Scopus, Web of Science, MEDLINE/PubMed, CINAHL, PsycINFO, LILACS, Science Direct, Cochrane Library, and Google Scholar databases. A data extraction instrument was developed, and study variables (attributes, antecedents, and clinical consequences) were analyzed using descriptive statistics (absolute and relative frequencies) and presented in tables.
Results
The middle-range theory comprised 16 concepts, 20 propositions, and one diagram. A total of 15 related factors, 29 defining characteristics, six at-risk populations, and one associated condition were indicated to propose the nursing diagnosis for occupational stress.
Conclusion
The middle-range theory supported elaborating elements to propose a nursing diagnosis for occupational stress.
Introduction
Nursing diagnoses are guiding tools for the work process in nursing. In this context, the NANDA International encourages reviewing and developing nursing diagnoses to improve its knowledge and allow researchers from different countries to expand the taxonomy (Herdman et al., 2021).
The middle-range theory (MRT) allows for developing diagnoses and expanding nursing knowledge (Fernandes et al., 2022). Also, an MRT addresses specific concepts for nursing care (Leandro et al., 2020; Lemos et al., 2020). Lopes et al. (2015) reinforced the need for developing strategies based on MRT to reduce gaps between theory and practice. Similarly, Lopes and Silva (2016) recommended developing nursing diagnoses based on MRT since it reinforces relationships among the concepts of elements.
Several nursing theories were developed, such as the Betty Neuman systems model, which can generate the MRT using a deductive method. In this model, the person (i.e., client) has constant reciprocal interaction with the environment and stressors that may cause instability in the system and reactions to stress (e.g., sickness). Thus, the nurse performs essential interventions to stabilize the system of the client (Neuman & Fawcett, 2011). The Betty Neuman systems model can be applied in several areas of nursing (e.g., occupational and mental health and infectious diseases), including in patients with COVID-19 and health professionals (Almino et al., 2021; Costa et al., 2020; Joshi et al., 2020; Oliveira et al., 2018; Pinto et al., 2020).
Occupational stress in health professionals (OSHP) is an acute or chronic response of the individual, who presents fatigue, irritability, emotional exhaustion, and tension (Mojtahedzadeh et al., 2021; Sahin et al., 2020), which may lead to complications, such as Burnout syndrome, depression, and reduced quality of life (Abdelhafiz et al., 2020). Although healthcare requires complex, often immediate, and unpredictable decision-making, several health professionals still work under inadequate conditions (Costa et al., 2020; Hoseinabadi et al., 2020; Liu & Aungsuroch, 2019). Occupational stress is prevalent among health professionals from the surgery and intensive care unit sectors (Arunmozhi et al., 2018; Baye et al., 2020; Munhoz et al., 2020; Shen et al., 2020).
A study conducted among health care professionals in Turkey to examine increased levels of anxiety and occupational stress during the pandemic found that health care professionals working in intensive care and emergency services had higher rates of emotional exhaustion and lower rates of personal accomplishment compared with professionals working in laboratory, radiology, and outpatient settings (Sahin et al., 2020).
Occupational stress is common in all professions but more prevalent in groups with high sources of job pressure (Costa et al., 2020; Hoseinabadi et al., 2020; Liu & Aungsuroch, 2019). A multicenter study found that 82% of healthcare professionals reported moderate levels of stress (Aldarmasi & Alghamdi, 2021). Research showed a 77% prevalence of occupational stress among nursing professionals (Novaes Neto et al., 2020). Nursing is among the occupations that may develop this phenomenon since professionals are directly responsible for patient care and organization of the hospital sector, apart from excessive administrative, bureaucratic, repetitive tasks (sometimes under inadequate working conditions), and unhealthy environments (Abdelhafiz et al., 2020). In addition, these professionals are frequently exposed to tension and illness within the hospital (Appel et al., 2021).
In this sense, the physical, psychological, social, and cultural damage caused by occupational stress may impact the daily routine of nursing professionals and generate several consequences for the individual, the family, the company where the professional works, and the community (Santana et al., 2020). These professionals also need to intervene in occupational stress to enhance the mental health of healthcare professionals and reduce complications (e.g., mental disorders). Nevertheless, nursing lacks a standardized language complying with the nursing theory to describe problems related to occupational health. Also, the NANDA International presents no nursing diagnosis for occupational stress (Herdman et al., 2021). Therefore, developing such tools may guide nurses in clinical practice, prioritize nursing interventions, and improve the health of these professionals.
Therefore, this study aimed to develop a MRT of OSHP (MRT-OSHP) based on the Betty Neuman systems model to propose a nursing diagnosis for occupational stress.
Methods
Design
This methodological study was based on a valid causal theory. The MRT was developed based on a concept analysis from the theoretical framework by Walker and Avant (2019) and a scoping review derived from Betty Neuman systems model (Neuman & Fawcett, 2011). The concepts of MRT were divided into five steps according to the theoretical framework by Fawcett and Gigliotti (2001): (1) comprehension of the Betty Neuman systems model; (2) literature review of studies based on the Betty Neuman systems model; (3) development of the conceptual–theoretical–empirical structure (C–T–E); (4) disclosure of the C–T-E structure from a narrative and diagram; and (5) evaluation of the empirical adequacy of the MRT and validity of the Betty Neuman systems model.
According to the second step proposed by Fawcett and Gigliotti (2001), a literature review was also performed to identify and classify studies based on the Betty Neuman systems model on occupational, mental health, or both. The search was conducted on Scopus, Web of Science, MEDLINE/PubMed, CINAHL, and LILACS using the keywords ‘nursing theory’ AND ‘Neuman’. Eighteen studies using the Betty Neuman systems model were included.
Inclusion criteria comprised articles published without time and language restriction that addressed the Betty Neuman systems model on occupational, mental health, or both. Exclusion criteria comprised letters to the editor, interviews, and abstracts.
Subsequently, a concept analysis was performed through a scoping review to identify the antecedents, attributes, and clinical consequences of OSHP. The scoping review also identified propositions of the MRT-OSHP, related factors, defining characteristics, at-risk populations, and associated conditions of the proposition for the nursing diagnosis. Thus, this scoping review supported the third and fourth steps for the MRT derived from the Betty Neuman systems model.
The scoping review was based on the Joanna Briggs Institute (JBI), registered on the Open Science Framework, and guided by the PRISMA Extension for Scoping Reviews (PRISMA-ScR) (Peters et al., 2020).
The following databases were used for literature search: Cochrane Library, Scopus, Web of Science, National Library of Medicine (MEDLINE/PubMed), Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, Latin American and Caribbean Literature in Science of Health (LILACS), ScienceDirect, and Google Scholar.
Research Question
The research question was developed using the Population, Concept, and Context (PCC) mnemonic. Thus, P was defined as health professionals; C was OSHP; and C was health services. The following questions were established: “which attributes determine the OSHP?”; “which are the antecedents and clinical consequences of OSHP?”; “which are the protection and prevention factors of the OSHP?”.
Inclusion and Exclusion Criteria
The inclusion criteria comprised articles published without time or language restrictions that addressed any group of health professionals working in health services. Publications not responding to the research questions, duplicates, abstracts, letters to the editor, or editorials were excluded.
The following Medical Subject Headings (MeSH) were used with Boolean operators ‘AND’ and ‘OR’: occupational stress, burnout, professional, health personnel, nurses, dentistry, physiotherapists, occupational therapists, physicians, speech therapy, risk factors, signs and symptoms, and health services. These descriptors were also related terms from the following Health Sciences Descriptors (DeCS): occupational stress, health personnel, symptoms, and health services.
The following combination of terms was used: (1) Occupational stress OR Burnout and Professional AND Health personnel OR Nurses OR Dentistry OR Physioterapists OR Occupational Therapists OR Physicians OR Speech Therapy AND Health Services; (2) Occupational stress OR Burnout and Professional AND Health personnel OR Nurses OR Dentistry OR Physioterapists OR Occupational Therapists OR Physicians OR Speech Therapy AND Risk Factors AND Health Services; and (3) Occupational stress OR Burnout, Professional AND Health personnel OR Nurses OR Dentistry OR Physiotherapists OR Occupational Therapists OR Physicians OR Speech Therapy AND Signs, and Symptoms AND Health Services.
Sample
Studies were selected based on a flowchart adapted from the PRISMA-ScR (Peters et al., 2020). The search was performed simultaneously and manually by four trained nurses to avoid biases in article selection (Figure 1).
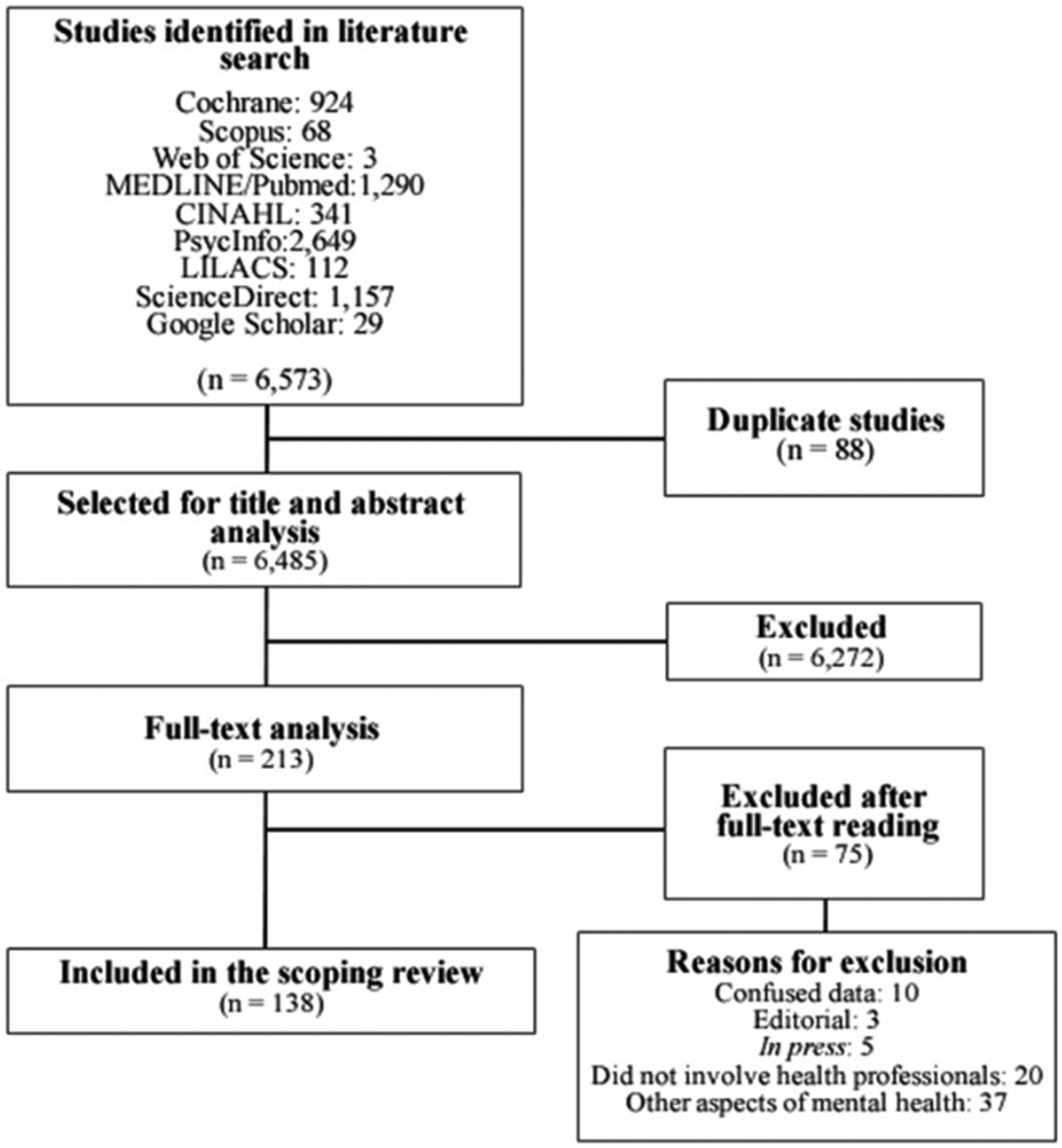
Flowchart of study search adapted from the PRISMA-Scr.
Initially, 6,573 articles were identified in the Cochrane (924), Scopus (68), Web of Science (3), MEDLINE/PubMed (1,290), CINAHL (341), PsycINFO (2,649), LILACS (112), ScienceDirect (1,157), and Google Scholar (29) databases; 88 duplicates were excluded.
A total of 6,485 were selected for title and abstract analysis, and 213 studies were selected for full-text analysis. However, 138 composed the final sample.
Instruments
An instrument was developed for data extraction considering the following information: article title, year of publication, journal, study design, country of study, data source, objective, attributes, antecedents and consequences, causal relations, protective factors, and intervention strategies to prevent OSHP.
Statistical Analysis
Variables were analyzed using descriptive statistics (i.e., absolute and relative frequencies), and a table was created with attributes, antecedents, and clinical consequences. A diagram of the MRT and a chart of the proposed nursing diagnosis were also developed.
Results
Sample Characteristics
A final sample of 138 studies was selected for the scoping review; most were cross-sectional and quantitative studies conducted with nursing or health professionals and published within the last 10 years in the MEDLINE/PubMed database. The Asian and European continents contributed mostly to research involving OSHP.
Research Question Results
The MRT-OSHP was developed according to the scoping review and Betty Neuman systems model (Neuman & Fawcett, 2011).
Comprehension of the Betty Neuman Systems Model
The Betty Neuman systems model is based on stress, reaction to stressors, and interventions for stress prevention (Neuman & Fawcett, 2011). The following main concepts were observed: client system (i.e., individual, community, family, or social); interaction variables (i.e., physiological, psychological, sociocultural, developmental, and spiritual); stressors (intra-, inter, and extrapersonal); basic structure or central core; flexible, normal, and resistance line of defense; internal, external, and created environment; stability of client system; well-being variations; reconstitution; and prevention as intervention (primary, secondary, and tertiary) (Neuman & Fawcett, 2011).
Literature Review of Studies Based on the Betty Neuman Systems Model
Most studies addressing the Betty Neuman systems model were qualitative (38.8%/n = 7) and published in the last eight years (61.1%/n = 11). Brazil (44.4%/n = 8) and the United States (38.8%/n = 7) were the countries that most published studies on this model.
Publications addressed the Betty Neuman systems model mainly in the mental health field (61.1%/n = 11), stress (55.5%/n = 10), and professionals (38.8%/n = 7). Most studies (50%/n = 9) only described the concepts of the Betty Neuman systems model.
Development of the C–T–E Structure
Attributes, antecedents (i.e., stressors), clinical consequences (i.e., symptoms), and propositions for OSHP were listed to construct the C
Two attributes, 21 antecedents, and 29 clinical consequences for the concept of OSHP were observed. Three antecedents were classified as intrapersonal, three as interpersonal, and fifteen as extrapersonal stressors. Also, eight clinical consequences were classified as physiological and 20 as psychological symptoms. Table 1 highlights the most prevalent clinical antecedents, attributes, and consequences.
Synthesis of the Most Prevalent Attributes, Antecedents, and Clinical Consequences of Occupational Stress in Health Professionals.

The following concepts were adapted from the model: client system; intra-, inter-, and extrapersonal stressors; client system instability; illness; reactions; interaction variables; client system stability; wellness/health; nursing; and primary, secondary, and tertiary prevention.
The MRT had a holistic philosophical approach focused on OSHP. It also presented a multicultural and inter-, multi-, or transdisciplinary perspective based on occupational stress and interventions for prevention.
The following concepts were defined for the MRT-OSHP: health
In MRT-OSHP, occupational stress had a perspective of negative human response but not disease. The propositions of the MRT-OSHP (highlighting the nursing metaparadigm) are detailed below:
The client is a healthcare professional; Intra-, inter-, and extrapersonal stressors may influence the health The conflict between identity and role, having more than one job, and low professional experience are intrapersonal stressors for OSHP; Inefficient network of social support, imbalance among work, family, and leisure, and conflicting interpersonal relationships are interpersonal stressors for OSHP; The work environment is related to extrapersonal stressors for OSHP; Care for critical patients, excessive workload and working hours, ineffective communication and management, difficulty in decision-making, inadequate staffing, traumatic professional experience, exposure to biological agents, professional disability and devaluation, precarious working conditions, long commuting time to work, alternate or night shift work, and professional experience in pandemics, epidemics, or infectious outbreaks are extrapersonal stressors for OSHP; Adoption of healthy living practices, preserved physical health, spiritual well-being, life skills (cognitive, emotional, and social), social support, personal and professional fulfillment, adequate working conditions and processes, and well-being and quality policies at work are protective factors for the health professional to respond to intra-, inter-, and extrapersonal stressors and present stability in the health–disease process (i.e., preserved mental health); Health professionals with negative responses to intra-, inter-, and extrapersonal stressors may present physiological symptoms (e.g., cardiovascular, dermatological, gastrointestinal, immunological, musculoskeletal, and appetite changes, headache, and insomnia); Health professionals with negative responses to intra-, inter-, and extrapersonal stressors may present psychological symptoms (e.g., impaired concentration, anxiety, apathy, low situational self-esteem, recurrent crying, impaired quality of life at work, fault, desire to change sectors, lack of work motivation, difficulty in performing work activities, work-related frustration, suicidal ideation, job dissatisfaction, insensitivity to patients, irritability, nervousness, fear, anger, depressive symptoms, sadness, and use of psychoactive substances); The instability of the health–disease process of the health professional is an OSHP, which is evidenced by emotional exhaustion or work-related fatigue; The nurse promotes stability in the health–disease process of the health professional; The nurse identifies intra-, inter-, and extrapersonal stressors to promote mental health and prevent occupational stress; The nurse acts at the primary, secondary, and tertiary levels to promote mental health and prevent occupational stress in health professionals; Nursing interventions can be performed directly by the nursing team or indirectly when the nurse articulates interventions with a multidisciplinary team. The health professional should actively participate in the planning and evaluation of interventions; Interventions of primary prevention aim to promote mental health in health professionals by identifying and minimizing the negative impacts of intra-, inter-, and extrapersonal stressors; Primary prevention for OSHP includes the following interventions: stimulate life skills, healthy practices and adequate working hours, effective leadership and communication, healthy relationships and conflict resolution, shared decision-making, and participation of professionals in commissions and working groups; provide social support, training, programs for well-being and quality of life at work, professional development with adequate workload and remuneration, supply of materials, daycare, accommodation, transport, and staff admission; adequate working conditions and process, institutional policy for health professionals, and measures to control and prevent infections at work; opportunities to shift activities; and guide patients and companions on rights and duties; Interventions of secondary prevention aim to early detect OSHP and treat the physiological and psychological symptoms; Secondary prevention for OSHP includes the following interventions: nursing consultation to detect early symptoms of OSHP, planning the treatment with the multidisciplinary team, and providing a group of support for counseling; Interventions for tertiary prevention aim to readapt and maintain the stability of the health–disease process; Tertiary prevention for OSHP includes the following interventions: nursing consultation for follow-up and evaluation of return to work, planning the support from coworkers, guiding managers, and offering art and music therapy and other integrative and complementary practices.
Disclosure of the C–T–E Structure From a Narrative and Diagram
According to the MRT-OSHP diagram (Figure 2), health professionals have protective factors to maintain the stability of the health–disease process and mental health when exposed to intra-, inter-, and extrapersonal stressors in internal and external work environments. However, health professionals may develop psychological or physiological symptoms, instability of the health–disease process, and occupational stress when they present negative responses to stressors. Thus, nursing is essential in this health–disease process to implement interventions for improving the mental health of health professionals and promoting secondary or tertiary prevention of occupational stress.

Diagram of the middle-range theory of occupational stress in health professionals (MRT-OSHP).
Evaluation of the Empirical Suitability of the MRT and Validity of the Betty Neuman Systems Model
This step must occur by evaluating the validity of the MRT-OSHP. Future research with quantitative, qualitative, or mixed designs is recommended to test the MRT-OSHP.
Proposition of the Nursing Diagnosis of Occupational Stress
The nursing diagnosis of occupational stress was based on the MRT-OSHP and proposed to be included in the NANDA International. Table 2 shows the structure of the proposed diagnosis.
Proposition of a Nursing Diagnosis for Occupational Stress.

The concept of the proposed diagnosis was defined, and 29 defining characteristics, 15 related factors, six at risk populations, and one associated condition were listed. The diagnosis should be included in domain nine (coping/stress tolerance) and class two (coping responses) of the NANDA International.
Discussion
The MRT-OSHP based on the Betty Neuman systems model supported the development of essential terms to characterize the studied occupational stress.
Most literature using the Betty Neuman systems model only described the concepts of the model and addressed stress in professionals (Almino et al., 2021; Pinto et al., 2020). In this sense, this study corroborated the importance of developing an MRT based on this model to improve concepts for clinical practice and reinforce the relevance of the studied topic.
The main associated factors (i.e., antecedents) and at-risk populations were excessive workload and working hours; professional experience in pandemics, epidemics, or infectious outbreaks; care for critical patients; and inadequate staffing. Thus, a relationship was observed between stress and excessive workload. In a cross-sectional study regarding occupational stress in different professionals, stress levels were high in nurses, mainly due to workload and the need for quick responses (Zare et al., 2021).
Several studies addressed the relationships between OSHP and professional experience during the COVID-19 pandemic. These studies described the following factors influencing stress levels in health professionals: SARS-CoV-2 infection, fear of developing the disease, illness of health professionals leading to work overload and exhausting working hours, insufficient staffing, precarious working conditions due to lack of supplies, and limited access to personal protective equipment (Abdelhafiz et al., 2020; Aldarmasi & Alghamdi, 2021; Ilczak et al., 2021; Lasalvia et al., 2021; Zare et al., 2021). Also, studies demonstrated relationships between occupational stress and health professionals who care for critical patients since they require greater caution in decision-making (Abdelhafiz et al., 2020; Wijn & Doef, 2020).
Regarding the defining characteristics (i.e., clinical consequences), anxiety, compromised quality of life at work, depressive symptoms, job dissatisfaction, and insomnia were the most relevant symptoms of occupational stress. In a Jordanian mixed study investigating occupational stress and job satisfaction during the COVID-19 pandemic, most professionals reported fear and anxiety related to clinical practice influencing emotional exhaustion (Alrawashdeh et al., 2021).
Occupational stress may decrease the quality of life of health professionals and increase demands, compromising professional and personal performance. Besides the relationship between impaired quality of life at work and occupational stress (Chen et al., 2019; Khatatbeh et al., 2022; Moukarzel et al., 2019), studies showed a direct association between occupational stress and depression, in which precarious working conditions and exhausted workforce due to the pandemic influenced the mental health of health professionals (Baptista et al., 2021; Denning et al., 2021).
Sleep disorders (e.g., insomnia and nightmares) were associated with OSHP. Night workers may be constantly alert and awake, changing their biological rhythm. Furthermore, other stressors may impact the sleep patterns of these professionals (Durand et al., 2019; Moukarzel et al., 2019; Peter et al., 2020; Zhao et al., 2020).
Job dissatisfaction is also associated with OSHP and may be influenced by stressors (e.g., excessive workload and conflicting interpersonal relationships) (Friganović & Selič, 2021; Peter et al., 2020; Tung et al., 2020). Thus, causal relationships between occupational stress and stressors and symptoms are complex, and nurses must be cautious about interventions implemented in clinical practice and the care of health professionals. In this sense, recognizing the protective factors of occupational stress is essential to increase the quality of care.
Most studies highlighted the importance of implementing institutional policies on health, well-being, and quality of life at work. The involvement of professionals in developing guidelines and policies should be encouraged at an organizational level (Baptista et al., 2021). Thus, organizational and political systems are essential to maintaining a healthy work environment and conditions (Jiang et al., 2021; Khatatbeh et al., 2022).
Social support benefited the stability of the health–disease process of health professionals, especially from colleagues, managers, and family (Wu et al., 2020). Also, adequate working conditions and processes were protective factors against occupational stress. In this sense, social and labor rights support may also ensure a healthy work environment (Novaes Neto et al., 2020; Wijn & Doef, 2020).
Studies emphasized the importance of developing life skills (cognitive, emotional, and social) as protective factors against occupational stress. Performance is high in health professionals well qualified to meet demands, creative, communicative, and with problem-solving skills at work; thus, institutions must encourage these skills (Araújo et al., 2020; Novaes Neto et al., 2020). Literature also indicated personal and professional fulfillment (e.g., satisfaction and recognition) as protective factors for professionals (Guissi et al., 2019; Scanlan & Still, 2019).
Although occupational stress has been addressed in several studies, it needs further investigation, especially occupational health. Nurses, for example, need to understand and intervene using specific methodological strategies from nursing topics (e.g., processes, diagnoses, and theories) since occupational stress is increasingly present among health professionals. In this context, the MRT-OSHP may help nurses identify the health stressors and protective factors in health professionals for (1) developing individual or collective interventions, (2) treating mental health, and (3) preventing occupational stress at primary, secondary, or tertiary levels. Moreover, these interventions can be implemented by the multidisciplinary team, managers, and health professionals, who should establish priority interventions. Nurses working with occupational health can also be supported by evidence-based practice (MRT-OSHP) and apply this model tin several nursing fields (e.g., assistance, research, teaching, and management).
The main concepts and propositions identified during the development of the MRT-OSHP enabled the explanation of this phenomenon in nursing professionals. Also, several less abstract and more specific concepts related to the nursing practice and OSHP were presented. Thus, this study provides clear and robust knowledge for nursing actions to identify and propose strategies, prevent occupational stress, and promote satisfaction, well-being, and quality of life at work. Moreover, the proposed theory may reduce the gap between nursing theory and practice and can be an alternative to other movements, such as evidence-based practice and translational research
The study was innovative for the theoretical advance of nursing focused on the mental health of professionals. As a limitation, the MRT-OSHP was focused only on health professionals; thus, the theory should be interpreted with caution in other populations.
Implication for Nursing Practice
This study supports effective and robust nursing care by identifying the needs of health professionals and establishing priorities for nursing interventions to promote mental health and prevent occupational stress. Nevertheless, future research must evaluate the use of the MRT-OSHP and its theoretical content in nursing care.
Conclusion
The study allowed the development of the MRT-OSHP, which addresses that health professionals have protective factors to maintain the stability of the health–disease process and mental health when exposed to intra-, inter-, and extrapersonal stressors in internal and external work environments. However, health professionals may develop psychological or physiological symptoms, instability of the health–disease process, and occupational stress when they present negative responses to stressors. Thus, nursing is essential in this health–disease process to implement interventions for improving the mental health of health professionals and promoting secondary or tertiary prevention of occupational stress.
The MRT-OSHP was based on the Betty Neuman systems model and supported by the proposition of the nursing diagnosis for occupational stress. Among the 29 defining characteristics, the most prevalent were anxiety, impaired quality of life at work, depressive symptoms, dissatisfaction at work, and insomnia. Also, the most prevalent associated factors and at-risk populations were excessive workload and working hours; professional experience in pandemic, epidemic, or infectious outbreaks; care for critical patients; and inadequate staffing. Psychiatric disorder was the only associated condition.
A total of 16 concepts, 20 propositions, and one diagram were developed for the MRT-OSHP. Thus, the MRT-OSHP and proposition of the nursing diagnosis may help clarify the occupational stress in this population.
Footnotes
Acknowledgments
The authors thank the Brazilian Hospital Services Company for their contribution to this research and Probatus Academic Services for providing scientific language translation, revision, and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.