
Abstract
Background
Violence during pregnancy, childbirth and after childbirth is a critical issue globally. There remains a lack of consensus on operational definitions of the components across different cultures globally since the definitions of respect, disrespect and violence can differ among cultures, traditions and places. Obstetric violence presents a significant barrier to seeking facility-based care during pregnancy and childbirth and instead women may opt for home deliveries with unskilled attendants. As a result, some experience complications thus contributing to the high prevalence of maternal mortality and morbidity.
Objective
To explore the contextual components of obstetric violence as perceived by postnatal mothers, health care providers and key community informants in central zone Tanzania.
Methodology
An exploratory qualitative case study employed in-depth interviews with purposefully selected 24 postnatal mothers, 18 healthcare providers, and 4 religious leaders. Additionally, 6 focus group discussions were conducted with male partners, community health workers, and 10-cell leaders. Data analysis followed qualitative content analysis process, incorporating both inductive and deductive approaches.
Results
Nine categories of obstetric violence experienced by women during health facility care emerged from the analysis. These categories are lack of supportive care and treatment, autonomy limitations, non-consented care, compromised privacy and confidentiality, painful routine procedures that are not evidence-based, verbal violence, sexual violence, stigma and discrimination, emotional violence. Additionally, six categories of obstetric violence emerged related to experiences of women at the community level. They included: forceful insertion of herbs to the vagina, verbal violence, physical violence, psychological violence, forced home delivery and inappropriate sexual practices.
Conclusion
Contextual components gathered by this study help to better define obstetric violence in the Tanzanian context and serve as a reference. This might help to validate measurement methods, and provide a pathway for developing evidence-based interventions to reduce obstetric violence and promote respectful maternity care.
Background
The World Health Organization (WHO) defines obstetric violence (OV) as the control over a woman's body and reproductive processes through dehumanizing treatment that in turn negatively impacts her quality of life (World Health Organization, 2015). Obstetric violence occurs when a woman is forced into procedures without consent such as during vaginal exams, cesarean section delivery, sexual comments or sexual assault, spoken disrespectfully words, non-confidential care, detention in facilities due to failure to pay user fees, physical abuse or non-consented care (Bowser & Hill, 2010; Cristiano et al., 2021; Lamaze, 2013; Miguel et al., 2021; Sando et al., 2016). The prevalence of obstetric violence during pregnancy and delivery ranges from 15% to 99% (Hirut et al., 2022), 44% to 51.5 in Sub-Saharan Africa (Kassa et al., 2020; Sanga & Joho, 2023). Obstetric violence contributes to high maternal mortality and morbidity (Bohren et al., 2014). This is because the experience of obstetric violence may hinder women from seeking health care services in the health facilities for adequate management of maternal and neonatal complications and end up opting for home deliveries with unskilled attendants (Kassa et al., 2020; Sanga & Joho, 2023).
In 2015, the WHO emphasized the right of every woman to attain high standard of health, including the right to dignified and respectful care (World Health Organization, 2015). Scholars worldwide are actively investigating the definition, underlying causes and methods of assessing obstetric violence during pregnancy and childbirth. Despite extensive studies, there remains a lack of universal agreement on its operational definitions of its components, driving factors and measurement methods attributed to variations influenced by geographical and cultural factors (Ministry of Health, Community Development, Gender, 2019; Savage & Castro, 2017). Designing policies and bolstering systems that offer respectful care requires an understanding of the contextual perspectives on violence, disrespect, and respect (Downe, 2019). Local context plays a key role in defining and understanding obstetric violence as the meaning of respect, disrespect and violence may vary across cultures, traditions, and geographical locations (Kaveri et al., 2022). Without recognizing local manifestations and understandings, there is a risk of underreporting or overreporting, which leads to a lack of awareness among policymakers and healthcare providers and hinders efforts to address these issues effectively.
In Tanzania, as in other nations, the available contents in the existing guidelines are largely informed by evidence from other contexts that may be different from Tanzania. Consequently, certain aspects of obstetric violence as understood by Tanzanians might be overlooked or misrepresented (McMahon et al., 2014).
Therefore developing an evidence-based typology of obstetric violence is a critical step to inform the development of measurement tools and support the development and evaluation of context specific interventions to reduce obstetric violence and promote respectful maternity care (Bohren et al., 2016). To that end, this study sought at exploring context specific component of obstetric violence in Central zone, Tanzania.
Review of Literature
Globally, evidence of obstetric violence is reported and research shows that almost every woman goes through some level of violence during childbirth (Kaveri et al., 2022). Researchers from across the world continue to explore the meaning, driving factors, and measurement of obstetric violence during pregnancy and childbirth as to date there is no consensus at a global level on how it is defined and measured (Vogel et al., 2015). The most common forms of obstetric violence reported in different studies include physical abuse (54.5%), verbal abuse (58%), abandonment (36.8%), non-dignified care (6%), and 55.5% non-consented care (Cristiano et al., 2021; Miguel et al., 2021; Sanga & Joho, 2023) . Obstetric violence is so normalized that it is not (yet) considered violence against women in most settings. In some settings, women are told that everything is alright and all that what is important is that the baby is alive (Cheryl et al., 2014). Understanding of “obstetric violence” involves our ability to challenge “normal” obstetric care practices. It is highly dependent on how we understand “violence” and our collective ability to recognize obstetric violence in a particular context may be influenced by cultural and geographical differences. These can vary from one country to the next and the violence can manifest differently between women with different socio-demographic characteristics (Bowser & Hill, 2010; Pickles, 2021).
Objective
This study aimed at exploring the context specific components of obstetric violence as understood by postnatal women, health care providers, and key community informants in Central Zone Tanzania.
Methods
Study Design
An exploratory case study was conducted in Central Zone Tanzania between July and December, 2023. This design is considered appropriate to describe components of obstetric violence as it enables researchers to obtain multiple perspectives, explore the meanings people attach to the phenomenon of interest and take into account contextual complexity (Creswell, 2018; Robert, 2023). The COREQ guidelines were followed.
Study Setting and Selection
The study was conducted in the regions of Dodoma and Singida which are located in the central part of Tanzania. These regions were purposefully selected because of their high maternal mortality rate. The mortality rate in Dodoma is 417 and Singida 468 per 100,000 live births (Nassoro et al., 2020; National Bureau of Statistics Ministry of Finance Dar es Salaam et al., 2015). In these regions, women commonly give birth at homes as they hesitate to seek care at a birthing facility due to individual and community experiences of obstetric violence (Das et al., 2021; Eidgenossenschaft & Svizzera, 2019; Muhunzi et al., 2020).
Study Participants and Sampling Procedures
While childbirth experiences are long recalled, sometimes for decades or years (Simkin, 1992), the accuracy of recall for some clinical details and perceptions may decline over time. To mitigate the possibility of recall bias when reporting such details, 24 postnatal mothers who had given birth within the past 6 to 12 months were purposively recruited, in accordance with inclusion criteria established in other studies (Coughlin, 1990; Garthus-Niegel et al., 2014; Waldenström, 2003). This period was chosen to optimize recall accuracy and allow adequate emotional and experiential reflection. Assistance from 10-cell leaders and community health workers facilitated the identification of these households and postnatal mothers within their respective catchment areas but they were not involved in interviewing processes, rather two trained research assistants unaffiliated with that particular area carried out the interviews. Furthermore, members of the community were purposively selected in the two administrative wards based on their roles and influence in the community and served as key informants in this study. These included 10-cell leaders (local grassroots leaders), religious leaders (influential in shaping beliefs), community health workers (who link communities with health care services), and male partners (key decision-makers within households). These key informants were also individuals who had lived in that particular administrative ward for more than one year and were Tanzanian by origin. In addition, three traditional birth attendants (TBAs) were included as key informants and were recruited by snowball sampling technique. Purposive sampling was utilized to recruit 18 healthcare providers, selected based on their professional cadre and experiences. Among them, 14 were midwives and 4 were obstetricians. The majority had over 10 years of work experience in maternity units. Figure 1 below describes how the sampling process was conducted (Pritha, 2022). The sampling process was carried out based on the principle of data saturation, whereby interviews continued until no new information was provided by the participants. This was an indication that any further collection of data was not likely to yield more new information (Saunders et al., 2018).
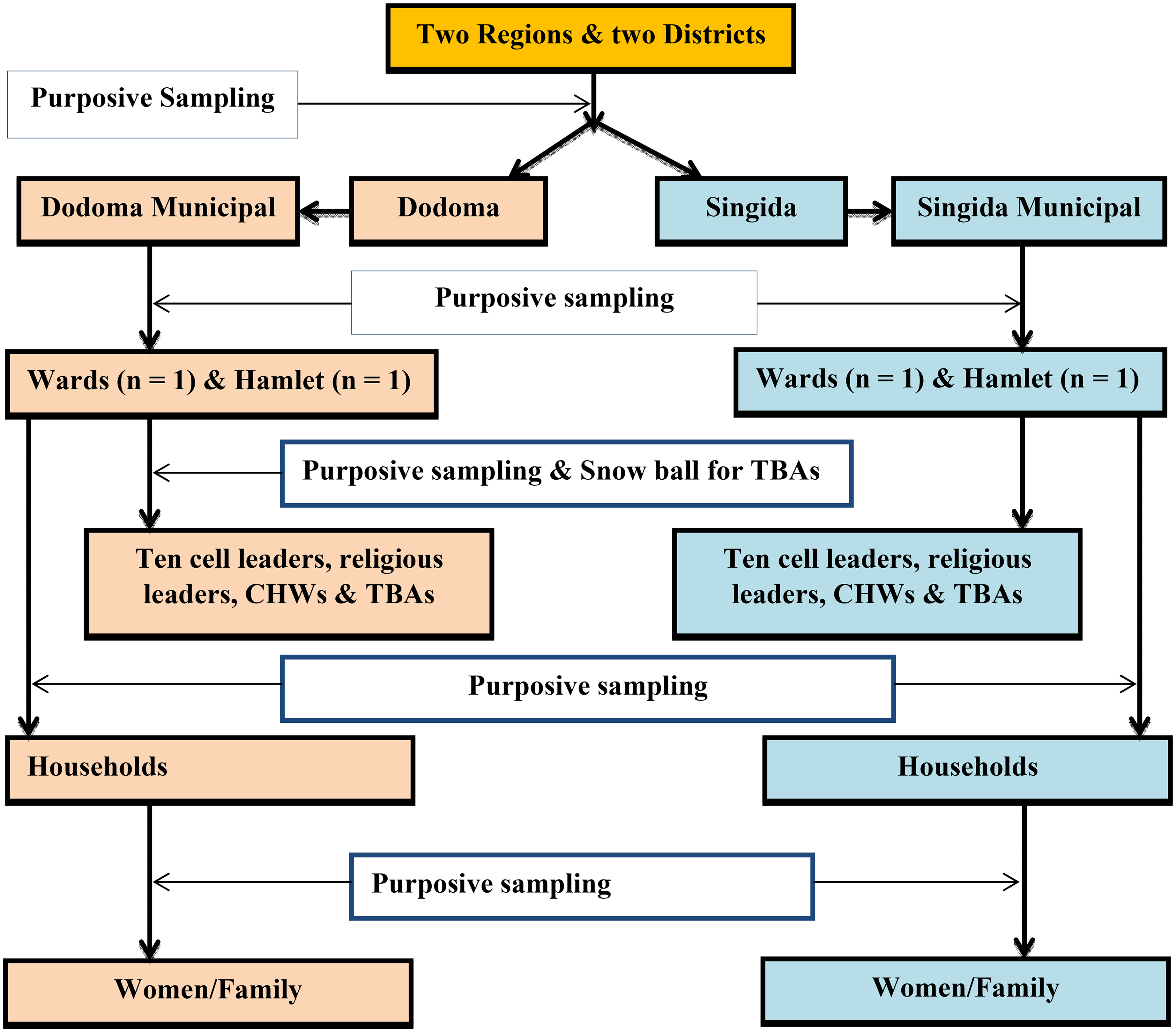
Multi-stage sampling flow chart.
Data Collection
The Kiswahili interview guides were used to conduct in-depth interviews (IDIs) and focus group discussions (FGD). Twenty-four IDIs were conducted with postnatal mothers and four were conducted with religious leaders. In addition, six FGDs with key informants (10-cell leaders, religious leaders, and community health workers) were conducted. Additionally, 18 key informant interviews with health care providers were conducted, as shown in Table 1.
Summary of the Study Participants for IDI, KII, and FGD.

The interviews were conducted by two trained research assistants who had prior experience in interviewing participants and conducting qualitative research. The audio portion of the IDIs, key informant interviews (KIIs) and FGDs were recorded using a digital voice recorder. The IDI and KIIs lasted between 30 and 50 minutes while the FGDs lasted between 60 and 90 minutes. Interviews were conducted in various locations chosen by the participants. These included participants’ homes, offices, and private rooms at health facilities. Each FGD consisted of 7 to 10 individuals and took place either at village executive offices or in a participant's home as coordinated by the 10-cell leaders. Socio-demographic information such as age and education level as well as obstetric characteristics like parity and gravidity, were collected initially and documented in the information sheet. This was followed by open-ended questions and probes concerning perspectives on obstetric violence, their birth experience, contributing factors and recommendations for improving. In order to ensure exploration of comprehensive information about obstetric violence perspectives, the interview guide (attached as supplement file) was kept flexible and was modified during the data collection process. Participants provided consent for participation before the interview.
Data Analysis
Qualitative content data analysis was employed in the analysis process (Graneheim & Lundman, 2004). All IDIs, KIIs, and FGDs were audio recorded and subsequently transcribed verbatim. The Kiswahili transcripts were analyzed to preserve the authenticity of the gathered data. Researchers ensured comprehensive familiarity with the data through repeated readings of the complete transcripts and field notes. A hybrid approach combining both inductive and deductive methods was utilized. Initially, a deductive approach was used to develop a preliminary codebook based on the study's objectives and the researchers’ familiarity with the data. Following this, an inductive approach was employed to incorporate new codes that emerged during the data analysis. The codebook was reviewed and refined through discussions among all authors until consensus was achieved. Meaning units related to participants’ perspectives were identified through data reduction and codes were generated from these condensed units. NVIVO software version 12 was used to manage and organize the data. The initial codes were reviewed and agreed upon by the authors. Similar codes were grouped and organized into sub-categories through comparison. After reflecting on the similarities and differences between sub-categories and considering the participants’ perspectives, the authors reached an agreement on the main categories. Selected quotes were used to illustrate the categories and sub-categories. Finally, the codes and quotes were translated from Kiswahili to English by an independent translator and the research team verified that the meaning remained consistent. The whole process of analysis was iterative (Id & Simba, 2021; Mwakawanga et al., 2022).
Results
Obstetric violence at health facilities
Physical violence
Obstetric Violence at Health Facilities.

Obstetric Violence at the Community Level.

“I might share instances of harmful actions based on my own experience. When I was about to give birth, the healthcare providers pinched my shoulder with forceps, telling me to push. Then, they slapped my thighs, and one nurse strapped my legs to the delivery bed. Another doctor, who was nearby, covered my mouth while I was screaming from the pain. I prefer not to remember those moments.”
“Giving episiotomy without anesthesia like lignocaine is also a violence, and many women do complain of this act. And the other thing that women complain much is the fundal pressure.”
Lack of supportive care and treatment:
“I was once denied services at the antenatal clinic because I didn't have a partner with me. Since my husband wasn’t around, I decided to bring my brother-in-law.” “This happened to my wife once. I took her to the health facility for further care after she had delivered at home. When we arrived, the nurses just stared at us.One of them said, ‘Why didn’t you finish everything there if you were able to deliver at home? You’re just disturbing us.”
Lack of autonomy
“I remember when my sister was about to undergo surgery, she asked the nurses and doctors for a few minutes to pray, hoping that God might help her deliver naturally. The providers refused and said there was no time to wait.”
“For me, it's even better to deliver at home because the older women will take care of you, but in the hospital, they treat you like you're a child who doesn't know anything. It feels like a form of violence.”
“I remember when I was delivering my last child, they put you on medication, they stick needles in my buttocks as they want without clarification.”
Non-consented care
“At one point, I was eager to be informed about my labor progress. I spent an entire day in labor without receiving any updates, which I find concerning. In my opinion, it's essential for women in labor to be updated about their situation and progress."
“I can share my own experience. A nurse told me I needed a cesarean section because I had been in labor for a long time. I refused and was given a form to sign. Instead, I used Vaseline oil in the restroom to lubricate my rectum, and within an hour, I was able to push naturally. I believe many women are being rushed into surgery without proper evaluation.”
Lack of privacy and confidentiality
Two sub-categories emerged, including “Violence could also include inadequate privacy for women as sometimes you may find six beds lined up in a single room and no curtains to separate them.” “To me, discussing secret information and treatment in the presence of other people who are not supposed to here is not a good practice.”
Sexual violence
Participants mentioned acts such as inappropriate massaging of breast and inappropriate clitoris stimulation during per vagina examination to be bad practices. “It has once happened to me on my ANC visit. I was so scared to find the doctor's hand on my underpants massaging my external private parts and breast unusually during examination. I wanted to shout but the doctor apologized. I will never go to that health facility.”
Participants also reported the habit of some health care providers suturing the vaginal opening after delivery to narrow the opening based on a husband's request. “There is a practice where the vaginal opening is sutured after delivery to narrow the entrance, often at the husband's request for sexual pleasure. This is done secretly, and providers are paid to carry out the procedure. In most cases, women are unwilling. Additionally, some providers abuse their power to demand sex from pregnant women, claiming they are warm. I have witnessed this happen with a colleague in another place”
Stigma and discrimination
“Pregnant woman who are HIV positive can be violated and stigmatized during labor and delivery, I once heard a provider telling his colleague that be careful you have a family to feed.”
Verbal violence
“I passed a stool when I was in labor on the bed. The midwife who was helping shouted on me saying, I was dirty like a toilet. She spoke very harshly in a disrespectful manner and she was very young to me.”
Psychological /emotional violence
“Violence to me includes actions such as blaming a woman because of bad birth outcome such as losing a baby during delivery, being blamed of being unable to push the baby adequately.”
“Even denying a woman and her newborns discharge after childbirth because of not clearing the hospital bills to me is also a violence and brings emotional torture.”
Obstetric violence at community level
Traditional herbal practices “I have several times received women in labor with herbal medication inserted in their vaginal and some end up with complications like ruptured uterus. And most of the time if you ask them, they complain to be forced by elderly.” Sexual violence Participants described being told to have sex immediately after delivery so that if the husband goes out with other women will not harm the baby “There is ths tendency of male partners forcing their wives to have sex immediately after delivery so that if he goes out will not harm the baby to me this is violence. Physical violence “I started a labor pain at home, my mother started pulling the external genitalia to increase the labor pain, after that action the external parts were swollen and painful, is when I was taken to the hospital. I felt so ashamed on how the nurses were looking at me and communicated to each other.” “To my side obstetric violence from the community, could also include this practice of hot water massage after delivery, it makes women bleed more, should be stopped.” Psychological and emotional violence “Being neglected both at home and to the health facilities by husband and close relatives and lack their support because she did not deliver the wanted sex is also common here in our setting, this is also violence to me.” Forced home delivery “To me even forcing our wives to deliver at home, telling them you fear the hospital expenses is violence. Telling them our mothers and grandmother never go to hospital, is becoming common in our society.” “To me even forcing our wives to deliver at home, telling them our mothers and grandmother never go to hospital - I consider it as violence.” Verbal violence
“Some of the male partners use disgusting words and comments such as bitch, circumcised private parties, you do not look attractive any more especially when they did not want that pregnancy.”
Discussion
The current study aimed to describe perspectives of OV among postnatal mothers, key community informants and health care providers during pregnancy, childbirth and after childbirth. Contextualizing and typifying this phenomenon in different geographic and cultural contexts is crucial in better understanding and prevention obstetric violence. This study identified nine categories of OV connected to health facilities and six categories OV related to the community.
Several acts and practices were recognized as OV at the health facilities. These included nine key areas: physical violence, inadequate support, lack of autonomy; lack of privacy and confidentiality, sexual violence, verbal violence, stigma and discrimination, psychological and emotional violence. These results are consistent with recent data from a WHO-led study conducted in four countries: Ghana, Guinea, Myanmar, and Nigeria (Vogel et al., 2015; WHO, 2019) and some of the components also mirror those identified by Bowser and Hill (2010). The WHO-led study did not examine community-related OV, but the majority of health facility-related OV were similar, with a few notable exceptions such as the objectification and infantilization of women as identified in the current study.
Verbal violence was the most often described component of obstetric violence (OV), followed by physical violence. These patterns have also been found in other research to be the most prevalent during labor (Adu-Bonsaffoh et al., 2022; Okedo-Alex et al., 2021). On the other hand emotional violence, such as being detained in a health facility because one cannot pay the hospital costs, was frequently mentioned by our participants. This form of violence has been documented by few researchers (Bowser & Hill, 2010).
Health workers explained that women tend to be ungrateful and asserted that they would perceive being violated regardless of how well they were treated. Remarkably, most of the health providers shared that they sometimes use harsh words with women in labor so that women comply with their instructions and felt that this should not be taken directly as violence. This perspective was also reported in a study that assessed providers perspectives of practice, in which most of the providers reported to be doing these acts for the purpose of helping women instead of violence (Mwasha et al., 2023).
Providers’ views on birth companions varied, they all agreed that if the labor ward were made more comfortable, they would be willing to support it. Currently they are more concerns for the privacy of other women in labor in the same ward and workspace constraints. Similar opinions have been expressed by providers in other studies (Bohren et al., 2016). In addition, different perceptions were made of birth companions among postnatal mothers; some said they would never allow their spouse to be present because they fear their husbands will run away if they see the full delivery process.
Denying a woman her preferred birthing position was another often-stated act of violence described by participants. Some postpartum mothers went so far as saying they would prefer to give birth at home, where they have more freedom to choose their preferred positions, this perspectives also mirrors that of WHO recommendations for positive pregnancy experience that women should be allowed to choose their preferred birthing positions when possible (World Health Organization, 2016). According to other research, women are frequently forced against their choice to give birth in the lithotomy position (Savage & Castro, 2017).
Additional forms of violence that were identified in this context included sexual violence. A few women used the example of the “husband stitch,” which is when a husband asks his wife to have her vaginal hole sutured after giving birth; the procedure is carried out in secret and the provider receives payment. Similar findings were also provided in other research explaining the same husband stitch practices (Pickles, 2021).
This study identified new categories of community-related obstetric violence that need to be further researched. They included acts such as forceful use of herbal medication to speed delivery, physical violence, verbal violence from husband and relatives, inappropriate sexual practices, forced home deliveries, and psychological and emotional violence. Identifying clear categories of community-based and also health-facility obstetric violence distinguishes the current study from prior research on obstetric violence. In addition to facility-based obstetric violence, we examined community violence experience related to childbirth, which may affect pregnancy and childbirth outcomes. Furthermore, community-based obstetric violence norms may be significant drivers of violent obstetric practices and experiences at health facilities in Central Tanzania.
Strengths and Limitations
This is the first qualitative study conducted in Tanzania that explores the context-specific aspects of obstetric violence at both the community level and within health facilities. It has provided valuable insights into the perspectives on obstetric violence in this setting, marking a crucial step in the development of context specific measurement tools and enabling the creation and evaluation of interventions aimed to reduce obstetric violence and promote respectful maternity care.
The findings of this study might be subjected to the following limitations; given that the primary author conducted participant interviews, there is a possibility that this could have influenced the responses. This was mitigated by enlisting a research assistant who was well in qualitative research. Furthermore, the inclusion of data from various sources such as postnatal mothers, healthcare providers, and key community informants from diverse settings helped counterbalance this limitation. Additionally, data analysis was carried out not only by the researchers but also by other qualitative analysts who were not directly involved in the study. The inter-coding of data during analysis, and ongoing dialogue among members of the research team all contributed to enhancing the study's credibility. In addition, following components were used to ensure trustworthiness of this study which are credibility, transferability, dependability, and confirmability (Korstjens & Moser, 2018). Credibility of this study was ensured by involving different groups of participants as sources of information and different data collection methods were used during IDIs, key informant interviews and focus group discussions. Confirmability was achieved by sharing the interpretation of findings with the respondents to verify that it was the same information they shared during the interview.
Implications for Practice
Contextual components gathered by this study, might help to define what constitutes community-based and health facility-based obstetric violence based on the Tanzania context and serve as a reference. This will help in validating measurement methods, and provide a pathway for developing evidence-based interventions to reduce obstetric violence within the community and health facility and promote respectful care.
Conclusions
Moving forward in addressing obstetric violence, it is crucial to include the perspectives of both women and healthcare providers. Both groups have often been overlooked in most studies as well as the broader community. This approach will help addressing the problem in its entirety and from all angles. In this study, all categories of participants condemned these acts of obstetric violence as they contribute to women avoiding health facility care and contribute to complications experienced during home deliveries. These research findings can help shape community and health facility-level policies and programs that better guarantee all women experience positive birth experiences in accordance with WHO recommendations.
Supplemental Material
sj-pdf-1-son-10.1177_23779608251361015 - Supplemental material for “Being Treated Like an Infant Who Doesn’t Know Anything” Obstetric Violence From Perspectives of Women, Health Care Providers and Key Community Informants in Central Zone Tanzania: A Qualitative Exploratory Case Study
Supplemental material, sj-pdf-1-son-10.1177_23779608251361015 for “Being Treated Like an Infant Who Doesn’t Know Anything” Obstetric Violence From Perspectives of Women, Health Care Providers and Key Community Informants in Central Zone Tanzania: A Qualitative Exploratory Case Study by Theresia J. Masoi, Lilian Teddy Mselle, Stephen M. Kibusi and Nathanael Sirili in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251361015 - Supplemental material for “Being Treated Like an Infant Who Doesn’t Know Anything” Obstetric Violence From Perspectives of Women, Health Care Providers and Key Community Informants in Central Zone Tanzania: A Qualitative Exploratory Case Study
Supplemental material, sj-docx-2-son-10.1177_23779608251361015 for “Being Treated Like an Infant Who Doesn’t Know Anything” Obstetric Violence From Perspectives of Women, Health Care Providers and Key Community Informants in Central Zone Tanzania: A Qualitative Exploratory Case Study by Theresia J. Masoi, Lilian Teddy Mselle, Stephen M. Kibusi and Nathanael Sirili in SAGE Open Nursing
Footnotes
Acknowledgements
Heartfelt thanks to the University of Dodoma for providing support to conduct this study, Muhimbili University for providing ethical clearance, local administrative leaders at all levels, research assistants and all the research participants. Gratitude is also extended to Elisa Brettler Vandervort for assistance with manuscript review and English language editing of the final draft.
Ethical Considerations and Consent to Participate
Ethical clearance for this study was obtained from the Senate Research and Ethics Committee of the Muhimbili University of Health and Allied Sciences in Tanzania (Ref.No.DA.282/298/01.C/1758). Permission for data collection was obtained from the Ministry of Health, Ministry responsible for local government, regional and district authorities, heads of health facilities and community leaders. Written informed consent was obtained individually from each study participant before the commencing of the interview or the discussion. The objective and importance of the study were explained to study participants and they were encouraged to be free to communicate as their information would only be used for research purposes. They were further informed that their participation was purely voluntary and they could withdraw from the interview or discussion any time. Confidentiality of the information was ensured by avoiding mentioning names or titles during interview and recording. FGDs participants were assigned numbers that were kept separately from the audio record descriptions. To ensure privacy, typed notes and audio records were kept in a pined folder in a computer of the first author that was only accessible to her. Only the transcripts were shared with other authors.
Authors’ Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received some funds from the University of Dodoma to support her doctoral study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data regarding this study are available upon request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.