
Abstract
Introduction
Asphyxia at birth remains the leading cause of neonatal morbidity and mortality worldwide, accounting for ∼23% of all neonatal deaths. Although the causes vary from country to country, early identification and treatment of risk factors can improve the situation.
Objectives
To determine the risk factors of birth asphyxia in hospital-delivered neonates in Dodoma, Tanzania.
Methods
A matched case-control study was conducted from May to July 2017 at Dodoma Region Referral Hospital. Data were collected using a semistructured questionnaire and a standard antenatal care index card. Cases were neonates diagnosed with asphyxia at birth (N = 100), while controls were neonates not diagnosed with asphyxia at birth (N = 300). A binary logistic regression model was used to assess the independent variables associated with birth asphyxia and reported as crude and adjusted odds ratios along with their 95% confidence intervals.
Results
A total of 400 newborns and their birth mothers were involved in the study. The average age of the case mothers was 26.9 years (SD = 7.85) and that of the control mothers was 27.24 years (SD = 6.08). Place of residence, anemia, maternal age, prenatal visits attended, use of herbs during labor, previously complicated pregnancy, duration of labor, meconium-stained amniotic fluid, and mode of delivery were predictors of birth asphyxia.
Conclusion
The study showed that most predictors of birth asphyxia can be prevented. The results suggest appropriate health education before conception, effective follow-up through prenatal care, early identification and treatment of high-risk pregnant women, and proper monitoring of labor and delivery.
Introduction
Birth asphyxia is the failure to initiate or maintain spontaneous breathing during birth, resulting from a lack of blood flow or gas exchange to or from the fetus in the period immediately before, during, or after the birth process (Gillam-Krakauer & Gowen Jr., 2022). Birth asphyxia is still a major clinical problem affecting global neonatal morbidity and mortality (World Health Organization, 2022). The global incidence of birth asphyxia is estimated to be 2–10 per 1,000 term newborns and is higher in developing countries than in developed countries. In Africa, asphyxia at birth accounts for 24.0%, with East and Central Africa accounting for the largest proportion (15.9%) (Workineh et al., 2020). Approximately 2.4 million newborns die each year worldwide, and birth asphyxia is reported to be responsible for ∼23% of all deaths, of which more than 90% come from low- and middle-income countries (World Health Organization, 2022). In Tanzania, the neonatal mortality rate is 20 out of 1000, and more than 25% of these deaths are due to birth asphyxia (Ahmady et al., 2020).
When asphyxia occurs during birth, the infant is deprived of oxygen, resulting in physical damage to vital organs, most commonly the brain (Adhikari & Rao, 2017; Samad et al., 2016). Under extreme circumstances, birth asphyxia can quickly lead to serious problems such as increasing hypoxia, significant metabolic acidosis, and hypercapnia (Collins & Popek, 2018; Moshiro et al., 2019), and even pose a threat to life. The results reported long-term complications of birth asphyxia such as cerebral palsy (Ahearne, 2016; Thoresen et al., 2021; Zhang et al., 2020), epilepsy (Adhikari & Rao, 2017; Xiao et al., 2019), impaired neural cognitive development (Adhikari & Rao, 2017; Kivi et al., 2022; Seikku et al., 2016), reduced vision (Adhikari & Rao, 2017; Chong et al., 2019), and hearing impairment (Adhikari & Rao, 2017; Aziza & Yuldashev, 2022).
Review of the Literature
Although there is wide variation in the determinants of birth asphyxia across countries, studies have classified the predictors into antepartum, intrapartum, and postpartum factors (Wodajo et al., 2019; Yadav & Damke, 2017). The reported independent antepartum predictors of birth asphyxia were maternal age, educational level, antenatal care clinic (ANC), parity, gravidity, maternal prothrombotic disorders, antepartum hemorrhage, thyroid disease, chronic hypertension, diabetes mellitus, place of residence, and anemia (Baye et al., 2021; Fekede et al., 2022; Ilah et al., 2015; Nadeem et al., 2021; Woday et al., 2019). Intrapartum factors included acute fetal distress, chorioamnionitis, mode of delivery, umbilical cord complications, uterine rupture, prolonged labor, meconium-stained amniotic fluid, multiple births, fetal presentation, and premature and prolonged rupture of membranes (Collins & Popek, 2018; Nadeem et al., 2021; Tegegnework et al., 2022; Wodajo et al., 2019; Woday et al., 2019; Workineh et al., 2020). Postpartum factors included preterm birth and pulmonary, neurological, and cardiovascular abnormalities in newborns (Collins & Popek, 2018).
Birth asphyxia is preventable, but once asphyxia occurs, the associated consequences are almost untreatable (Locatelli et al., 2020). To reduce the burden of birth asphyxia, preventive interventions based on the predictive factors need to be developed (Usman et al., 2019). Therefore, the aim of this study was to investigate the risk factors for birth asphyxia in hospital-delivered neonates in Dodoma, Tanzania.
Methods
Study Design
This was a facility-based matched case-control study conducted from May to August 2017 to investigate risk factors for birth asphyxia in hospital-delivered neonates in Dodoma region, central Tanzania. Dodoma is the capital of Tanzania and one of the fastest-growing regions with a population of 3,085,625 (Tanzania National Bureau of Statistics, 2022). Dodoma Region Referral Hospital is the largest public hospital with a large maternity and neonatal unit. It offers daily delivery services carried out by 19 midwives, five general practitioners, and three gynecologists. All newborns diagnosed with asphyxia at birth are admitted and cared for in the Level III neonatal intensive care unit until discharged home or referred for further treatment. Normal newborns are admitted to the postpartum ward for observation 24 to 48 hours after delivery and then discharged home.
Research Questions
What antepartum risk factors are associated with birth asphyxia in hospital-delivered neonates in Dodoma, Tanzania? What intrapartum risk factors are associated with birth asphyxia in hospital-delivered neonates in Dodoma, Tanzania?
Sample
The sample size was determined with EPI INFO version 3.5.1 Stat Calculation statistical software using the double population proportion formula for a matched case-control study. The study adopted 50% of hospital-born neonates without birth asphyxia with an odds ratio (OR) of 2.0 (Pitsawong, 2011). Assuming a standard normal error of 5%, a power of 80%, and a case-to-control ratio of 1:3, the researchers obtained 388 respondents. Adding the nonresponse rate of 6.1% results in a total sample size of 412 (103 cases and 309 controls). However, of the calculated cases, three were excluded during data collection because two had major congenital anomalies (hydrocephaly and congenital heart defects) and one had low birth weight (2.43 kg; Figure 1). Risk-based sampling was used. Each case was matched to three controls based on gestational age and birth weight.

Sampling process of the newborns involved in the study.
Inclusion Criteria and Exclusion Criteria
Newborns born to their biological mother at 37 weeks of age or later were eligible for this study. Inclusion criteria for cases were neonates diagnosed with asphyxia at birth according to the national guideline (Apgar score ≤ 7 at 5 min, inability to initiate and maintain breathing, ongoing need for resuscitation, and presence of multiple organ failure). Control subjects were neonates not diagnosed with asphyxia at birth (Apgar score >7 at 5 min, ability to initiate and maintain breathing, and no multiple organ failure). Exclusion criteria were neonates born at 37 weeks of age or older but with severe congenital malformations, intrauterine growth restriction, and low birth weight.
Study Measures
The dependent variable was birth asphyxia, while the independent variables were social demographic characteristics and antepartum and intrapartum factors. The independent variables were measured using a semistructured questionnaire adapted from Tabassum et al. (2014), and the standard ANC index card. The questionnaire was first prepared in English, then translated into Swahili (the national language in the study area), and then translated back into English to ensure consistency. Before the actual data collection, a pretest of the questionnaire was carried out on 15 newborns and their biological mothers. The tool was then modified and adjusted based on the pretest results to ensure validity.
Data Collection Procedures
Data collection was carried out by three experienced nurses under the supervision of a midwife who received two days of training on the questionnaire. Data were collected from each case in the labor ward or neonatal intensive care unit, followed by three controls in the postnatal ward. The supervisor monitored the data collection process on-site daily. The principal investigator conducted a daily review of collected data for completeness, precision, and consistency.
Ethical Considerations
Ethical approval for this study was granted by the Institutional Research Ethics Committee. The regional medical officer approved a letter requesting permission for data collection. Before the interview, the study was explained to all participants and both oral and written informed consent was obtained. Strict confidentiality was maintained throughout the study.
Statistical Analysis
Analysis was performed using SPSS for Windows version 20. Descriptive analysis including frequencies and percentages was performed to describe the study participants. To determine the relationship between dependent and independent variables, a chi-square test was performed. All factors that showed a strong association in the 95% confidence interval (CI) with a p ≤ .05 were included in the bivariate logistic regression analysis and the crude OR (COR) was determined. To control for confounding factors, all variables with p ≤ .25 (Zhang, 2016) were subjected to the multivariable logistic regression model to obtain the adjusted OR (AOR), and factors were considered significant predictors when p ≤ .05 at the 95% CI.
Results
Social Demographic Characteristics of the Study Participant
A total of 400 newborns (100 cases and 300 controls) and their biological mothers were involved in the study with a response rate of 97.1%. The average age of the mothers in the case group was 26.9, SD = 7.85 years and that of the control group was 27.24 SD = 6.08 years. In the cases, 25 (25%) mothers and in the control group 30 (10%) mothers were >35 years old. Regarding parity, 16 (16%) mothers in the cases and 21 (7%) mothers in the control group had more than four children. Sixty-five (65.0%) mothers in the cases and 151 (50.3%) mothers in the control group lived in the rural part of the study area. Unexpectedly, 61 (61%) of the mothers with asphyxiated newborns and 148 (49.3%) of the mothers with non asphyxiated newborns had secondary school education. More than half (52%) of neonates with asphyxia and 140 (46.7%) of neonates without asphyxia at birth were male (Table 1).
Social Demographic Characteristics of Cases and Control (N = 400) in Dodoma, Tanzania, 2017.

Antepartum Risk Factors for Birth Asphyxia Among Neonates (N = 400)
Regarding antepartum risk factors for birth asphyxia, the study examined maternal anemia, ANC booking and number of ANC visits attended, maternal age, parity, use of herbal medicines during labor, maternal education level, and place of residence. The results showed that the presence or absence of asphyxia at birth was significantly associated with maternal age (p ≤ .001), parity (p = .026), place of residence (p = .011), antenatal visits (p ≤ .001), anemia (p = .025), and use of herbal medicines during labor (p = .034; Table 2).
Antepartum Risk Factors, for Birth Asphyxia Among Hospital-Delivered Neonates in Dodoma, Tanzania (N = 400, Chi-Square Test), 2017.

Note. ANC = antenatal care clinic.
After adjusting for other variables, maternal age, place of residence, early timing of first ANC visit, number of ANC visits attended, maternal anemia, and use of herbal medicines during labor were the significant determinants of birth asphyxia. Results showed that mothers aged <20 years and >35 years had a higher risk of delivering newborns with asphyxia (p = .002); AOR = 4.49, 95% confidence interval [CI] = [1.763, 11.437]) and (p = .008; AOR = 2.611[ 95% CI = [1.288, 5.294]) each compared to mothers aged 20 to 35 years. It was observed that newborns born to mothers in rural areas had a higher risk of birth asphyxia (p = .022; AOR = 1.84; 95% CI = [1.091, 3.123]) compared to mothers in urban areas. Newborns born to mothers who delayed attending the antenatal clinic had a higher risk of birth asphyxia (p = .014; AOR = 0.207; 95% CI = [0.059, 0.724]) compared to those whose mothers started their first ANC visit early. Birth asphyxia was higher in neonates whose mothers attended fewer than four ANC visits (p = .003; AOR = 6.27, 95% CI = [1.842, 21.362]) compared to newborns whose mothers attended more than four ANC visits. Newborns born to mothers who suffered from anemia during pregnancy had a higher risk of birth asphyxia (p = .046; AOR = 1.883; 95% CI = [1.011, 3.510]) compared to those who did not have anemia. Newborns whose mothers took herbal medications during labor had a higher risk of birth asphyxia (p = .021; AOR = 3.226; 95% CI = [1.191, 8.739]) than mothers who did not consume herbs (Table 3).
Bivariate and Multivariable Logistic Regression for the Antepartum Risk Factors for B.A Among Neonates in Dodoma, Tanzania (N = 400), 2017.

Note. COR = crude odds ratio; AOR = adjusted odds ratio; CI = confidence interval; ANC = antenatal care clinic.
Intrapartum Risk Factors for Birth Asphyxia in Newborns in the Dodoma Region of Tanzania
Regarding the intrapartum risk factors associated with birth asphyxia, the study examined the history of complications in the previous pregnancy, duration of labor, timing of rupture of membranes, meconium-stained amniotic fluid, mode of delivery, and the type of delivery, onset of labor, umbilical cord complications, and other complications during labor. The results show that there is a significant association between asphyxia at birth and the duration of labor (p ≤ .001), meconium-containing amniotic fluid (p ≤ .001), and other complications during delivery (p ≤ .001; Table 4).
Intrapartum Risk Factors for Birth Asphyxia Among Hospital-Delivered Neonates in Dodoma, Tanzania (N = 400 Chi Square), 2017.

Note. PROM = prerupture of membrane; SVD = spontaneous vaginal delivery. *p-value are the fishers exact p-value.
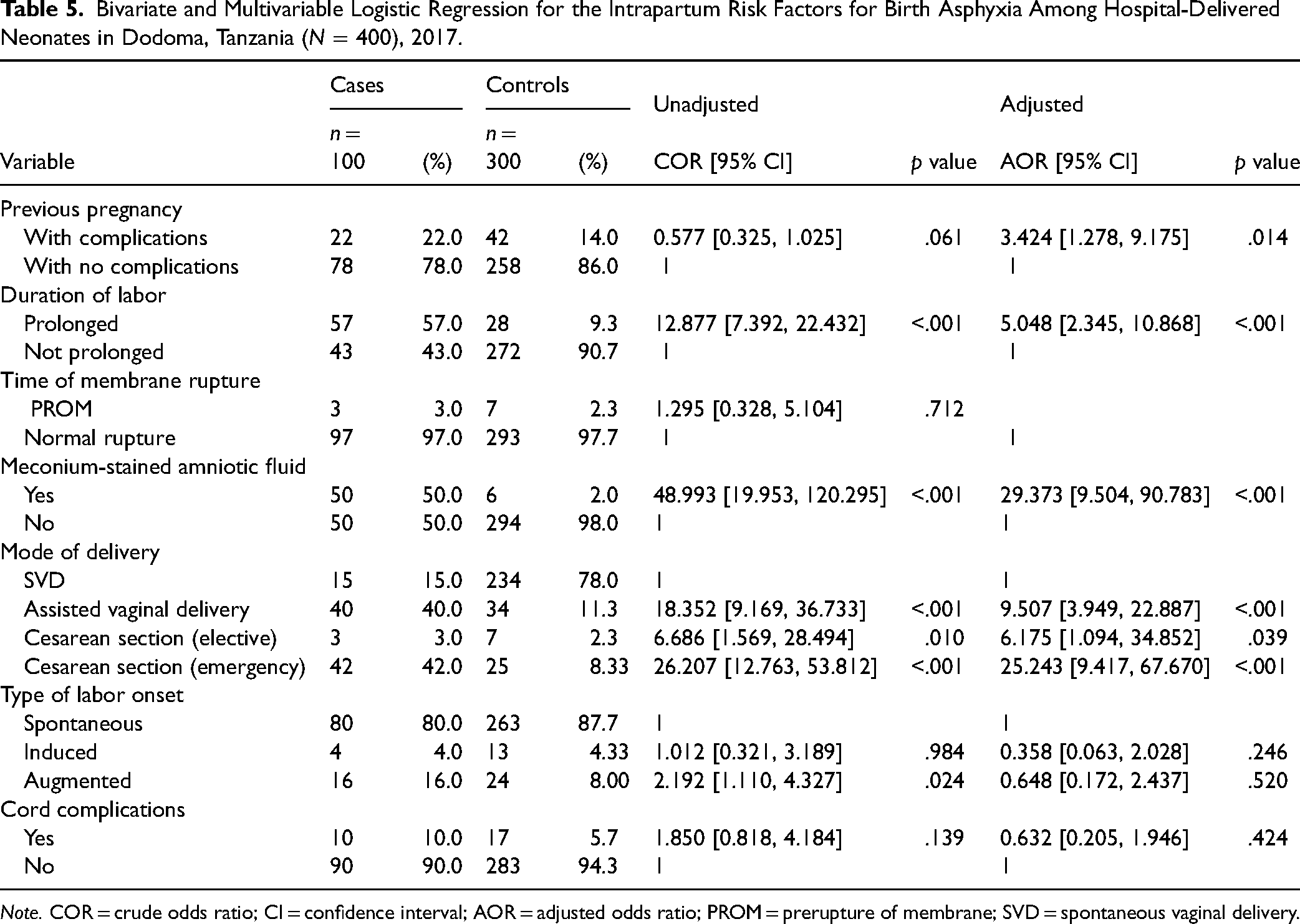
After controlling for other variables, birth asphyxia was observed to be significantly predicted by complications in the previous pregnancy (p = .014), duration of labor (p ≤ .001), meconium-stained amniotic fluid (p ≤ .001), assisted vaginal delivery (p ≤ .001), elective cesarean section (p = .039), and emergency cesarean section (p ≤ .001).
It was observed that newborns of mothers who had complications in the previous pregnancy had a higher risk of birth asphyxia (p = .014; AOR = 3.424, 95% CI = [1.278, 9.175]) compared to mothers who had no complications. Newborns born to mothers who had prolonged labor had a higher risk of birth asphyxia (p ≤ .001; AOR = 5.048; 95% CI = [2.345, 10.868]) compared to newborns whose Mothers in labor had normal contractions. Newborns of mothers who had an assisted vaginal delivery, an elective cesarean section, or an emergency cesarean section had a higher risk of birth asphyxia (p ≤ .001; AOR = 9.507; 95% CI = [3.949, 22.887]), (p = .039; AOR = 6.175; 95% CI = [1.094, 34.852]), and (p ≤ .001; AOR = 25.243; 95% CI = [9.417, 67.670]) each compared to spontaneously delivered neonates (Table 5).
Bivariate and Multivariable Logistic Regression for the Intrapartum Risk Factors for Birth Asphyxia Among Hospital-Delivered Neonates in Dodoma, Tanzania (N = 400), 2017.
Note. COR = crude odds ratio; CI = confidence interval; AOR = adjusted odds ratio; PROM = prerupture of membrane; SVD = spontaneous vaginal delivery.
Discussion
The aim of the study was to identify the predictors of birth asphyxia in hospital-delivered neonates in Dodoma, Tanzania. Maternal age, place of residence, maternal anemia, early timing of ANC visits, number of ANC visits attended, herbal medications, complications in previous pregnancies, prolonged labor, and mode of delivery were the independent risk factors for birth asphyxia.
Newborns born to mothers younger than 20 years had a higher risk of birth asphyxia than mothers aged 20 to 35 years. This is similar to Aslam et al. (2014), and Yadav and Damke (2017). The most likely explanation is that adolescent pregnancy is common in the area we studied. These young women may have lacked support from their partners and therefore had poor prenatal care and inadequate birth preparation. Likewise, in this study, birth asphyxia was higher in newborns born to mothers of advanced age (>35 years) than in mothers aged 20 to 35 years. The results are similar (Abdo et al., 2019) and could be influenced by the association between older maternal age and a higher risk of adverse neonatal outcomes (Laopaiboon et al., 2014). However, the result is contradictory to Nayeri et al. (2012) and Tewesa et al. (2017) who found that maternal age was not a risk factor for birth asphyxia. This discrepancy could be explained by differences in sample size and the settings in which the research was conducted.
Mothers in rural areas had a higher risk of delivering their babies asphyxiated than mothers in urban areas. The results are consistent with Aslam et al. (2014) and Wodajo et al. (2019). The plausible explanation is that mothers in rural areas may have inadequate utilization of maternal health services and limited access to health facilities.
Compared to Senbeta et al. (2022), the risk of birth asphyxia was higher in anemic mothers than in mothers without anemia. The reason could be that maternal anemia can reduce the oxygen supply to the fetus and therefore lead to intrapartum hypoxia (Baev et al., 2022).
Mothers who attended fewer than four ANC visits had a higher risk of birth asphyxia than mothers who attended more than four visits. This is consistent with Ilah et al. (2015), Senbeta et al. (2022), and Tegegnework et al. (2022). This may be because care at each ANC visit significantly improves the assessment of fetal well-being and early detection and treatment of at-risk mothers. However, the results are contradictory to Nayeri et al. (2012) and Tewesa et al. (2017) who found that ANC follow-up is not associated with birth asphyxia. This discrepancy could be due to the different sample sizes used in these studies.
Taking herbal medicines during labor increased the risk of birth asphyxia compared to mothers who did not take herbal medicines. Although Purnamawati and Ariawan (2012) found similar results, Kekana et al. (2020) reported no significant association between herbal medicine use and birth asphyxia. This can be explained by the fact that the current study focuses on herbal medicines during labor, while the other study examines their use during pregnancy.
Comparable to previous studies (Alamneh et al., 2022; Fekede et al., 2022; Meshesha et al., 2020; Tegegnework et al., 2022), mothers with longer labor (>12 h) had a higher risk of birth asphyxia than mothers without prolonged labor. The reason may be that prolonged labor is typically caused by slow dilatation of the cervix, large babies, pelvic disproportion, and improper presentation of the fetus (Gaudernack et al., 2020; Ahmady et al., 2020). All of these can affect the supply of oxygen from the mother to the fetus via the placenta.
Mothers who had an assisted vaginal delivery and cesarean section had a higher risk of birth asphyxia than mothers with spontaneous vaginal delivery (SVD). The results are consistent with the observations of Ibrahim et al. (2017), Ilah et al. (2015) and Woday et al. (2019). Reasons for this may be that most indications for assisted vaginal delivery and cesarean section are due to medical conditions that affect the oxygen supply between mother and fetus. However, on the other hand, the findings contradicted (Tewesa et al., 2017) who found that the mode of delivery was not associated with birth asphyxia. This difference may be explained by the different sample sizes used in these studies.
Birth asphyxia was higher in mothers with meconium-containing amniotic fluid than in mothers with clear amniotic fluid, similar to Tegegnework et al. (2022), and Woday et al. (2019). This is because meconium staining is often associated with prolonged and obstructed labor. If a fetus inhales meconium, it can lead to chemical pneumonitis, pneumonia, and ultimately hypoxia (Collins & Popek, 2018).
The study also found that mothers who had complications in their previous pregnancies had a higher risk of birth asphyxia than mothers who had no complications. The results are comparable to those in Pakistan, Nigeria, and India (Aslam et al., 2014; Ilah et al., 2015; Yadav & Damke, 2017). This could be because some pregnancy complications tend to recur and therefore lead to intrapartum complications leading to birth asphyxia.
Strength and Limitation
The strength of this study lies in the use of case control, which is the appropriate design to establish the cause–effect relationship. However, the results should be viewed with caution as the newborns examined were diagnosed with asphyxia at birth in accordance with national guidelines. Laboratory studies such as arterial blood gas analysis to determine biological markers of fetal metabolic acidosis have not been performed due to limited resources. Furthermore, the results cannot be generalized because the hospital studied is a referral hospital that receives mothers with maternal complications from several primary health facilities in the region.
Implication for Practice
The study highlights the importance of public health education for men and women of childbearing age regarding preconception and prenatal care, childbirth preparation, and healthy pregnancy behaviors. The study also highlights the need for supportive supervision and ongoing training for pediatric nurses, midwives, and other obstetric professionals to improve their skills in prenatal care, early risk identification, labor and delivery, and neonatal resuscitation. Additionally, it is critical that hospitals improve their emergency obstetric referral system. Furthermore, these baseline data in the study area can be used by multiple stakeholders to jointly develop preventive measures against birth asphyxia.
Conclusion and Recommendation
The study showed that most predictors of birth asphyxia can be prevented. The results suggest appropriate health education before conception, effective follow-up through prenatal care, early identification and treatment of high-risk pregnant women, and proper monitoring of labor and delivery. In addition, the study recommends further research to investigate the determinants of birth asphyxia in rural primary healthcare settings to determine the true burden of asphyxia, as the hospital used is a referral hospital that admits mothers with multiple obstetric complications.
Footnotes
Acknowledgments
The authors would like to thank Dodoma Region Referral Hospital for allowing them to conduct the study. The authors also thank the data collectors and supervisors for their tireless efforts in data collection.
Data Availability
The data used in this study are available from the corresponding author upon special request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article