
Abstract
Introduction
Childhood diarrhea remains a leading cause of death in children under 5 years of age worldwide, although the disease is both preventable and treatable. Effective caregiver involvement, rotavirus vaccinations, and parallel diarrhea prevention are critical.
Objectives
This study aimed to assess caregiver's knowledge of childhood diarrheal disease prevention, rotavirus vaccination knowledge, and associated factors in Dodoma, Tanzania.
Methods
A hospital-based analytical cross-sectional study was conducted at Makole Health Center, Dodoma. Data were collected from 274 caregivers of children under 5 years of age who attended a routine immunization clinic. Respondents were interviewed using a semi-structured, pretested questionnaire. Data were analyzed for frequency, percentages, and mean, followed by multivariable linear logistic regression to examine the association between sociodemographic factors and caregiver's knowledge.
Results
A total of 274 subjects were involved in the study. The majority (93.8%) were women, all had formal education, (62.8%) knew that diarrhea in children can be prevented by proper handwashing, and only (9.9%) knew about the rotavirus vaccine. Educational level (β = 0.565 CI; 0.490, 0.873) p-value < .001, age of parents (β = 0.738 CI; 0.427, 1.050) p-value .022 and age of child (β = −0.306 CI; − 0.490, −0.122), p-value <.001 and the fact that the child was male (β = 1.116, 95% CI = 0.712, 1.520) p-value < .001) were the factors associated with participants’ knowledge.
Conclusion
The results highlight the great need for public health programs to increase awareness of rotavirus vaccines and parallel diarrhea prevention interventions, which in turn will significantly improve caregivers’ knowledge and therefore the prevention of diarrhea in children
Introduction
Childhood diarrheal disease represents a serious public health problem and remains the leading cause of morbidity and mortality in children under 5 years of age worldwide (Cohen et al., 2022). Diarrhea is defined as three or more loose or liquid stools within 24 hr, occurring more frequently than normal in an individual child (World Health Organization, 2024). Diarrheal diseases account for more than 60% of the disease burden in children under 5 years of age worldwide, contributing to nearly 1.7 billion cases with more than 425,000 deaths per year (World Health Organization, 2024). Despite the dramatic decline in diarrheal mortality and morbidity among children under 5 years of age as part of global achievement of the MDG targets, diarrheal cases had only fallen from 11% in 2010 to 9% in 2015 (Drisse et al., 2017). In developing countries, diarrhea is responsible for one in eight deaths in children under five (Kotloff, 2017). In Tanzania, the under-five mortality rate has decreased from 147 to 54 deaths per 1,000 live births (Koffi et al., 2020). However, despite the significant rate of decline, Tanzania is reportedly the eighth country with the highest number of deaths among children under five, and diarrhea is reported as the fourth leading cause of death in children aged 6–59 months at 27% (Koffi et al., 2020).
Children with diarrhea may experience dehydration and changes in fluid and electrolyte balance (Demissie et al., 2021). Untreated childhood diarrhea may be associated with recurrent attacks and often results in severe dehydration, electrolyte imbalances, hypotension, hypovolemic shock, inflammatory and absorptive disorders, septic bacterial infections, renal failure, other multiple organ failure, underweight, reduced growth and development, decreased appetite and poor food intake and ultimately death (Getu Debalkie Demissie et al., 2021; Troeger et al., 2021; Workie et al., 2018). This data is alarming and shows that preventive measures are of great importance.
Childhood diarrheal diseases are caused by a variety of microorganisms, including bacteria, viruses, and protozoa (Kotloff, 2017). The most commonly reported pathogens worldwide are enteric viruses and diarrhea-causing E. coli (DEC) (Kotloff, 2017; Troeger et al., 2021) with rotaviruses being the most common cause of the most severe deaths from acute watery diarrhea in young children worldwide (Troeger et al., 2021). Rotavirus is responsible for more than 200,000 deaths in children each year, with low-income countries accounting for the majority of these deaths (Derso et al., 2020). Research reports show that proper breastfeeding, hand washing, and hygiene practices have resulted in a significant reduction in the diarrhea problem caused by intestinal bacteria and protozoa (Baye et al., 2021; Bennion et al., 2021; Kabhele et al., 2018; Mutuku & Ochieng, 2020; Workie et al., 2018) but have less influence on rotavirus. To protect young children from rotavirus diarrheal infections, a rotavirus vaccine has been developed and is now being included in routine national vaccination programs, particularly in areas where the disease is more common (Kurugöl, 2009; Parashar et al., 2016). The vaccines prevent 15–34% of severe diarrheal illnesses in developing countries and 37–96% of severe diarrheal illnesses in developed countries (Parashar et al., 2016). To achieve a significant reduction in diarrheal disease in children under 5 years of age, parallel interventions, e.g., rotavirus vaccines and other preventive measures against diarrheal disease are recommended, particularly in developing countries where hygiene and access to quality care remain a challenge (Baye et al., 2021; Parashar et al., 2016)
Review of the Literature
The main risk factors contributing to the high prevalence of diarrheal disease among children under 5 years of age in developing countries are suboptimal breastfeeding (Ogbo et al., 2018), improper handwashing, unhygienic handling of drinking water or food, contaminated infant formula, low rotavirus vaccination rates, and uneducated Parents (Derso et al., 2020; Kapwata et al., 2018; Troeger et al., 2021). These results indicate that it is very important to understand caregivers’ knowledge of diarrhea in children, as this may aid in prevention strategies. Informed parents are also more likely to recognize symptoms early, seek medical care, and adhere to treatment plans. However, parents’ level of knowledge varies greatly. Studies have shown that more than 35% of parents had no knowledge about preventive measures against diarrheal diseases (Elnadif & Abdalla, 2022; Turyare et al., 2020). Likewise, it is reported that parents were inadequately informed about the risk factors, causes, complications, preventive measures, signs and symptoms of dehydration, and the relevance of ORS applications as a primary treatment component for acute watery diarrhea (Chaudhary et al., 2014; Joya et al., 2022)
Regarding caregivers’ knowledge about rotavirus infection and vaccination, it was found that more than 60% of mothers/caregivers were uninformed. The mothers did not know what age of children this vaccine is suitable for, how many doses the child should receive, what diseases it prevents, and how to deal with the side effects of the vaccine (Ahmed, 2017; Pratiwi & Kristina, 2020). Caregivers’ low level of knowledge about diarrheal diseases, rotavirus vaccines, and other preventive measures is often related to parents’ age, mother's education level, marital status, vaccination information source, number of children, and economic status (Ahmed, 2017; Elnadif & Abdalla, 2022; Pratiwi & Kristina, 2020).
Mothers and caregivers are recommended to wash their hands with soap before preparing food, feeding their children, and after using the toilet, as diarrheal diseases are transmitted through feco-oral transmission(Kirk et al., 2017; Wolf et al., 2019). In addition, all children under 5 years of age must be vaccinated against rotavirus to significantly prevent diarrhea and its associated complications (Kotloff, 2017; Troeger et al., 2021)
Despite these available facts, there is limited data on whether caregivers of children under 5 years of age in our setting are informed about strategies for diarrhea prevention in children. Therefore, this study aimed to assess the knowledge of caregivers of children under 5 years of age about rotavirus vaccination, other strategies to prevent childhood diarrheal disease, and associated factors in Dodoma, Tanzania.
Methods
Study Design
A hospital-based cross-sectional analytic study was conducted. The study population consisted of all caregivers of children between 3 and 59 months of age who had ever brought the child to the clinic for routine childhood vaccination. Caregivers were used to determine the level of knowledge about diarrheal disease prevention strategies and associated factors. The study was conducted in the Dodoma region of central Tanzania. With a population of 3,085,625, it is one of the fastest-growing cities in Tanzania.
Research Hypothesis
Hypothesis 1: Caregivers of children under 5 years of age have varying levels of knowledge about how to prevent diarrheal illness in children. People with formal education tend to be more knowledgeable than people without formal education.
Hypothesis 2: There is a strong relationship between caregivers’ knowledge about childhood diarrhea and several factors such as parental age, income level, education level, marital status, and access to health information. Higher socioeconomic status and higher education levels are associated with higher levels of knowledge among caregivers of children under 5 years of age.
Research Questions
What level of knowledge do caregivers of children under five have about strategies to prevent childhood diarrhea?
What factors are associated with knowledge of childhood diarrhea prevention strategies among caregivers of children under five?
Sample
The sample was calculated using Kish and Leslie formula n = z2xp (1−p)/e2. Where z is the standard normal deviation = 95% of the confidence interval of 1.96, p is the expected prevalence of .34 based on a previous study (Kabhele et al., 2018) and e is the level of precision at 0.05. The calculated sample size was then 344.8 ≈ 345 caregivers of children under 5 years of age. However, only 277 participants were reached from the calculated sample size. Of the 277, three participants refused consent, therefore data from 274 participants were collected and analyzed (Figure 1). Dodoma City Council has two large public health centers offering childhood vaccination clinics, with one center randomly selected for the study to minimize bias, ensure representativeness, and thus improve the generalizability of the results. Study participants were selected using a simple random sampling method. Parents who arrived at the clinic each day received a numbered slip of paper. Those with even numbers were selected until the sample size was reached. This minimizes selection bias and increases the validity of the study results.

Participant recruitment flow diagram.
Inclusion and Exclusion Criteria
To be included in the study, a caregiver had to be either a parent or significant guardian who had stayed with a child for at least 2 months and frequently brought the child to routine child development clinics and vaccinations. Excluded from the study were key guardians who stayed with the child for less than 2 months, as well as caregivers whose children were seriously ill or refused consent.
Study Measures
The sociodemographic variables included as predictors of the outcome variables are eight items: age of caregiver (in years—continuous), age of child (in months—continuous), gender of caregiver (nominal) and gender of child (nominal), education level (ordinal), number of children (continuous), place of residence (nominal), and child–parent ratio (nominal). These variables were assessed using a social demographic questionnaire created by the research team based on information from previous studies (Adeleke & Mhlaba, 2019; Workie et al., 2018).
Knowledge about diarrheal disease prevention was measured using a questionnaire adapted from previous study (Adeleke & Mhlaba, 2019). A questionnaire with eight yes/no items: pathogen causing diarrhea, mode of transmission, toilet use, proper hand washing, breastfeeding, combination of rotavirus vaccines and other preventive measures, ORS applications to treat diarrhea at home, use of antibiotics, and impact of untreated diarrhea. Each item had a value of 1, which corresponded to the correct answer, and a value of 0, which corresponded to the incorrect answer. The variable “Knowledge about preventing diarrheal diseases” could be rated with values from 0 to 8, with a higher value indicating better knowledge. A pilot study was conducted in Makole health centers with 25 caregivers of children under 5 years of age to ensure that the questionnaire provided high-quality data. The insights gained from the pilot study were used to improve the questionnaire. In order to improve the content validity of the questionnaire, the expert also checked it.
Knowledge about the rotavirus vaccine was measured using a questionnaire adapted from studies in Nigeria and Italy (Babatola et al., 2020; Napolitano et al., 2019). A questionnaire with 10 yes/no points on the following topics: method of transmission of rotavirus, route of vaccine administration, number of doses of vaccine required, time for administration of the first dose, time for administration of the second dose, missed vaccination, vaccination safety, vaccination schedule and costs, breastfeeding after vaccination, and the disease against which the rotavirus vaccination protects. A value of 1 was assigned for each correct item and a value of 0 for an incorrect answer. Therefore, the value for the variable “Knowledge about rotavirus vaccines” is between 0 and 10, with a higher value indicating better knowledge.
Data Collection Procedures
Data collection took place from July to August in 2021. Data collection was carried out by a trained research assistant who was trained in the data collection procedure and questionnaire for 3 days. The trained research assistant conducted the questionnaire in a personal interview with the participants. Data were collected in the vaccination waiting area of the clinic for children under 5 years old at Makole Health Center.
Ethical Considerations
The study received ethical approval from the institution's research ethics committee. Participants signed an informed consent form before data collection. Participation was voluntary and confidentiality was maintained throughout the study.
Statistical Analysis
Data were analyzed using SPSS version 26. Descriptive frequency, percentage, and mean analyses were used to describe sample characteristics and knowledge levels of caregivers under 5 years of age about diarrheal disease prevention strategies and rotavirus vaccines. The association between sociodemographic factors and knowledge of caregivers under 5 years of age was examined using linear regression analysis. All factors that were statistically significant in bivariable analyses at a p-value ≤ .02 were included in multivariable linear regression models to account for confounding variables. The significant factors were determined by a p-value <.05 and presented as a β-coefficient with their 95% confidence intervals (CI).
Results
Social Demographic Characteristics of the Study Participants
A total of 274 caregivers consented and participated in the study, accounting for 79.4% of the calculated sample. Table 1 summarizes the sociodemographic characteristics of the caregivers and children. The average age of the caregivers was 28.34 years, standard deviation (SD) = 5.32 and that of the children was 1.26 months, SD = 0.87. The vast majority of caregivers (n = 257, 93.8%) were women. More than half (n = 167, 60.9%) had primary school education, while all the remainder had secondary school education. Table 1
Social Demographic Characteristics of the Study Participants N = 274.

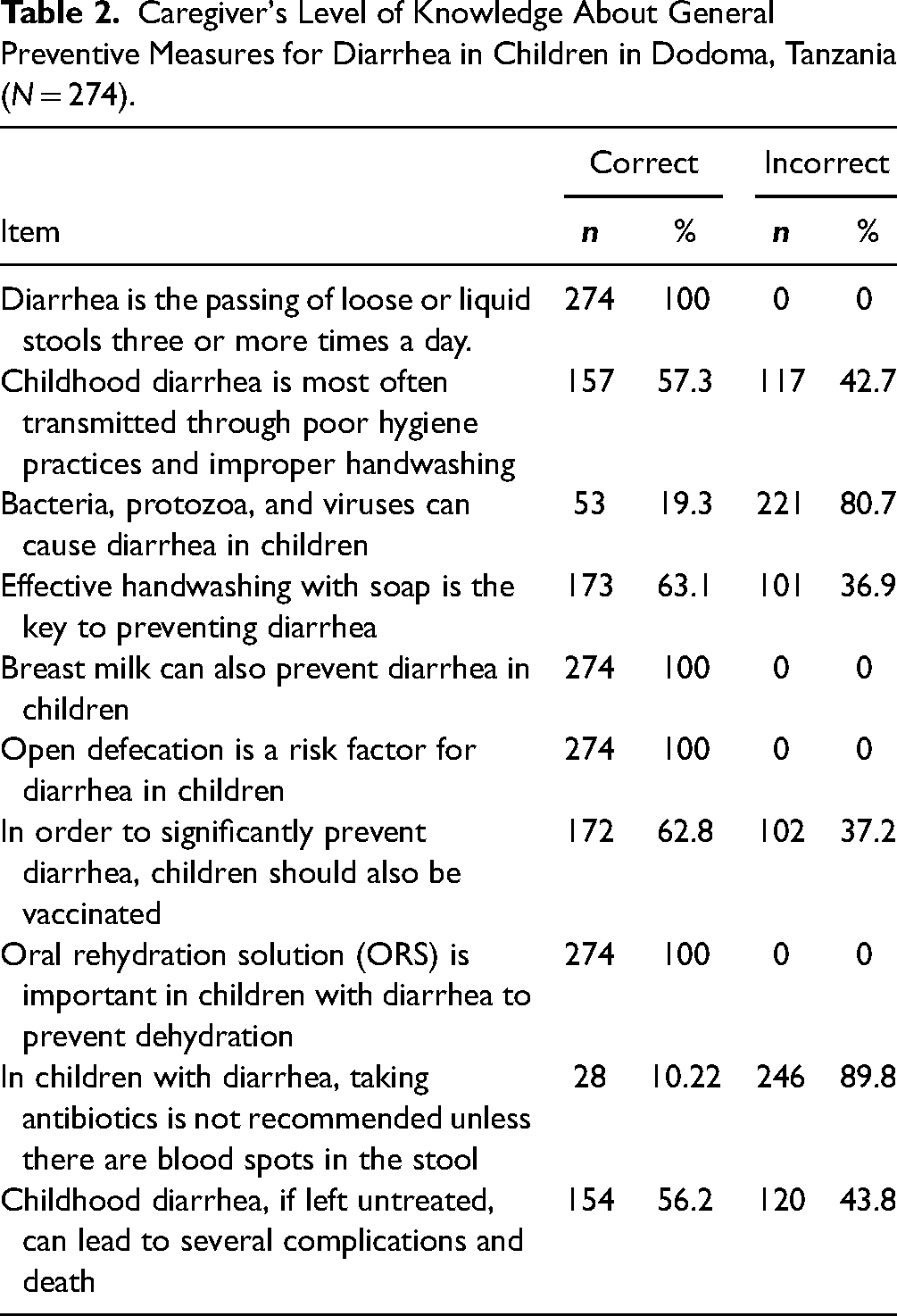
Caregiver's Level of Knowledge About General Preventive Measures for Diarrhea in Children
All respondents (n = 274, 100%) correctly defined diarrhea as passing loose or liquid stool three or more times per day. The overall average score of the caregiver's knowledge of general preventive measures for diarrhea in children was 7.058, SD = 1.327, the analysis of other items is shown in Table 2
Caregiver's Level of Knowledge About General Preventive Measures for Diarrhea in Children in Dodoma, Tanzania (N = 274).
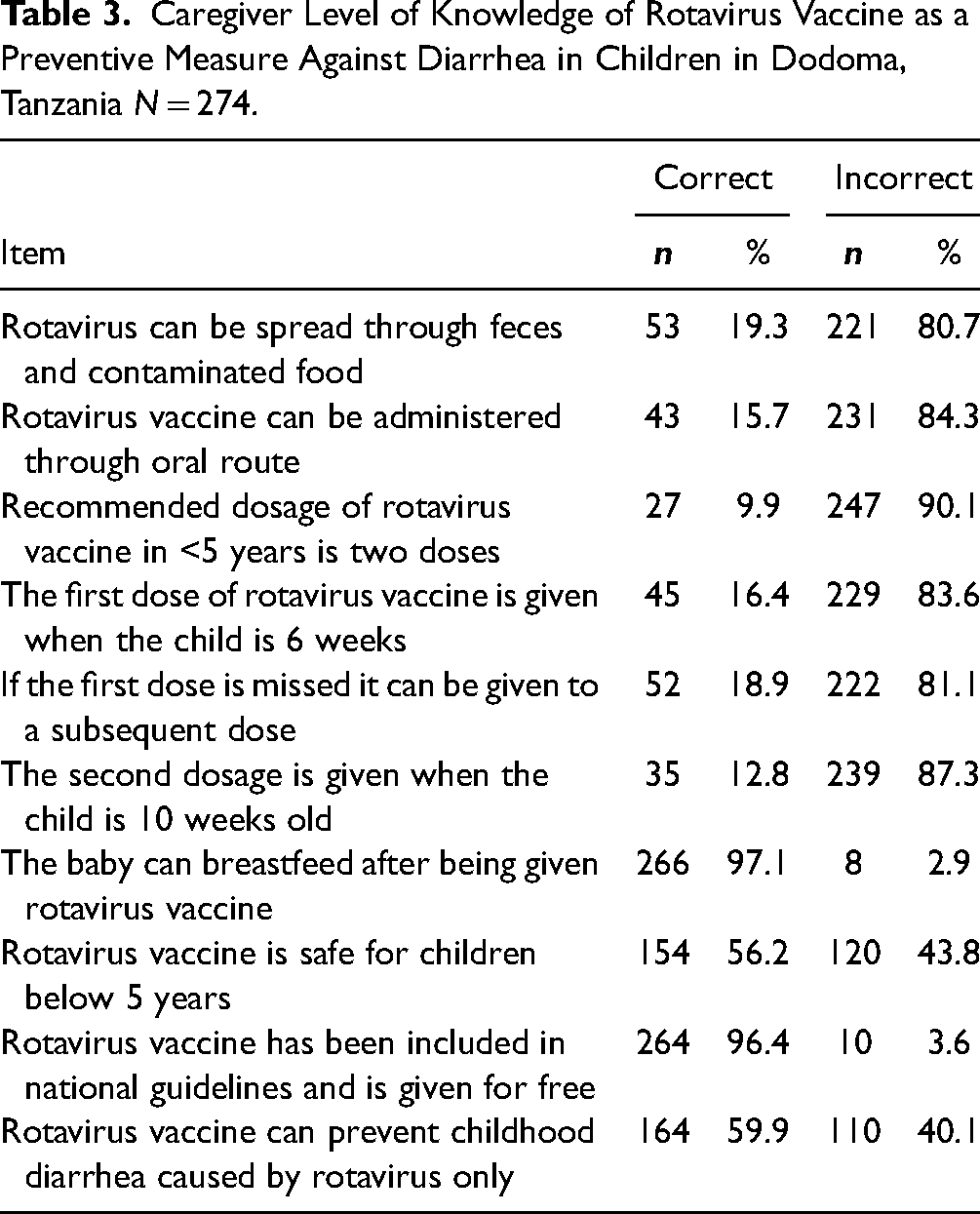
Caregiver's Level of Knowledge on Rotavirus Vaccine as One Among the Childhood Diarrhea Preventive Measures
The majority (n = 247, 90.1%) of caregivers of children under 5 years of age had never heard of the rotavirus vaccine. Their average overall knowledge level was 4.78 SD = 1.89, as shown in Table 3
Caregiver Level of Knowledge of Rotavirus Vaccine as a Preventive Measure Against Diarrhea in Children in Dodoma, Tanzania N = 274.
Factors Associated With the Caregiver's Level of Knowledge About General Childhood Diarrhea Prevention Measures and Rotavirus Vaccines. Multivariable Linear Regression Analysis
Regarding caregiver knowledge of general childhood diarrhea prevention measures, it was found that child growth in 1 month was associated with a 0.31 decrease in caregiver knowledge (β = −0.306, 95% CI) = −0.490, −0.122, p < .001). Furthermore, secondary education was associated with a 0.64 higher score than primary education (β = 0.641, 95% CI = 0.409–0.873, p < .001).
Regarding caregiver knowledge level about the rotavirus vaccine, it was found that a 1-month increase in child age was associated with a 0.64 decrease in caregiver knowledge level (β = −0.637, 95% CI = −0.893), −0.382, p < .001); As participants get older, their level of knowledge increases (β = 0.072, 95% CI = 0.10, 1.34, p = .022). Participants with secondary education had a 0.74 higher score than participants with primary education (β = 0.738, 95% CI = 0.427, 1.050, p < .001), while having a large number of children was associated with lower knowledge (β = −0.568), 95% CI = −1.035, −0.102, p = .017). Furthermore, being a male child was associated with 1.12 higher knowledge levels (β = 1.116, 95% CI = 0.712, 1.520, p < .001) (Table 4 and Table 5).
Multivariable Linear Regression of Factors Associated With Caregiver Knowledge of General Diarrhea Prevention Measures in Children in Dodoma, Tanzania N = 274.

Multivariable Linear Regression of Factors Associated With Caregiver's Level of Rotavirus Vaccine Knowledge in Dodoma, Tanzania N = 274.

Discussion
The aim of this study was to determine the knowledge of caregivers of children under 5 years of age on childhood diarrheal disease prevention strategies and associated factors in Dodoma, Tanzania. Regarding general diarrheal disease prevention measures, the study found that the average overall score of participants was 7.058, SD = 1.327. All 274 respondents (100%) were able to correctly define diarrhea. The results are similar (Joya et al., 2022; Workie et al., 2018). This can be explained by the fact that our study was conducted in an urban area where more than half of the participants had primary school education.
More than half of the mothers (57.3%) were aware that diarrhea in children can be caused mainly by poor hygiene practices, while unexpectedly, the majority of study participants (80.7%) were unaware of the specific common pathogens of diarrhea in children. This comes close (Joya et al., 2022; Omole et al., 2019). One justification for these results could be that the health education that parents receive in the child development clinic is not comprehensive enough.
Most participants were unaware of the signs and symptoms of dehydration (Mumtaz et al., 2014). However, all respondents (100%) were aware of the relevance of using ORS on a child with diarrhea (Chaudhary et al., 2014; Workie et al., 2018). On the other hand, our results contradict the observations of Joya et al. (2022). This may be due to differences in the understanding of health education provided on diarrhea in children. About 63% of caregivers knew that effective handwashing with soap was key to preventing diarrhea. All participants also knew that breastfeeding can also prevent diarrhea in children. The results are consistent with Joya et al. (2022) and Workie et al. (2018). This may be due to education about the importance of breastfeeding.
Most respondents (89.8%) did not know that it is not recommended to give antibiotics to a child with watery diarrhea before the results of laboratory tests. These results are contradictory to Padhy et al. (2017). The observed variation can be explained by the differences in literacy levels. Furthermore, similar to Chaudhary et al. (2014), Omole et al. (2019), and Padhy et al. (2017), 56.2% of respondents knew that diarrhea in children can have serious consequences if left untreated including stunted growth, developmental failure, and death. Regarding caregivers’ level of knowledge about the rotavirus vaccine as one of the measures to prevent diarrheal disease in children, the study found the following:
Although rotavirus vaccination is included in national guidelines for children under 5 years of age, only (9.9%) caregivers knew about rotavirus vaccination. Similar results were observed by Malik (2020). On the other hand, the results are contradictory to Napolitano et al. (2019) and Ahmed (2017). The reason for this discrepancy could be due to the difference in public health education and campaigning regarding vaccination of children under 5 years of age.
More than half of the study participants knew that a rotavirus vaccination can prevent diarrhea. The results are consistent with Joya et al. (2022). However, the majority of participants did not know the route of transmission of rotavirus. This is similar to what was found in Sudan by Ahmed (2017). One justification for these findings could be that the health education parents receive in the child development clinic is not comprehensive.
Our study found that the majority (90.1%) of participants did not know the recommended dosage of the rotavirus vaccine that can protect their child from diarrhea. This is consistent with Ahmed (2017). Additionally, the study found that two-thirds of study participants believed the rotavirus vaccine was dangerous for their children. This is similar to Ahmed (2017) but contradictory to Napolitano et al. (2019). The reason could be, in our facilities, the vaccine is included in the vaccination schedule and is provided free of charge, so parents would have sent their children for vaccination without noticing if they had also received a rotavirus vaccine.
An increase in the educational level of caregivers was also accompanied by an increase in their knowledge of general preventive measures against diarrheal diseases in children (Desta et al., 2017; Ogunrinde et al., 2012) and increased knowledge of rotavirus vaccines (Derso et al., 2020; Malik, 2020). This can be explained by the fact that as participants’ education level increases, their awareness of diarrhea increases, and therefore their knowledge about diarrhea increases.
This study found that as the child grew older by 1 month, caregivers’ knowledge of general diarrhea prevention measures and knowledge of rotavirus vaccines decreased. This can be explained by the fact that as the child grows older, the tendency of caregivers to visit a children's clinic decreases, resulting in lower participation in health education. The study suggests practical ways to maintain and improve parents’ knowledge as their children grow older, such as community outreach or using digital health platforms.
Increasing numbers of children have been found to reduce caregivers’ knowledge of rotavirus. This is in contrast to (Pratiwi & Kristina, 2020). One reason for this may be that, in our environment, the increase in the number of dependents leads to an increase in economic responsibility, which makes it less likely that parents will have time to find new information about vaccinating children
We also found that increasing the caregiver's age by 1 year increased knowledge about rotavirus vaccines. This can be explained by the fact that increasing age is usually associated with increasing exposure to children's health and therefore a higher level of knowledge.
Surprisingly, caregivers of female children had less knowledge than caregivers of male children. This may be related to the fact that diarrhea is more common in male children than in women (Elnadif & Abdalla, 2022), which is why mothers perceive the disease as more serious in boys and take precautionary measures. On the other hand, this could be because the early male circumcision awareness program is aimed more at mothers of boys, who may be more involved in health discussions about hygiene than mothers of girls. However, the study recommends further investigation of these results with a different design, preferably qualitative, to learn more from caregivers.
Strength and Limitation
The study included a sufficient sample size. However, because this was a cross-sectional design and hospital-based, the results cannot prove a causal relationship and the level of knowledge of the participants may differ from the general population as parents may have previously received health education about diarrhea.
Implication for Practice
The results highlight the great need to develop and implement public health education and awareness programs regarding the rotavirus vaccine, which in turn will increase awareness and knowledge and ultimately lead to significant prevention of diarrhea in children.
Conclusion and Recommendation
The study found a higher level of knowledge about general diarrheal disease prevention, but a low level of knowledge about the rotavirus vaccine. Therefore, there is a great need to develop and implement education and awareness programs on diarrhea in children. Furthermore, a future community-based study with a large sample size will help paint a true picture of caregivers’ knowledge of diarrhea in children.
Footnotes
Acknowledgments
The authors would like to thank the Administrative Secretary of Dodoma Region for permission to conduct this study. Many thanks also to Makole Health Center and mothers of under-five children for support during data collection.
Author Contributions
Conceptualization: NS and LSM. Methodology design: NS, LSM, PPM, and GMM. Data analysis: NS, LSM, PPM, and GMM. Writing of the original draft: LSM and PPM. Critical revision and writing of the draft review: GMM. Editing of the final draft of the manuscript and approval of it: NS, LSM, PPM, and GMM.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability of Data and Materials
The data used in this study are available from the corresponding author upon special request.
Ethical Approval and Consent to Participate
Ethical approval was obtained from the institution's research ethics committee with approval number MA.84/261/02/238. Approval to conduct the study was granted by the regional administrative secretary. Before data collection, participants were explained the benefits and potential risks of participating in the study and then signed the informed consent form. Participation was voluntary and confidentiality was strictly maintained throughout the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Use of AI software
The authors confirm that no artificial intelligence (AI) software was used in the creation of text, figures, or other information content in this manuscript.