
Abstract
Background
Breast milk provides infants with complete nutrition for immune development and protection against childhood diseases and associated mortality. Early initiation of breastfeeding (EIBF) aids in providing colostrum to newborns, providing protection against infection, and improving newborn and infant survival. Although Simiyu reported the lowest prevalence of EIBF in Tanzania, no study has investigated the factors associated with EIBF in this region.
Objective
The study aimed to determine early breastfeeding initiation prevalence and associated factors among women of reproductive age in the Simiyu region.
Methodology
We used data from a cross-sectional study conducted by AMREF Health Africa among 669 women of reproductive age (15–49 years) in the Simiyu region, Tanzania. An interviewer-administered questionnaire collected data on breastfeeding practices (including breastfeeding initiation) among others. A multilevel logistic regression analysis estimated the adjusted odds ratio (OR) and 95% confidence intervals (CI) for factors associated with EIBF.
Results
The mean age of 669 women analyzed was 28.3 years (SD ± 6.8). The prevalence of EIBF was 62.2%, ranging from 52.7% in Bariadi district to 73.3% in Maswa district. Lower odds of EIBF were among women who had a caesarian section (OR = 0.41; 95% CI = 0.17–0.98) and those who gave birth to male children (OR = 0.57; 95%CI = 0.39–0.82) while higher odds of EIBF were among mothers who reported skin-to-skin contact (OR = 2.40; 95%CI = 1.53–3.83) and from Maswa district (OR = 2.73; 95%CI = 1.09–6.89).
Conclusion
The prevalence of EIBF in the Simiyu region remains low (62%) relative to the global target of 70% by 2030 and varies by district. To promote EIBF in the region, good engagement and communication practices between mothers and healthcare providers should be emphasised in educating women about the importance of EIBF. Moreover, the practice of skin-to-skin contact between mother and child should be encouraged immediately after delivery.
Background
Breast milk provides complete nutrition to infants, is essential for immune development, and protects against childhood diseases (UNICEF, 2014). Lack of optimal breastfeeding is associated with long-term impacts, such as poor productivity due to compromised intellectual growth (Victora et al., 2016). About 166 million cases of diarrhoea and 9 million cases of pneumonia in children under 2 years can be avoided by optimal breastfeeding practices. Sub-optimal breastfeeding is attributed to 595 379 child deaths each year of which 56% occur in Sub-Saharan Africa (SSA) (Walters, Phan, et al., 2019). Optimal breastfeeding practices start from birth, hence delayed initiation of breastfeeding increases the risk of neonatal mortality. Infants who initiate breastfeeding between 2 and 23 h after birth have a 33% higher risk of death compared to those who initiate within 1 h, and the risk increases even more for those breastfed more than 24 h after birth (Smith et al., 2017).
Globally, in 2017, only 42% of newborns initiated breastfeeding within 1 h of delivery (UNICEF and WHO, 2018). In SSA, the prevalence of early initiation of breastfeeding (EIBF) was 58.3%, ranging from 24% in Chad to 86% in Burundi (Gebretsadik et al., 2020; Hailemariam et al., 2015; Ogbo et al., 2015; Walters, Phan, et al., 2019). In Tanzania, the prevalence of EIBF is 51% varying between 26% in the Simiyu region and 80% in the Tanga region (MoHCDGEC et al., 2016). The national estimate and that of the Simiyu region are below the global targets of EIBF rates of 70% by 2030 (WHO and UNICEF, 2019). Further studies in Tanzania show a variation of EIBF practice ranging from 51% in Morogoro to 83.1% in the Kilimanjaro region (Bruyn et al., 2018; Exavery et al., 2015; Kiwango et al., 2020; Lyellu et al., 2020; Smith et al., 2017). Community, maternal social-demographic, newborn, and reproductive and health services factors play a role in influencing EIBF and other breastfeeding practices (Mukora-Mutseyekwa et al., 2019; Nkoka et al., 2019; Teshale & Tesema, 2021).
The government of Tanzania implemented several national strategies for infant and young child feeding and nutritional interventions (MoHCDGEC et al., 2013) to promote optimal breastfeeding practices and achieve the national breastfeeding targets by 2025, such as a 65% coverage of EIBF (MoHCDGEC et al., 2021). Despite these efforts, reports indicate low EIBF practice, where Simiyu had the lowest prevalence (26%) than other regions (MoHCDGEC et al., 2016). Differences in health services coverage and population dynamics across the country may explain variations in EIBF practice across regions. Although Simiyu had the lowest prevalence of EIBF in Tanzania, no study documented the factors that influence EIBF in this region. Given this context, it is vital to identify determinants of EIBF among mothers in different parts of the country, especially in areas with low practice to help inform appropriate context-specific interventions. The study aimed to determine the prevalence of EIBF and associated factors among mothers with children less than 2 years old in the Simiyu Region lake zone in Tanzania.
Literature Review
EIBF practices vary globally across countries. Across the WHO European countries, the prevalence of EIBF ranged from 5% in Bulgaria to 84% in Kyrgyzstan (Bagci Bosi et al., 2016). In SSA, the prevalence of EIBF was 58.3%, ranging from 24% in Chad to 86% in Burundi (Tashale and Tesema, 2021). Several studies conducted in different parts of Africa have further reported the prevalence of EIBF ranging from 38% in Nigeria to 83.1% in rural parts of western Ethiopia (Gebretsadik et al., 2020; Hailemariam et al., 2015; Ogbo et al., 2015; Walters, Phan, et al. 2019). The reasons for the variation of EIBF across African countries include differences in cultural practices (Hailemariam et al., 2015), socio-economic status, and differences in health services coverage (Ogbo et al., 2015; Raihana et al., 2021). There are also variations of EIBF practices across studies in Tanzania, the lowest prevalence (26%) was reported in the Simiyu region, and the highest (83.1%) in the Kilimanjaro region (Ali et al., 2020; Exavery et al., 2015; MoHCDGEC et al., 2016). However, less is known about the reasons for the low prevalence of EIBF particularly in the Simiyu region.
Globally, factors influencing EIBF differ between and within countries due to differences in cultural, socio-economic, and demographic conditions, and health systems challenges. Studies in Africa reported several factors that increase the likelihood of EIBF including exposure to mass media, health facility delivery, vaginal delivery, skin-to-skin contact, higher socio-economic status, and having a formal education whether primary or secondary (Mukora-Mutseyekwa et al., 2019; Patel et al., 2015; Teshale & Tesema, 2021). Also, young mothers aged 15–19 years are less likely to practice EIBF than their older counterparts (Ogbo et al., 2015; Teshale & Tesema, 2021; Walters, Phan, et al. 2019). In Ethiopia and Malawi, mothers with singleton births, colostrum feeding, and being a housewife positively influenced EIBF (Hailemariam et al., 2015; Nkoka et al., 2019). Nevertheless, further investigations on formal or informal maternal employment on optimal breastfeeding practices are critical to inform policy decisions. Factors such as cesarean delivery, parity, delivering a male child, prelacteal feeding, failure to place the baby on the mother's chest after delivery affected EIBF negatively (Patel et al., 2015; Walters, Phan, et al. 2019).
In Tanzania, several studies have found that vaginal delivery, primary education level, multiparity, good knowledge of timely initiation of breastfeeding prelacteal feeding, and health facility delivery increased the likelihood of EIBF (Ali et al., 2020; Cooper et al., 2019; Exavery et al., 2015; Kiwango et al., 2020; Lyellu et al., 2020). A lower number of antenatal care (ANC) visits (less than four visits), lack of postnatal follow-up, a missed counseling opportunity on child nutrition during delivery, and poor knowledge of the importance of colostrum feeding delayed the initiation of breastfeeding (Gebretsadik et al., 2020; Lyellu et al., 2020; Weldesamuel et al., 2018). Despite the identification of these factors in some parts of the country, EIBF is still low (MoHCDGEC et al., 2016). More effort to identify context-specific determinants in different settings, especially with a low prevalence of EIBF like the Simiyu region will help in designing targeted interventions to address the existing gaps and promoting optimal breastfeeding practices.
Research Questions
We aimed to answer the following research question: What is the prevalence of EIBF and associated factors among women of reproductive age with children aged less than 2 years in the Simiyu Region, Tanzania? Specifically, the study answers the following questions:
What is the prevalence of EIBF among women of reproductive age with children aged less than 2 years in the Simiyu region, Tanzania? What are the factors associated with EIBF among women of reproductive age with children aged less than 2 years in the Simiyu region, Tanzania?
Methods
Study Design and Setting
We conducted a secondary analysis of data from a cross-sectional study in the Simiyu region from May 20 to June 03, 2021 by Amref Health Africa in Tanzania. The population of the Simiyu region according to the 2021 projection is approximately 2,418,495 with an annual growth rate of 5.0 (National Bureau of Statistics and Ministry Of Finance And Economic Affairs, 2021). Agriculture is the most dominant economic activity in the region. Other economic activities include fishing, trade, and commerce. The region has reported excessively worse situations for maternal and child health services coverage like postnatal check-ups (10%), facility delivery (40%), and newborns who received postnatal check-ups within two days (15%). Moreover, among children under 5 years, 33.3% and 5% are reported to be stunted and wasted, respectively, and only 15% of children were exclusively breastfed in the region (MoHCDGEC et al., 2016).
Study Population and Sampling
A multi-stage cluster sampling was used to select study participants. In the first stage, enumeration areas (EAs) in the Simiyu region from the 2012 Tanzania population and housing census were used as the sampling frame. A random number of 51 clusters were selected for inclusion out of 67 clusters. From sampled clusters, the enumeration of all households and their residents was carried out by trained enumerators and mappers from the National Bureau of Statistics (NBS). In the second stage, households were randomly selected from each cluster yielding a total 2035 of households. All women and men aged 15–49 residing within the selected households and provided informed consent were interviewed. A total of 2020 women were interviewed. This study included women of reproductive age (15–49 years) who gave birth 2 years preceding the survey. Out of the 2020 women, we included 754 who gave birth below 2 years before the survey, among them, 72 who never breastfed their children were excluded, and 13 with missing information on EIBF. We, therefore, analyzed data for 669 women (Figure 1).
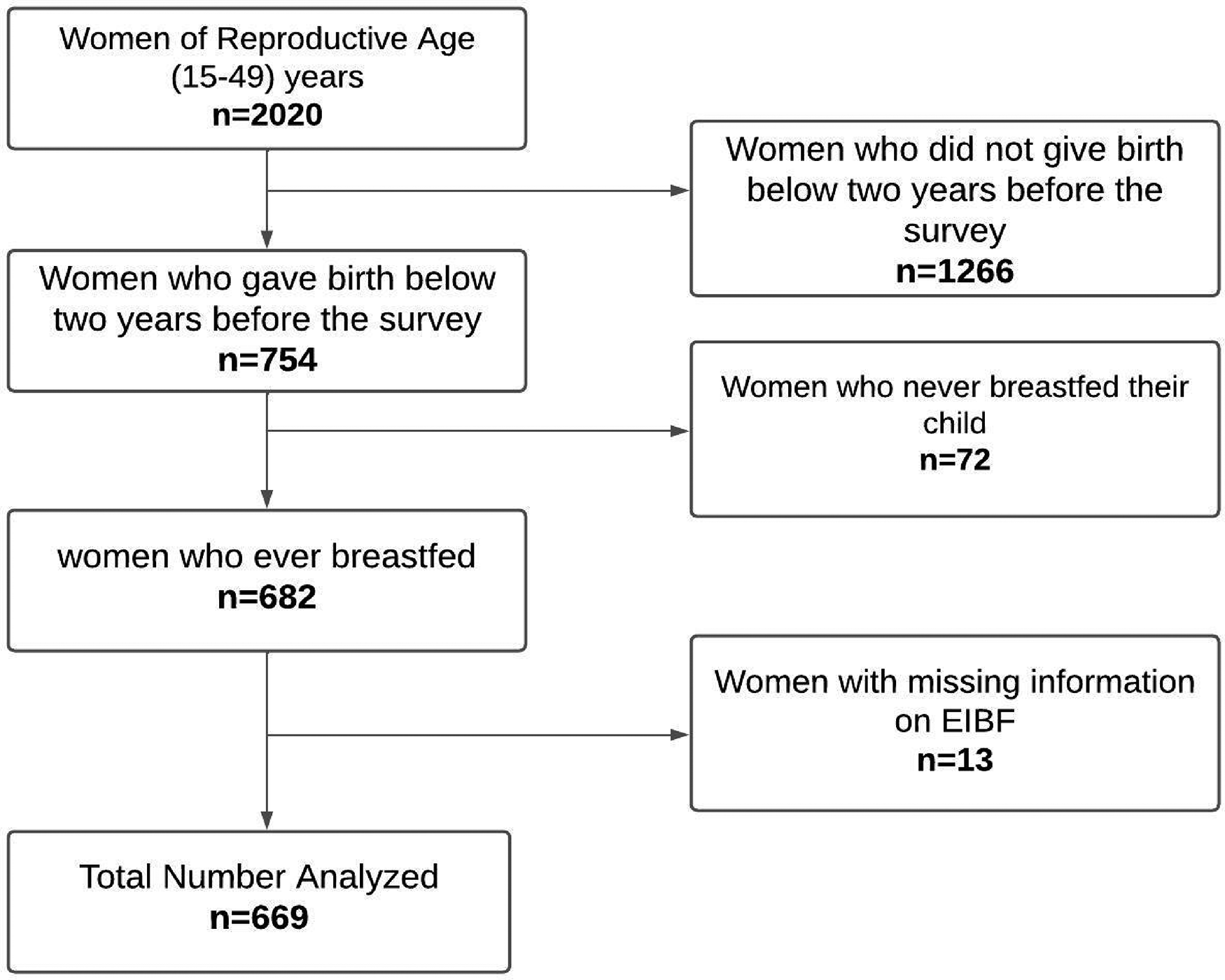
Flow chart showing the number of women of reproductive age analysed.
Data Collection Methods and Tools
An interviewer-administered questionnaire used for data collection was developed based on questions from the 2015/2016 Tanzania Demographic and Health Survey (TDHS). The questionnaires, developed in the English language, were translated into Swahili and installed on an Android tablet using Open Data Kit (ODK) for data collection. The questionnaire captured information on pregnancy, deliveries, post-delivery care, family planning, sexual activities/behaviours, decision making on various issues such as healthcare utilization and management of household income, and breastfeeding practices including EIBF. Trained research assistants collected the data. The head of the household provided permission to interview all eligible women available in the household, while informed consent was obtained from all eligible individuals.
Study Variables
The dependent variable was EIBF defined as the initiation of breastfeeding within 1 h after delivery (Ali et al., 2020; Exavery et al., 2015; Kiwango et al., 2020; WHO and UNICEF, 2019); classified as “1” if a woman initiated breastfeeding within 1 h and “0” if otherwise.
Independent variables included maternal and child demographic characteristics and reproductive and maternal health services. Maternal demographic characteristics included maternal age (15–19, 20–24, 25–29, and 30 + years), education level (non-formal education, primary, secondary,), marital status (single, married, cohabiting, divorced/ widowed), maternal employment (employed, not employed), and district of residence (Bariadi, Itimila, Busega, Maswa, Meatu). Child characteristics include the child's sex (male, female) and the child's age (<6, 6–12, 13–17, and 18–2 months). Reproductive and maternal health services included the number of antenatal visits (<4, 4 visits and more), place of delivery (health facility, home/others), mode of delivery (vaginal, cesarean section), placing of the baby on mother's chest/abdomen after delivery (skin to skin contact) (yes, no), level of health facility of delivery (health centre, dispensary, hospital), birth attendant (health professionals, traditional birth, and friend/relative/ others).
Data Management and Analysis
We used STATA software version 15 (StataCorp LLC, NY, USA) for data cleaning and analysis. Continuous variables were summarized using mean and standard deviation, while categorical variables were summarized using frequencies and percentages. Differences in the proportion of EIBF between groups of independent variables were determined using the Chi-squared test at a two-sided 5% threshold level. Since the study used data collected by a cluster sampling technique, the observations are dependent at several hierarchical levels, thus using a classical logistic regression may not be appropriate in analysing this data (Sheffel et al., 2019). Therefore, a multilevel logistic regression analysis model was used. To determine whether multilevel regression was required for the data set, a null model (a model without exposure variables) was first fitted. The intra-class correlation (ICC), a measure of the degree of variability between clusters (Irimata & Wilson, 2018), was used to determine whether there was a significant cluster difference.
Moreover, two models were fitted: model 1 was a two-level random effects model with clusters (EAs) as level 2. Model 2 was a three-level model with households as level 2 and clusters (EAs) as level 3. In model 2, the ICC indicated that there was no significant difference between the households. There was a significant cluster difference/variation, whereby, 27.6% of the total variation of EIBF was due to cluster difference. As a result, the log odds of EIBF were best modelled using model 1; a two-level logistic regression model with the following equation.

A bivariate analysis was performed to identify variables that are associated with EIBF. Variables with p-value < .10 in the bivariate analysis and those identified in the literature as potential confounders were considered for multivariable analysis. Akaike Information Criteria together with the ROC analysis/curve were used in model selection. In multivariable multilevel logistic regression analysis, variables with a p-value ≤ .05 were considered statistically significant.
Results
EIBF Proportion by Participant Background Characteristics
A total of 669 women of reproductive age (15–49 years) were analysed, with a mean age of 28.29 years (SD ± 6.8). Of all women in this study, 184 (27.5%) were aged 20–24 years. The majority of them 526 (79.7%) were married, 458 (68.5%) had primary education, over half, 392 (58.6%) were employed, and 336 (50.3%) gave birth to a male child (Table 1).
EIBF by Background Characteristics of Study Participants (n = 669).

Frequency does not tally to 669 due to missing values in marital status.
The prevalence of EIBF was 62.2%. The prevalence of EIBF differed significantly by resident district, mother's age, and child's sex. Maswa district had the highest prevalence of EIBF 73.3% (95% CI = 66.5–79.1) and the lowest being in Bariadi district 52.7% (95% CI = 44.1–61.1). Among women aged 25–29 years 72.8% (95% CI = 65.7, 78.9) initiated breastfeeding within 1 h. Furthermore, 67.5% (95% CI = 62.2–72.3) of female children were initiated to breastfeeding within 1 h (Table 1).
EIBF by Reproductive and Maternal Health Characteristics of Study Participants
Among 669 women analysed, 426 (66.2%) attended 4 or more ANC visits during the last pregnancy, 546 (81.6%) of women were delivered by a health professional birth attendant, virginal delivery was reported among 637 (95.2%) women, placing of the baby on mother's chest/abdomen after delivery was reported among 452 (97.8%) women. A total of 539 (80.6%) women delivered in the health facility, and for those who deliver at health facilities 378 (70%) women delivered in dispensaries (Table 2).
EIBF by Reproductive and Maternal Health Characteristics of Study Participants (n = 669).

Frequency does not tally to 669 due to missing values in these variables.
EIBF prevalence differed significantly by place of delivery, with 64.4% (95% CI = 60.2, 68.3) of women who delivered at a health facility practised EIBF. EIBF was also reported to be 67.2% (95% CI = 65.3–73.8) among women whose babies were placed on their chest/abdomen after delivery. Furthermore, 62.7% (95%CI = 62.3–71.8) and 62% (95%CI = 50.4–69.2) of women who delivered in the dispensary and hospitals initiated breastfeeding within 1 h, respectively (Table 2).
Factors Associated With EIBF
In the bivariate analysis, women who had a caesarian delivery had 59% less likelihood of EIBF than those who had a virgin delivery (COR = 0.41; 95%CI = 0.20–1.04). When compared to female children, women who had male children had 0.62 (95%CI = 0.45–0.92) times lower odds of EIBF. In addition, mothers who reported placing the baby on their chest/abdomen after delivery (skin-to-skin contact) had twice the odds of EIBF compared to their counterparts (COR = 2.40; 95%CI = 1.53–3.83). Furthermore, compared to the women from Bariadi district, women from Maswa district had 2.73 times higher odds of EIBF (COR = 2.73; 95%CI = 1.09–6.89) (Table 3).
Factors Associated With EIBF.

Results from the multivariable multilevel logistic regression model showed that women who had a caesarian delivery had a 59% less likelihood of EIBF than those who had a virginal delivery (AOR = 0.41; 95% CI = 0.17–0.98). Women who delivered a male child had 0.57 (95%CI = 0.39–0.82) times lower odds of EIBF. Mothers who had their babies placed on their chest/abdomen after delivery had twice the odds of EIBF compared to their counterparts (AOR = 2.40; 95%CI = 1.53–3.83). Furthermore, compared to women from Bariadi district, women from Maswa district had 2.73 times higher odds of EIBF (AOR = 2.73; 95%CI = 1.09–6.89) (Table 3).
Discussion
The prevalence of EIBF in this study is slightly lower than the national EIBF target of 65% by 2025 (MoHCDGEC et al., 2021) though higher than the TDHS 2015/16 national estimate and that from Simiyu (MoHCDGEC et al., 2016) and Morogoro regions (Exavery et al., 2015). However, the prevalence is lower than what was observed in the northern part of the country (Ali et al., 2020; Kiwango et al., 2020; Lyellu et al., 2020). This can be explained by an increase in ANC attendance and health facility delivery from that reported in 2016 to what was observed in the current study among women in the Simiyu region over time (MoHCDGEC et al., 2016). ANC visits and health facility delivery provide an opportunity for health professionals to inform and assist mothers in the process of achieving timely breastfeeding initiation and improved EIBF knowledge and practices (Lyellu et al., 2020). The prevalence reported in Chad and Nigeria (Ogbo et al., 2015; Teshale & Tesema, 2021) was also lower. However, the observed prevalence differs slightly from that observed in Northeast Ethiopia (Gebretsadik et al., 2020) but is lower than those in Burundi, Malawi, and West Ethiopia (Hailemariam et al., 2015; Teshale & Tesema, 2021; Walters, Phan, et al. 2019). As a result, progress in EIBF can be promoted with good interaction and communication between mothers and healthcare providers.
Placing of the baby on the mother's chest/abdomen after delivery (skin-to-skin contact) was significantly associated with higher EIBF likelihood. Early mother-to-baby contact after birth develops a baby-to-mother bond, which has various benefits. One of these benefits is the improvement of nutritional behaviours. When skin-to-skin contact is maintained for at least 1 h, it stimulates digestion and the baby's interest in feeding. Newborns instinctively move towards the breast (“breast crawl”), resulting in the baby suckling on the mother's breasts. This ensures that breastfeeding begins immediately after the baby is born. Consistent findings are reported in previous studies from low- and middle-income countries (Ephrem & Tsegaye, 2020; Mukora-Mutseyekwa et al., 2019; Patel et al., 2015). In the absence of complications for either the mother or the child during delivery, the practice of skin-to-skin contact between mother and child should be encouraged immediately after delivery and uninterrupted for 1 h or until the first feed.
This study found that women who had caesarean section had a lower chance of EIBF than those who had virginal deliveries. A possible explanation is that mothers who had caesarean section deliveries required extensive post-operative care. During this time, the child is under the care of a paediatrician while the mother recovers from conditions such as general anaesthesia effect, pain, and fatigue, which in turn, delays the breastfeeding initiation (Lyellu et al., 2020; Ogbo et al., 2015; Teshale & Tesema, 2021). This finding is consistent with what has been reported elsewhere in Tanzania (Exavery et al., 2015; Lyellu et al., 2020) and across other settings in SSA (Adewuyi et al., 2017; Mukora-Mutseyekwa et al., 2019; Ogbo et al., 2015; Teshale & Tesema, 2021; Walters, Phan, et al. 2019).
As also reported elsewhere (Ezeh et al., 2019a; Teshale & Tesema, 2021), male children had lower odds of EIBF. This gender disparity in EIBF may be explained by cultural issues regarding male children in some African cultures. For instance, colostrum feeding is not encouraged in some African societies for male children, and male children are more likely than female children to receive prelacteal feeding (Berde & Ozcebe, 2017). However, given that the majority of women reported giving birth in a health facility, the influence of EIBF by cultural issues regarding male children may also indicate missed opportunities among healthcare providers to emphasise and assist women on EIBF. To emphasise equal EIBF among all newborns, regardless of sex in the Simiyu region, more effort among healthcare providers on assisting, educating, and emphasising EIBF should be provided to women at ANC, during delivery and community at large.
We also observed variations in EIBF between districts in Simiyu where mothers from Maswa had higher odds of EIBF than those from Bariadi district. These disparities may be due to regional differences in maternal and child health care coverage and services. Moreover, when compared to other districts, Maswa district had the highest proportion of women who are more educated (secondary education). Secondary or higher education has an impact on increased awareness and knowledge of EIBF, resulting in higher EIBF practices. Geographic variations in EIBF prevalence have also been reported in other settings in Tanzania (Ali et al., 2020; Exavery et al., 2015; MoHCDGEC et al., 2016) and SSA (Ezeh et al., 2019a; Mukora-Mutseyekwa et al., 2019).
Study Strengths and Limitations
One strength of the study is the inclusion of all of the districts in the Simiyu region, hence results can be generalised to all women of reproductive age (15–49 years) in the region. However, the study has limitations. Firstly, because we used secondary data, variables like parity, child weight, multiple births, and gestational age at delivery were not captured, but they have been linked to EIBF in other studies (Ali et al., 2020; Ezeh et al., 2019b; Mukora-Mutseyekwa et al., 2019; Teshale & Tesema, 2021), hence the results may be affected by residual/unmeasured confounding. Furthermore, EIBF was self-reported by mothers, hence the potential for recall bias since multiple events occur concurrently during delivery, whereby the exact time for breastfeeding initiation may be incorrectly reported, leading to an overestimation of the prevalence of EIBF.
Implications for Practice
A caesarean section delivery was observed to lower the odds of EIB. As recommended by the WHO, caesarean sections should be performed only when necessary. This will reduce the number of caesarean sections and thus the delayed initiation of breastfeeding. Furthermore, greater emphasis should be placed on the implementation of interventions aimed at improving EIBF, particularly among caesarean delivery women. Moreover, in the absence of complications for either the mother or the child during delivery, the practice of skin-to-skin contact between mother and child should be encouraged immediately after delivery. Healthcare providers should put more effort into assisting, educating, and emphasising EIBF without child sex discrimination among women attending ANC, during delivery, and the community at large.
Conclusion
The prevalence of EIBF in the Simiyu region is still low (62%) compared to the global target of 70% by 2030 and varies by district. To improve EIBF in the region, good interaction and communication practices between mothers and healthcare providers should be emphasized in educating women about the importance of EIBF regardless of the child's sex. Moreover, the practice of skin-to-skin contact between mother and child should be encouraged immediately after delivery.
Footnotes
List of Abbreviation
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.