
Abstract
Introduction
Chronic heart failure (HF) is a global health issue, with telemonitoring emerging as a key strategy for elderly patient management, aligning with the Universal Health Care Law.
Objective
To assess the impact of telemonitoring on the quality of life, hospitalization rate, and mortality rate among elderly patients with chronic HF.
Methods
A rapid review of 11 studies, including randomized controlled trials, quasi-experimental, prospective, and retrospective studies from 2013 to 2023, was performed using CINAHL. The studies encompassed 14,993 elderly patients with chronic HF from hospital and homecare settings.
Results
The impact of telemonitoring on quality of life, hospitalization, readmission, and mortality among elderly patients with chronic HF varies widely across studies. Three studies reported quality of life improvements in the intervention group, one showed no significant change, and most studies revealed no difference in all-cause hospitalizations and readmissions between intervention and control groups. Mortality rate comparisons also showed no significant differences.
Discussion
The studies, conducted between 2013 and 2020 primarily in high-income regions, highlight telemonitoring's growing role in managing chronic heart failure (CHF) among elderly patients, yet its global applicability remains limited by a lack of research from Asia and Africa. While telemonitoring systems showed promise in improving patient adherence, engagement, and potentially reducing mortality, their effectiveness on quality of life, hospitalization, and readmission rates is inconsistent, likely influenced by variability in system design and patient characteristics. Limitations such as reliance on a single database, a small number of studies, and underrepresentation of mortality data further constrain the generalizability and conclusiveness of the findings.
Conclusion
Telemonitoring is a complex, yet promising tool for elderly CHF patient management. To enhance care quality and fulfill universal healthcare goals, policymakers and healthcare practitioners should consider these insights to create precise, effective telemonitoring strategies.
Introduction
Chronic heart failure (HF) poses a substantial global health burden that necessitates innovative approaches to elevate disease management (Sapna et al., 2023). Traditional models of care often fall short of addressing the needs of the elderly (aged 60 and above) with chronic HF, largely due to barriers in accessing care, frequent hospitalizations, and the challenges involved in managing multiple chronic conditions (Husson et al., 2014; McNabney et al., 2022). Telemonitoring emerged as a revolutionary tool in managing chronic HF, offering a blend of technology and health that promises improved patient outcomes and healthcare efficiency (Silva-Cardoso et al., 2021).
Telemonitoring in managing chronic HF involves using remote monitoring technologies to track patient's health status and provide timely interventions. Its core lies in its ability to remotely monitor vital health parameters, such as heart rate, blood pressure, and weight (Ghilencea et al., 2022). Real-time monitoring enables early detection of any changes that may signal a worsening condition, allowing healthcare providers to respond promptly (Nguyen et al., 2024) and potentially reduce hospitalizations (Salma et al., 2024). Additional features on patient education and engagement empower patients with the knowledge and tools necessary to actively engage in self-management, fostering sustainable behavioral changes and improved outcomes (Li et al., 2021). Medication management is another feature that promotes patient adherence as well as allows healthcare providers to make timely adjustments based on real-time data (Eggerth et al., 2020). Telemonitoring bridges the gap between clinical care and patient autonomy by providing continuous support and individualized feedback, making it a promising tool to effectively manage chronic HF especially in highly vulnerable populations such as elderly patients.
Telemonitoring in managing chronic HF has led to better patient outcomes, such as improvement in the quality of life. Patients are able to develop a sense of security and empowerment, making them feel that they are in control of their health, which contributes to improved quality of life (Dinesen et al., 2022; Fatrin et al., 2022). Long-term telemonitoring has also been associated with fewer hospitalizations (Fatrin et al., 2022; Urbich et al., 2020) and reduction in mortality rates (Matta et al., 2022), underscoring its potential to revolutionize the management of chronic HF and provide significant, life-saving interventions.
Despite the growing adoption of telemonitoring in the Philippines as part of government telehealth initiatives, significant gaps remain that hinder its effective implementation, particularly in rural areas. Technological barriers, such as limited access to technological devices (e.g., smartphones) and unreliable internet connectivity, pose a major barrier since telemonitoring requires the use of mobile devices and strongly relies on reliable data transmission and storage systems (Aranki et al., 2016; Ferrari et al., 2022; Macariola et al., 2021). Telemonitoring devices, such as the implantable pulmonary arterial pressure monitoring systems, are already available but their use is limited by regulatory approvals (Iellamo et al., 2020). Cultural acceptance and educational disparities exacerbate the challenges associated with adopting telemonitoring since the public, including healthcare providers, may be reluctant to transition to virtual monitoring due to a lack of familiarity and training (Alvarez et al., 2021). Lastly, the geographical structure of the Philippine archipelago and the significant workflow modifications and resource allocations required for the integration of telemonitoring into existing healthcare systems also pose infrastructural challenges (Barradas et al., 2024).
Several studies have investigated the effectiveness of telemonitoring in managing chronic HF among elderly patients. It is therefore timely to determine the results of these studies to inform policymakers advocating its integration into the healthcare system. Furthermore, while government initiatives and private sector efforts have accelerated the adoption of telemonitoring, partly in response to the COVID-19 pandemic, there remains a pressing need for robust policy development to ensure sustainability, standardization, and inclusivity in telemonitoring practices (Ferrari et al., 2022; Ruyobeza et al., 2022; Stoumpos et al., 2023).
Objective
In support of the development of policies aligned with the Philippines’ Universal Health Care Law and facilitating its effective integration into the healthcare system, this rapid review of literature aims to determine the impact of telemonitoring on the quality of life, hospitalization rate, and mortality rate among elderly patients with chronic HF.
Methods
A rapid review is a type of research synthesis method that aims to provide a quick and streamlined assessment of existing literature on a specific topic, typically with a shorter timeline compared to traditional systematic reviews (King et al., 2022). Rapid reviews are often conducted in response to time-sensitive policy, clinical, or research questions and are designed to provide evidence-based answers in a more timely fashion (Smela et al., 2023).
The need for rapid reviews arises in situations where there is a pressing need for evidence-based information, and traditional systematic reviews may take several months or even years to complete due to their comprehensive and rigorous nature (Garritty et al., 2021). Rapid reviews are conducted with the goal of balancing the need for speed with maintaining a certain level of methodological rigor (Tricco et al., 2022).
The primary review question was the following: “Among elderly patients with chronic heart failure, how effective is the use of telemonitoring as compared to usual care in disease management?” The secondary review questions were as follows: (1) “What is the impact of telemonitoring on quality of life among elderly patients with chronic HF?,” (2) “How does telemonitoring affect the overall rate of hospitalizations of elderly patients with chronic HF?,” and (3) “How does telemonitoring lower the incidence of mortality among elderly patients with chronic HF?”
The rapid review method used was parallel to Dobbins’ (2017) five-step process (Figure 1). The search focused on the criteria set by the researchers, which include (1) English and English translated, (2) full-text peer-reviewed articles from January 2013 to December 2023, (3) was conducted through randomized controlled trial, quasi-experimental, retrospective, and cohort studies, and participants ages 60 years old and above, and (4) there should be a comparison to standard or usual care. These criteria were chosen to ensure that the study captures high-quality, up-to-date evidence on telemonitoring's effectiveness and applicability in managing chronic HF among elderly patients. The selected methodologies and focus on peer-reviewed studies also help to ensure that the findings are reliable and applicable to real-world healthcare settings. The researchers used initial search terms consisting of “chronic heart failure,” “telehealth,” “usual care,” and “disease management.” Other search terms included “geriatric” for elderly, “telemonitoring” and “nurse-led telehealth” for telehealth, “face to face intervention” for standard care, and “disease control” and “self-management” for disease management. The Boolean operator “AND” was used to narrow down the search for similar or alternative words or phrases. Due to limited time, the researchers used CINAHL as the search engine since it is tailored specifically to nursing and allied health literature making it an excellent and comprehensive resource for finding relevant studies for rapid review, housing approximately 3,800 active indexed and abstracted journals from which 3,416 are active peer-reviewed journals.

Dobbins’ five-step process of rapid review.
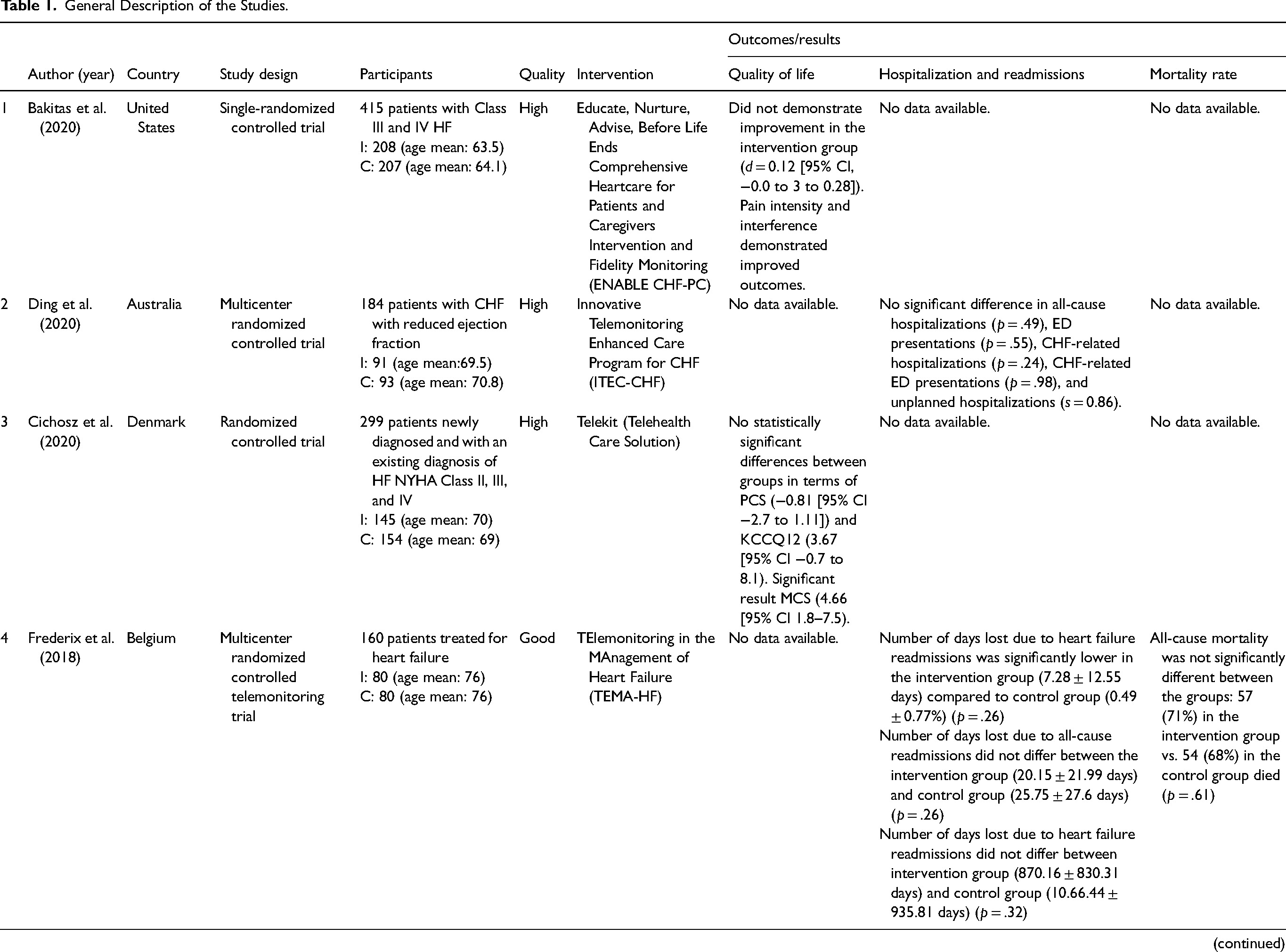
The research team began the initial search in November 2023 and identified a total of 54 records. Researchers KLA and CRP removed 37 studies from the initial research due to duplication of records. Researchers LR and LH reviewed and screened the remaining articles (n = 17). After record screening, the articles were trimmed down to 16 (n = 1, not usual care as comparison). The Johns Hopkins Research Evidence-Based Appraisal Tool (Appendix E) was utilized for external review of the remaining 16 articles. Three external reviewers, who are experts in the study methodology, helped ensure the quality, objectivity, and reliability of the articles, providing impartial perspective, increasing the rigor and trustworthiness of the final report. Five articles (n = 5) were removed due to ineligibility. Finally, 11 articles were included in the rapid reviews (see Figure 2). Relevant data were extracted and presented through structured tables, including author, country, study design, participants, quality rating, the type of telemonitoring system used under interventions and the outcomes and main study results relevant to quality of life, hospitalization and readmission, and mortality rate (see Table 1).

PRISMA flow diagram: identification, screening, and selection of articles included in the rapid review.
General Description of the Studies.
Discussion
General Characteristics of the Literatures
The screening process yielded 11 articles, which were reviewed and evaluated for their quality and relevance. The studies were conducted in Australia (n = 1), the United States (n = 5), and Europe (n = 5) and were published between 2013 and 2020. Of the 11 studies, 8 (73%) studies were randomized controlled trials, 2 (18%) studies were retrospective studies, and 1 (9%) study was prospective quasi-experimental. The mean age of the participants in the 11 studies was 65.7 years old (65.6 for the intervention group and 65.7 for the control group). Each study used a different type of telemonitoring system and was conducted in 6 (54.5%) hospitals and 5 (45.5%) home settings. A detailed presentation of the studies is found in Table 1.
Types of Telemonitoring Systems
Diverse telemonitoring systems have been utilized in the management of chronic HF, each with distinct approaches and goals. In-person comprehensive consultations with palliative care clinicians, telehealth nurse coaching sessions centered on critical palliative care topics, and monthly follow-up calls to evaluate patient needs and reinforce previously learned material are all components of Bakitas et al.’s (2020) ENABLE CHF-PC (Educate, Nurture, Advise, Before Life Ends Comprehensive Heartcare for Patients and Caregivers) Intervention and Fidelity Monitoring. ITEC-CHF or Innovative Telemonitoring Enhanced Care Program for chronic HF combines remote body weight monitoring, structured telephone support, nurse-led collaborative care, and standardized patient education materials to give patients more control, identify early deterioration, maintain consistent care, and utilize a team-based approach in managing chronic HF (Ding et al., 2020). In the telemonitoring program using Telekit (Telehealth Care Solution), participants were given an electronic scale to weigh themselves and a device to answer symptom-related questions (Cichosz et al., 2020). Daily measurements were transmitted to a secure site and automatically examined, with alarms generated as needed. Nurses then contact patients to validate their information and make necessary referrals.
The Telemonitoring in the Management of Heart Failure, also known as TEMA-HF by Frederix et al. (2019), combined nurse-led collaborative care with structured telephone support and remote body weight monitoring to manage chronic HF. Motiva Telemonitoring Systems, created by Phillips Healthcare, integrate instructional materials, medication prompts, health questionnaires, and motivating communications to assist those with chronic ailments such as HF (Koulaouzidis et al., 2019). It aims to improve patient outcomes by utilizing individualized and proactive remote monitoring and support to boost patient involvement, medication adherence, and overall health management. The Tel-Assurance Monitoring System developed by Pharos Innovations entails conducting toll-free calls on a daily basis for a duration of 6 months (Jayaram et al., 2017). During these conversations, patients are prompted to answer automated questions regarding their symptoms and record their daily weight. This technology allows for the remote monitoring of patients’ health status, enabling the early diagnosis of possible difficulties and for proactive management. Ultimately, it enhances patient participation and improves results in chronic illnesses such as HF.
The MedSentry Medication Monitoring System utilizes electronic devices that are remotely monitored to notify patients when it is time to take their meds (Hale et al., 2016). A surveillance facility staffed with counselors reaches out to participants and caregivers in the event of noncompliance with medication instructions. The Remote Monitoring System (RMS) provides notifications and responses between the patient and the healthcare provider when essential indicators (such as weight, blood pressure, and heart rate) surpass predetermined thresholds, guaranteeing prompt intervention for patients with chronic ailments such as HF (Evangelista et al., 2015). Nurses utilize teleconferencing sessions to engage in collaborative discussions with primary care providers, facilitating a synchronized strategy to fulfill patient requirements and enhance the distant provision of care, thereby enhancing patient outcomes. Influence of home monitoring on mortality and morbidity in HF patients with impaired left ventricular function, also known as IN-TIME Telemonitoring (Hindricks et al., 2014), is a remote monitoring system that provides patients with implant-based multiparameter telemonitoring via Biotronik Home Monitoring. The technology identifies tachyarrhythmias and sends information to a monitoring center for proper treatment.
The Health Buddy electronic device used by Gingele et al. (2019) provides extensive assistance to patients with chronic diseases through the provision of education, guidance for self-care, and daily monitoring of symptoms. It enables patients to properly manage their health while allowing healthcare experts to swiftly respond if symptoms require further research or advice. This proactive strategy fosters patient involvement, encourages self-control, and enhances overall results in the management of chronic diseases. Although not specified, the telemonitoring system in Madigan et al.’s (2013) study measures daily vital signs such as blood pressure, pulse, oxygen saturation, and weight. It is implemented after hospitalization. Each Home Health Care (HHC) agency's central monitoring station receives this data via the patient’s phone line. With this configuration, ongoing remote monitoring, early health status changes detection, and prompt interventions to aid in patient recuperation and enhance posthospitalization results are all made possible.
Quality of Life
The various studies examined the impact of telemonitoring on the quality of life for elderly patients experiencing chronic HF. Bakitas et al. (2020) observed no overall improvement in quality of life, although there was a positive effect on pain intensity and interference. Cichosz et al. (2020) reported no significant changes in the physical aspects of quality of life but found a notable improvement in mental well-being. In contrast, Hale et al. (2016) found that the intervention group actually experienced a decline in quality of life. Conversely, Jayaram et al. (2017) and Madigan et al. (2013) both documented improvements in quality of life among their intervention groups. Evangelista et al. (2015) added to the positive findings by reporting enhancements in physical, emotional, and overall quality of life scores for their intervention group.
Overall Rate of Hospitalizations
The data on hospitalization and readmissions in elderly patients diagnosed with chronic HF across the different studies provided its importance to the creation of guidelines for such intervention. Ding et al. (2020) found no significant difference in all-cause hospitalizations or emergency department presentations, suggesting that their telemonitoring intervention did not impact these metrics. Similarly, Frederix et al. (2019) reported a significant reduction in the number of days lost to HF readmissions in the intervention group, yet this did not extend to all-cause readmissions. Koulaouzidis et al. (2019) observed no difference in the overall rate of hospitalizations, though the intervention group spent fewer days in the hospital. Gingele et al. (2019) noted that while the time to first HF-related admission did not change, the intervention group had significantly fewer such admissions overall. In contrast, Hale et al. (2016) reported a significant decrease in all-cause hospitalizations, indicating a strong positive effect of their intervention.
Mortality Rate
In the examination of mortality rates among elderly patients with chronic HF subjected to telemonitoring intervention, the data from select studies revealed a range of outcomes. Notably, the majority of studies provided no information on mortality rates, leaving a gap in the collective understanding of intervention impacts in this critical area. However, of those that did, Frederix et al. (2019) and Gingele et al. (2019) reported no significant difference in all-cause mortality between intervention and control groups, indicating that the interventions in these particular studies did not alter the mortality rate. On a more positive note, Koulaouzidis et al. (2019) found a significant decrease in all-cause mortality among the intervention group, suggesting a potential benefit of their specific telemonitoring system. Similarly, Hindricks et al. (2014) documented a lower 1-year all-cause mortality rate in the intervention group, lending support to the idea that certain interventions could improve survival outcomes.
The studies span a period from 2013 to 2020 and have been conducted across diverse regions that include Australia, the United States, and Europe. This reflects that telemonitoring has been increasingly accepted as part of the management of chronic HF among elderly patients. However, the lack of studies from Asian and African regions underscores a significant gap, limiting its applicability and acceptability on a global scale. Apparently, most of the studies, being randomized controlled trials (73%), lend robustness to the data, with retrospective and prospective quasi-experimental studies providing additional perspectives.
Telemonitoring systems demonstrate significant variability, with each system utilizing a distinct approach to customized patient needs and healthcare goals. These systems range from remote monitoring of vitals and symptoms to advanced platforms that incorporate complex actions encompassing patient education, individualized nurse coaching, and medication reminders. Such variety highlights the flexibility and adaptive characteristics of telemonitoring, allowing it to encompass a broad range of patient care dimensions, which increases patient adherence to treatment regimens, leading to a reduction of clinical mortality (Gupta, 2023). By addressing both clinical and behavioral aspects of health, the diversity of these systems establishes the multifaceted nature of telemonitoring—from promoting patient engagement to increasing the efficiency of healthcare providers in the delivery of individualized healthcare.
The impact of telemonitoring on the quality of life for elderly patients varies widely across studies. Such varied results suggest that telemonitoring's impact on quality of life is not uniformly positive among elderly patients and may depend on specific interventions or treatment plans. Moreover, the distinction between mental and physical aspects of quality of life is crucial, as some interventions may be more effective in addressing psychological well-being rather than physical symptoms (Paddon & Kampman, 2023). Nonetheless, telemonitoring platforms provide personalized treatment advice and self-management tools, empowering their users to better manage their conditions, thereby effectively contributing to improved quality of life.
The findings on hospitalization and readmissions among elderly patients with chronic HF are diverse. Although some studies, such as Hale et al. (2016), demonstrated a substantial decrease in all-cause hospitalizations, others demonstrated more specific or limited effects. For instance, Frederix et al. (2019) and Gingele et al. (2019) reported decreases in readmissions, including decreased number of hospital days during hospitalizations; however, these effects did not consistently extend to all-cause readmissions or duration of first admission. In contrast, Ding et al. (2020) and Koulauzidis et al. (2019) did not observe any substantial differences in the overall hospitalization rates. The inconsistent results across different telemonitoring platforms suggest that the effectiveness of telemonitoring in reducing hospitalization and readmissions remains poorly established.
The analysis of mortality rates associated with the utilization of telemonitoring among elderly patients in the management of chronic HF is difficult to generalize due to critical gaps in literature since most studies did not include them. However, some of the studies found a decrease in mortality rates (Hindricks et al., 2014; Koulaouzidis et al., 2019), suggesting that some telemonitoring systems have the potential to increase survival outcomes. In contrast, Frederix et al. (2019) and Gingele et al. (2019) reported no significant difference, signifying that telemonitoring did not directly affect survival outcomes. These disparate findings highlight the complexity of addressing mortality in chronic HF patients and suggest that while some interventions may hold promise, the overall effectiveness of telemonitoring on mortality rates is not conclusively demonstrated.
Limitation of the Study
The study has several limitations that could influence the interpretation of its findings. It relied solely on the CINAHL database, which may have limited the scope of studies included by potentially missing relevant research from other sources like PubMed. Time constraints of the rapid review process may have also restricted the depth of the literature search. With only 11 studies analyzed, the generalizability of the findings might be limited, as a larger sample could provide more robust evidence. Additionally, the included studies utilized diverse telemonitoring systems, introducing variability that complicates drawing uniform conclusions. Mixed results regarding telemonitoring's impact on quality of life suggest that effectiveness may depend on intervention design and patient characteristics. Furthermore, many studies did not report on mortality rates, creating gaps in understanding telemonitoring's effect on survival outcomes. Most of the studies were conducted in high-income countries, which could limit the applicability of the findings to lower-income settings.
Implications for Practice
The analysis of these results underscores the complexity and variability in the effectiveness of telemonitoring systems for CHF management. The varied impact on quality of life, hospital readmission rates, and mortality rates suggests that telemonitoring's efficacy is not uniform and is likely influenced by numerous factors including the specific nature of the intervention, patient characteristics, and healthcare settings.
Future research should focus on identifying which elements of telemonitoring are most beneficial, for whom, and under what circumstances. Additionally, more studies are needed to fill in the data gaps, particularly regarding mortality rates. There is also a clear need for personalized approaches in telemonitoring, as the diverse needs and responses of patients to different interventions become evident. Furthermore, the overall effectiveness remains variable and indicates a need for further research to identify the most efficacious approaches.
Conclusion
In conclusion, the studies provide valuable insights into the use of telemonitoring for elderly patients with chronic HF, highlighting both its potential benefits and limitations. This rapid review provided little but significant information regarding the use of telemonitoring in healthcare practice, which can be useful in policymaking. Policymakers and healthcare practitioners can use these findings to develop more targeted, effective, and patient-centered telemonitoring strategies that align with broader healthcare goals and ensure equitable and quality care for all.
Footnotes
Acknowledgments
We thank the anonymous reviewers for their constructive feedback, which helped improve the manuscript.
Author Contributions
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.