
Abstract
Introduction
Preeclampsia is a pregnancy-specific hypertensive disease that affects 3–5% of pregnant women all over the world and 1.3% of pregnancies among Jordanian women.
Objectives
This study aims to assess the cardiovascular disease risk factors awareness among women with a recent history of preeclampsia in Jordan and assess the role of healthcare providers in providing counseling about cardiovascular disease risk factors.
Methods
A descriptive cross-sectional design was used to recruit 180 women with a recent history of preeclampsia during the last 12 months. Data were obtained from patients’ medical records and the Attitude and Beliefs about Cardiovascular Disease Risk Questionnaires.
Results
The results revealed that 43.9% of women with a recent history of preeclampsia have hypertension, 6.7% have diabetes mellitus, 16.1% have dyslipidemia, 28.9% have a family history of cardiovascular disease, 66.1% are overweight or obese, and 7.2% are smokers. The mean total score of knowledge subscale was 5.5 (SD = 1.21) out of 8. Only 20% of the participants had good cardiovascular disease knowledge. The mean total score of risk perception was 15.47 (SD = 7.8). The mean score of perceived benefits and intention to change behaviors was 2.30 (SD = 0.62). The mean score of healthy eating intentions was 2.54 (SD = 0.81). Income, having diabetes mellitus, and receiving counseling about preeclampsia as cardiovascular disease risk factor were associated with some dimensions of cardiovascular disease risk factors awareness.
Conclusion
The prevalence of cardiovascular disease risk factors was relatively high among the study participants. The majority of participants had inadequate cardiovascular disease knowledge. In addition, the role of healthcare providers in providing counseling about cardiovascular disease and related risk factors, including PE was limited. Providing more counseling related to cardiovascular disease by nurses and doctors is essential to enhance women's cardiovascular disease knowledge and intention to change lifestyle.
Introduction
Preeclampsia (PE) is a vascular pregnancy-specific hypertensive disease that was linked to an approximately 75% greater risk of cardiovascular disease (CVD)-related mortality (Grandi et al., 2019). Since 2011, the American Heart Association and the American Stroke Association have included PE as a risk factor for CVD with other risk factors such as hypertension, obesity, dyslipidemia, and smoking. In addition, they recommended treating women with a PE history along with other CVD risk factors (Mosca et al., 2011).
PE increases the sodium sensitivity of blood pressure, endothelial dysfunction, and metabolic changes as the insensitivity of insulin and lipid profile, which encourages the development of CVDs (Appelman et al., 2015). Additionally, PE accelerates the development of CVD events, usually arising at an earlier age as compared to women with normotensive pregnancy. Myocardial infarction, stroke, hypertension, and type 2 diabetes mellitus (DM) occur 8–10 years earlier in women with a history of PE (Sandvik et al., 2013). So, women with a history of PE are at future risk of early CVD; hence, screening for cardiovascular risk factors and avoidance strategies should be taught to these young women until effective therapies are found (Paauw et al., 2016).
Prevention and early detection of cardiovascular risk factors is the primary goal of the treatment. It also provides an opportunity to modify risk through healthy lifestyle behavior implementation and routine screening (Maabreh et al., 2023). Knowledge of the association between PE and future CVD would maximize the effect of preventive lifestyle or medical interventions (Traylor et al., 2016). On the other hand, many internists and obstetrician–gynecologists have inadequate knowledge related to the association between PE and CVD later in life, which may decrease the attention to PE as a risk factor in the clinical area (Young et al., 2012).
Literature Review
CVD remains the leading cause of death among women worldwide (Kandasamy & Anand, 2018). In the USA, one woman dies every 80 s from CVD (Benjamin et al., 2018). Some behavioral risk factors such as high-risk diet, tobacco, alcohol use, and physical inactivity can contribute to blood pressure elevation, blood lipid level elevation, blood glucose elevation, overweight, and obesity (World Health Organization, 2019). The burden of CVD is growing faster than the ability to combat it due to the increased prevalence of significant risk factors for heart disease and stroke, including unhealthy diet, obesity, blood pressure elevation, and diabetes (Dunbar et al., 2018). Understanding the association between PE and increased risk for future CVD development is important for building awareness and decreasing the CVD risk among women (Skurnik et al., 2016). Few studies were conducted to assess patients’ awareness of CVD and PE, showing an inadequate understanding of the association between PE and future CVD (Reeder, 2017; Skurnik et al., 2016; Spratling et al., 2014). In Jordan, Khader et al. (2018) assessed CVD risk factors among women with a history of PE. However, the current study is among novel studies that assess the CVD risk factors awareness and the role of HCPs in providing counseling about CVD among women with a recent history of PE.
Purpose
This study aimed to assess the CVD risk factors awareness among women with a recent history of PE in Jordan and assess the role of HCPs in providing counseling about CVD risk factors.
Methods
Design
A descriptive, cross-sectional study was conducted with a convenience sample of 180 women with a recent history of PE.
Sample
The target population was women with a recent history of PE. The accessible population included women with a recent history of PE in Al-Basheer hospital and Princess Badeea obstetrics and gynecology hospital. A convenience sampling technique was used to recruit the study participants. The inclusion criteria included women who were of childbearing age (between 15 and 45 years) and delivered and experienced PE during the last 12 months. The exclusion criteria include women with a history of CVDs before pregnancy. A total of 236 women with a recent history of PE were approached to participate in the study from the two hospitals. Of these, 56 women were not interested in participating. Therefore, the response rate was 76.6%.
Data Collection Instrument
Data were collected using a two parts questionnaire. The first part included questions that the researcher filled out after reviewing the patient health record about whether they received health education about CVD (if the patients received counseling about their CVD future risk, what they received, and when they received the counseling). The second part was a self-reported questionnaire composed of 20 questions about demographic characteristics and health history questions.
In addition, the self-reported questionnaire comprised the Attitude and Beliefs about Cardiovascular Disease (ABCD) risk questionnaire, which was developed by Woringer et al., (2017) to evaluate patients’ awareness of CVD risk. The questionnaire consists of four subscales: knowledge of CVD risk and prevention, perceived risk of heart attack/stroke, perceived benefits, intention to change, and healthy eating intentions. The questionnaire has internal consistency reliability of Cronbach's α = 0.85 for Perceived Risk, and 0.82 for Perceived Benefits and Intention to Change Behavior. Healthy Eating Intentions has Cronbach's α = 0.60 which is below 0.70 but acceptable for a three-item scale and may be used in assessing patients’ awareness of CVD risk as mentioned by the author who developed this tool (Woringer et al., 2017).
Permission was obtained from the tool developer to translate the English version of the tool to Arabic. The questionnaire was translated into Arabic and back-translated into English by two native Arabic-speaking experts who were fluent in English. Then, the Arabic version was compared with the original English version by a third translator. After clarifying some ambiguities and inconsistencies, the consensual Arabic version was sent to an expert panel for final review of all translation reports until consensus was achieved. The content validity index was high and the final version was tested among 30 Jordanian women who showed an understanding of all items. Consistent with the original tool, the final Arabic version consisted of four subscales. The Knowledge subscale (eight items) was scored as 1 for correct answers and 0 for incorrect or “I don’t know” answers. The total score can range from 0 to 8, with higher scores indicate more knowledge. The other subscales include “perceived risk of heart attack/stroke” (eight items), “perceived benefits and intention to change behavior” (seven items), and “healthy eating intentions” (three items). These subscales are rated on a 5-point scale rated as the following: 1 = strongly disagree; 2 = disagree; 3 = agree; 4 = strongly agree; and N/A = 0.
Data Collection Procedure
Ethical approval was obtained before conducting the study. After that, the principal investigator met the directors of the target hospitals and explained the purpose of the study and the data collection procedure. Then, the researchers accessed the potential participants, obtained their approval to participate, reviewed their health records to fill out the first part, and provided them with the self-reported questionnaire. The study was conducted following ethical conduct and protecting the patient’s rights.
Statistical Analysis
The data were analyzed using the Statistical Package of Social Science (SPSS) version (23). The significance level was set at P < 0.05. Descriptive statistics were used to describe the study sample. As per the author's guidelines for scoring the ABCD risk questionnaire (Woringer et al., 2017), the sum score of the Knowledge subscale was calculated, with a higher sum score indicating higher knowledge. Due to lack of specific guidelines by the tool developer to identify what constitutes good knowledge, knowledge scores were rescaled to 100, and the mean percent score was reported. Then, we used Bloom's cutoff to categorize knowledge scores as good for women with a percentage score of more than 80% (Bloom et al., 1956). The other subscales were scored and interpreted as per author guidelines: Perceived Risk (higher sum score indicates higher risk perception), Perceived Benefits and Intentions to Change (higher average score indicates higher perceived benefits and readiness for change), and Healthy Eating Intentions (higher average score indicate higher perceived readiness for change). Descriptive statistics were also used to describe the role of HCPs in providing counseling about CVD risk factors. Lastly, the relationships between demographic variables of participants and the four subscales of CVD risk factors awareness were assessed with multiple linear regressions.
Results
Sample Characteristics
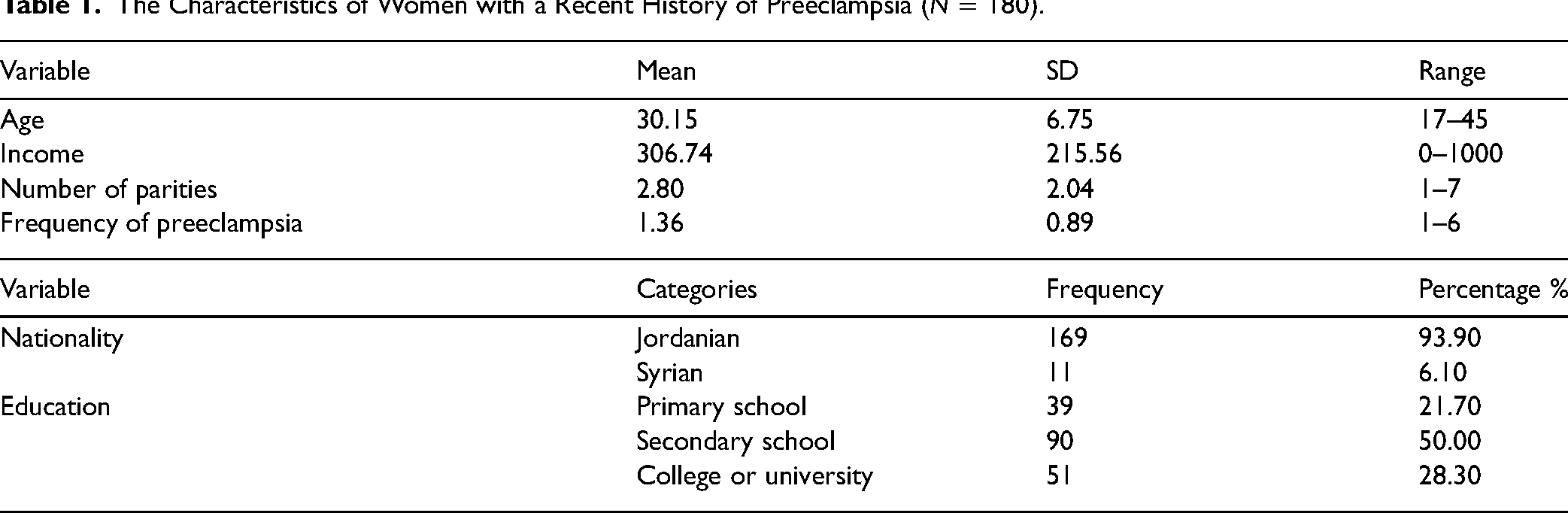
The mean age of the women respondents was 30.15 (SD = 6.75), ranging from 17 to 45 years. Most participants were Jordanians (n = 169, 93.9%), while only 11(6.1%) were Syrian. The mean monthly income of the participants was 306.74 Jordanian Dinars (JD) (SD = 215.56). Regarding educational level, the majority completed secondary school (50%, n = 90), followed by the college or university (28.3%, n = 51), and, lastly, primary school (21.7%, n = 39). The mean number of parities was 2.80 (SD = 2.04, ranges 1–7), while the mean frequency of PE was 1.36 (SD = 0.89, ranges 1–6), Table 1.
The Characteristics of Women with a Recent History of Preeclampsia (N = 180).
CVD Risk Factors among the Study Participants
Table 2 presents the frequencies and percentages of different CVD risk factors among the study participants. About 7.2% of the participants are current smokers, 43.9% had hypertension, 6.7% had DM, 16.1% had dyslipidemia, 28.9% had a family history of CVDs, and 14.4% had a family history of PE, and about two-thirds had a BMI of 25 or more.
Cardiovascular Disease Risk Factors among Women with a Recent History of Preeclampsia (N = 180).

BMI = body mass index; CVD = cardiovascular disease; DM = diabetes mellitus.
CVD Risk Factors Awareness among the Study Participants
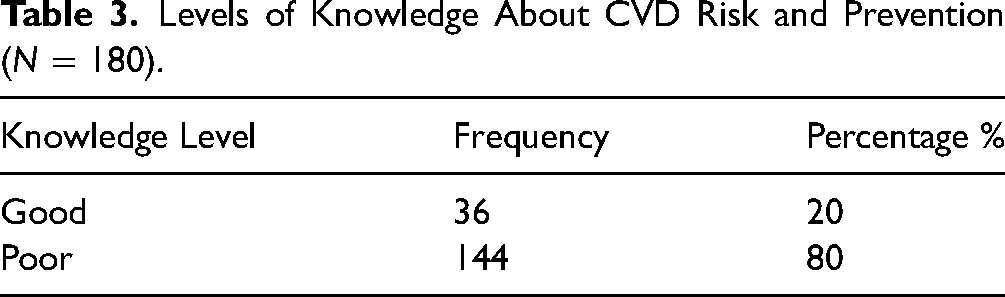
The mean total score of the knowledge subscale was 5.5 (SD = 1.21) out of 8. Only 20% of participants had good CVD knowledge (Table 3). The mean total score of risk perception was 15.47 (SD = 7.8) out of 32. The mean score of perceived benefits and intention to change behaviors was 2.30 (SD = 0.62) out of 4. The mean score of healthy eating intentions was 2.54 (SD = 0.81) out of 4.
Levels of Knowledge About CVD Risk and Prevention (N = 180).
The Role of HCPs in Providing Counseling About the CVD Risk Factors, Including PE
After a thorough observation of the medical records and inpatient and outpatient files, no documentation of any health education about CVD risk factors was noted by physicians or nurses. However, some patients mentioned that they received education related to CVD risk factors and PE. Most frequently the counseling was provided by obstetricians (n = 41, 22.8%) followed by midwives and nurses (n = 7, 3.9%, each) and lastly by a cardiologist (n = 1, 0.6%). A description of the delivered counseling is presented in Table 4.
The Role of HCPs in Providing Counseling About the CVD Risk Factors Including Preeclampsia for Women with a Recent History of Preeclampsia (N = 180).

CVD = cardiovascular disease.
Factors Associated with CVD Risk Awareness
Multiple linear regression was used to assess the relationship of age, income, nationality, receive counseling about CVD, dyslipidemia, hypertension, diabetes, and smoking with the scores of the four subscales of CVD risk factors awareness. As shown in Table 5, income had a significant negative relationship with the knowledge subscale (β = −.185, t = −2.017, P = .046). Being diagnosed with DM was associated with an increased risk of CVD (β = .214, t = 2.423, P = .017). Finally, receiving counseling about PE as CVD risk factor was associated with increased scores of perceived benefits and intention to change behaviors (β = .231, t = 2.708, P = .008).
Factors Associated with Cardiovascular Disease Risk Factors Awareness.

CVD = cardiovascular disease; DM = diabetes mellitus.
Discussion
Risk factors of CVDs are serious threats to women's health conditions; the burden of CVD is now growing according to the dramatic rise of significant risk factors, including smoking, DM, obesity, and Hypertension (HTN) (Dunbar et al., 2018). In the current study, the reported prevalence of these factors is similar to or higher than those reported in previous studies (Khader et al., 2018; Okour et al., 2019). These findings could be due to unhealthy habits such as smoking, being too sedentary, having an unhealthy diet, not getting enough sleep, or having erratic sleep patterns, in addition to the family history risk factor.
The current study showed that 43.9% of women were diagnosed with HTN, as reported by the study participants, while other previous studies reported that 4.9% of women with a history of PE were complaining of HTN (Khader et al., 2018). Regarding family history, 28.9% of our participants had a family history of CVD; this percent was less than what was reported in a previous similar study that was conducted in the UK (Traylor et al., 2016). These results support that PE shared many risk factors, including hypertension and a family history of CVD.
Only 20% of participants had good CVD knowledge. This outcome is in line with the study of Hassen et al. (2022) which reported that 36.5% of women in Antwerp and 21.2% of women in Nottingham had good CVD knowledge, respectively.
The results indicated that the mean total score of risk perception was lower than the midpoint value of the total score of the original scale. This outcome indicates that most women did not recognize that there is a link between PE and CVD. This result is congruent with several previous studies (Brown et al., 2013; Hoedjes et al., 2012; Seely et al., 2013; Skurnik et al., 2016; Traylor et al., 2016) where women did not identify the link between PE and CVD risk. This result emphasizes the necessity for practical education to increase awareness about CVD as one of the major risk factors for PE; this awareness may play a significant role in early recognition of the risk factors and lead to early implementation of primary prevention.
The results also indicated that the mean score of perceived benefits and intention to change behaviors was lower than the midpoint value of the mean score of the original scale. This result is inconsistent with a previous research by Brown et al. (2013), which reported the vast majority of women believed that regular exercise will decrease the CVD risk. In the same line, Spratling et al. (2014) and Traylor et al. (2016) reported that most women identified smoking habits as factors that increase the CVD risk. In a Dutch study, the vast majority of women reported that they intended to adopt a healthy lifestyle (Hoedjes et al., 2012). Once women knew the link, they expressed their interest in learning more about it and their intention to improve their lifestyle (Skurnik et al., 2016). This emphasizes the necessity for implementing education to increase awareness of women about the role of regular exercise and smoking cessation to reduce the chance of having heart attack or stroke in the future. In 2017, 26% of women believed that they were at risk of having a heart attack, while after the educational intervention, the percentage increased to reach 41% (Reeder, 2017).
In the same line, our study result is similar to that of Traylor et al. (2016), which indicated that the participants also were less likely to recognize their risk of cardiovascular morbidities, including heart attack and stroke later in life. These results concluded that women's awareness of CVD risk factors would increase their perceived risk of heart attack/stroke, perceived benefits, and intention to change behaviors. Besides, women with a history of PE with no family history of CVD did not perceive themselves as being at risk for future CVD even though they had risk factors, while those with a PE and CVD family history believed that they were more vulnerable to cardiovascular problems (Brown et al., 2013). These results clarify that all mothers without traditional risk factors need to be taken into account that PE is an independent factor for future CVD.
In our study, a thorough reviewing of the medical records and patients’ files, no documentation of any counseling about CVD risk factors was performed by HCPs. The limited role was noted even in self-reported data by patients in the questionnaire, which could be due to work overload and limited time. Several studies have reported a similar finding, For instance, a study conducted in the USA showed that most women did not receive education about CVD risk factors, or the consequences of PE (Seely et al., 2013; Skurnik et al., 2016).
A US study indicated that 95% of internists and 70% of OB-GYNs provide routine counseling for cardiovascular risk reduction. However, a high proportion of them was unaware of the link between PE and CVD later in life and related that only 9% of internists and 38% of OB-GYNs were providing counseling for cardiovascular risk reduction among women with a history of PE (Young et al., 2012).
The American College of Obstetricians and Gynaecologists (ACOG) (2013) recognized knowledge gaps that, if addressed, will represent an opportunity to provide CVD preventive care among women who experienced PE by primary HCPs (Young et al., 2012). Twenty-eight percent of internists and 14.8% of gynecologists would not obtain a pregnancy history when assessing a history of a patient for cardiovascular health (Wilkins-Haug et al., 2015). In Ontario, just half of the HCPs (family physicians, obstetricians, and midwives) identified that PE increases the risk of future CVD which pointed out a knowledge deficit and communication gap among HCPs (MacDonald et al., 2007). For this, most women expressed that the HCPs were not aware of the link between PT and CVD later in life (Skurnik et al., 2016).
The knowledge deficiency of the link between PE and future CVD may limit the application in the clinical area. So, the ACOG in 2015 recommended that internists will need ongoing education to involve pregnancy history and specifically PE as a CVD risk factor. Obstetricians–gynecologists need education about follow-up screening for women with a history of PE and a life-course approach for integrating pregnancy complications into the clinical area leading to CVD prevention (Wilkins-Haug et al., 2015).
Women's age was not correlated with knowledge, perceived risk perception, benefit, and intention subscales. This outcome is in line with the previous studies that showed no relationship between mother’s age, knowledge, perception, or awareness of CVD and the related risk factors (Reeder, 2017; Seely et al., 2013; Skurnik et al., 2016; Spratling et al., 2014).
Regarding women's educational level, our study reported no significant difference in CVD risk factors awareness based on educational level. This result matches the other previous studies (Eshah et al., 2021; Reeder, 2017; Seely et al., 2013; Skurnik et al., 2016; Spratling et al., 2014). It is also incongruent with Okour et al. (2019) study, which showed the lacked awareness of CVD in educated women. Moreover, our result showed that women's income was negatively correlated to women's awareness level, which is converse to the result of Okour et al. (2019). A suggested strategy should be developed to enhance knowledge about healthy lifestyle behaviors in the general population.
In the same line, the current study revealed that women who received counseling about CVD and related risk factors had higher mean scores of perceived benefits and intention to change behaviors, such as exercise, weight, healthy diet, and smoking than those who didn’t receive counseling. This result is inconsistent with a study by Spratling et al. (2014) and Reeder (2017), which reported a significantly increased knowledge level of cardiovascular modifiable risk factors among women with a history of PE. This result concluded that counseling about CVD risk factors is more likely to increase the mothers’ awareness level compared to mothers who never received any counseling.
Limitations
The current study has some limitations. Data were collected from two public hospitals in Jordan, which limits the generalizability of the results. Also, using a self-reported questionnaire could pose a response set bias in answering the questions.
Study Implications
The current study has important implications for nursing practice, research, and education. Initially, it emphasizes the need to inform nurses about evidence of CVD risk among women with PE. This can be accomplished by giving lectures and workshops for nurses in hospitals and nursing students in universities. Afterward, these nurses will be able to do individualized assessments of women using appropriate risk assessment tools, followed by education on risk-reduction behaviors of modifiable risk factors to decrease as possible the risk of future CVD.
This study might be considered a cornerstone for future research. More research studies, especially using qualitative design, are needed to understand the dimensions of CVD problems among patients with PE. Further, interventional studies that assess the impact of education programs or risk reduction interventions on awareness levels and incidence of CVD are needed among these women.
Conclusion
Various conventional risk factors were prevalent among women, while hypertension and obesity were the highest prevalence risk factors. The majority of participants had inadequate CVD knowledge. On the one hand, the percentage of women with a history of PE who were aware of the link between PE and increased risk of CVDs later in life was high. Nurses should be supported to provide more education according to intention for healthy eating, perceived benefits to change their lifestyles, especially smoking, and the perceived risk of future heart attack/stroke.
According to the findings, once the participant was a smoker or aware of this link through healthcare providers’ counseling, the perceived benefits and perceived intent to change their lifestyle increased significantly. Notably, the role of HCP turned out to be limited among women in providing counseling to their increased risk of future CVD, as evidenced by the lack of documentation regarding providing counseling in participants’ medical charts and their self-reported responses. Providing more counseling related to CVD by nurses and doctors is essential to enhance women's CVD knowledge and intention to change lifestyle. Ultimately, steps should be taken to activate the HCP role in this “window of opportunity” in women's life to initiate preventive therapies as they are young.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.