
Abstract
Background
Paracetamol is a commonly used analgesic among older adults. There have been reports of adverse events with chronic paracetamol use even at therapeutic doses. The objective of this clinical audit is twofold – 1. To evaluate the prevalence of inappropriate paracetamol prescription in the elderly admitted for falls; 2. To introduce strategies to reduce the rate of inappropriate paracetamol prescription in this population.
Methods
A clinical audit was performed on 100 patients aged 75 years and older who were admitted to the Geriatric Medicine department of a tertiary hospital between July 2019 and October 2019 with a primary diagnosis of a fall. Data collected included demographic data, relevant medical history of cirrhosis, cognitive impairment, alcohol use and weight <50 kg, prescription pattern of paracetamol on day 1 or two of admission and on discharge as well as clinical data on the documented indications for paracetamol use.
Results
Paracetamol was prescribed in 84 patients. Out of these 84 patients, 56 were prescribed round-the-clock paracetamol with a median duration of 9 (IQR = 10) days. In this group, paracetamol use was inappropriate in 32 (57%) of them and 32 (57%) patients were discharged with round-the-clock paracetamol for a median duration of 17.5 (IQR = 46) days.
Conclusion
This clinical audit revealed a high prevalence of round-the-clock and inappropriate paracetamol prescription in elderly patients admitted for a fall. Moving forward, we hope that the implementation of a paracetamol prescribing algorithm may reduce the rates of inappropriate paracetamol prescribing in this population.
Introduction
Paracetamol is a commonly used analgesic in older adults. 1 Prior studies report paracetamol use in approximately 90% of older adults at an average dose of 3–4g per day. 1 Even when prescribed at therapeutic doses, paracetamol use has been associated with acute liver injury and acute liver failure. 2 There have also been reports of metabolic acidosis due to the accumulation of endogenous organic pyroglutamate as well as analgesia-related nephropathy associated with long-term paracetamol use.2,3
Due to altered pharmacokinetics and pharmacodynamics, the presence of multiple co-morbidities and polypharmacy, the elderly are more prone to adverse outcomes including the use of commonly prescribed medications.3,4 In frail elderly patients, it has been reported that clearance to paracetamol glucuronide was markedly reduced as compared to elderly who were fit. 5 Risk factors for paracetamol toxicity include older age, frailty, weight of ≤50 kg, malnourishment, presence of renal or liver impairment and hepatotoxic factors such as ethanol.6,7
Keeping the above in mind, there is a need to rationalise the use of paracetamol in older adults and dose adjustments may be necessary. Existing guidelines do not have specific dosing recommendations on the use of paracetamol in the elderly. However, some literatures caution the use of paracetamol in those who are malnourished or who weigh ≤50 kg. 7 Existing literature recommends a maximum dose of 60 mg/kg/day or 3000 mg/day in individuals <50 kg. 7 In individuals with cirrhosis and those who consume regular alcohol, a maximum daily dose of 2–3g per day has been considered safe.6,7 For individuals with severe renal impairment (creatinine clearance<30 mL/min), a dosing interval of at least 6 h is recommended. 7
There have been minimal studies to date on the use of paracetamol in elderly patients admitted for a fall. Pain from soft tissue injuries, fractures and dislocations are not uncommon and pain is often under-recognised in older adults 8 especially in those with dementia. 9 Older adults often underreport pain unless asked due to factors such as stigma associated with reporting pain, underlying cognitive impairment, impaired pain recognition and differing perceptions of pain. 10 Suboptimal pain control is associated with greater functional decline, social isolation, depression, poor sleep, and recurrent falls. 8 The objective of this clinical audit was to evaluate the prevalence of inappropriate paracetamol prescribing in the elderly admitted for falls and to introduce strategies to reduce the rate of inappropriate paracetamol prescribing in this population.
Methods
A clinical audit against locally developed criteria for inappropriate prescribing of paracetamol based upon available literature was conducted (Figure 1). Clinical charts of 100 patients aged ≥75 years old, admitted under the Geriatric Medicine department of a tertiary hospital with a primary diagnosis of a fall between July 2019 and October 2019 were reviewed. Demographic data collected included age, sex, and race. Medical history collected included a history of cirrhosis, cognitive impairment and its severity, alcohol use and whether the patient weighed <50 kg. Clinical charts were reviewed for the prescription patterns of paracetamol, including whether paracetamol was prescribed round-the-clock on admission and on day 2 of admission, the dose and duration of paracetamol prescribed round-the-clock during admission and on discharge, indications for paracetamol use, the ability of patients to give a coherent history or indicate pain and the presence of any agitation or restlessness documented by the doctors or nurses. Clinical data on the other types of analgesics prescribed together with round-the-clock paracetamol was also collected. Flow diagram for clinical audit. Algorithm for paracetamol prescription in elderly patients admitted for a fall.
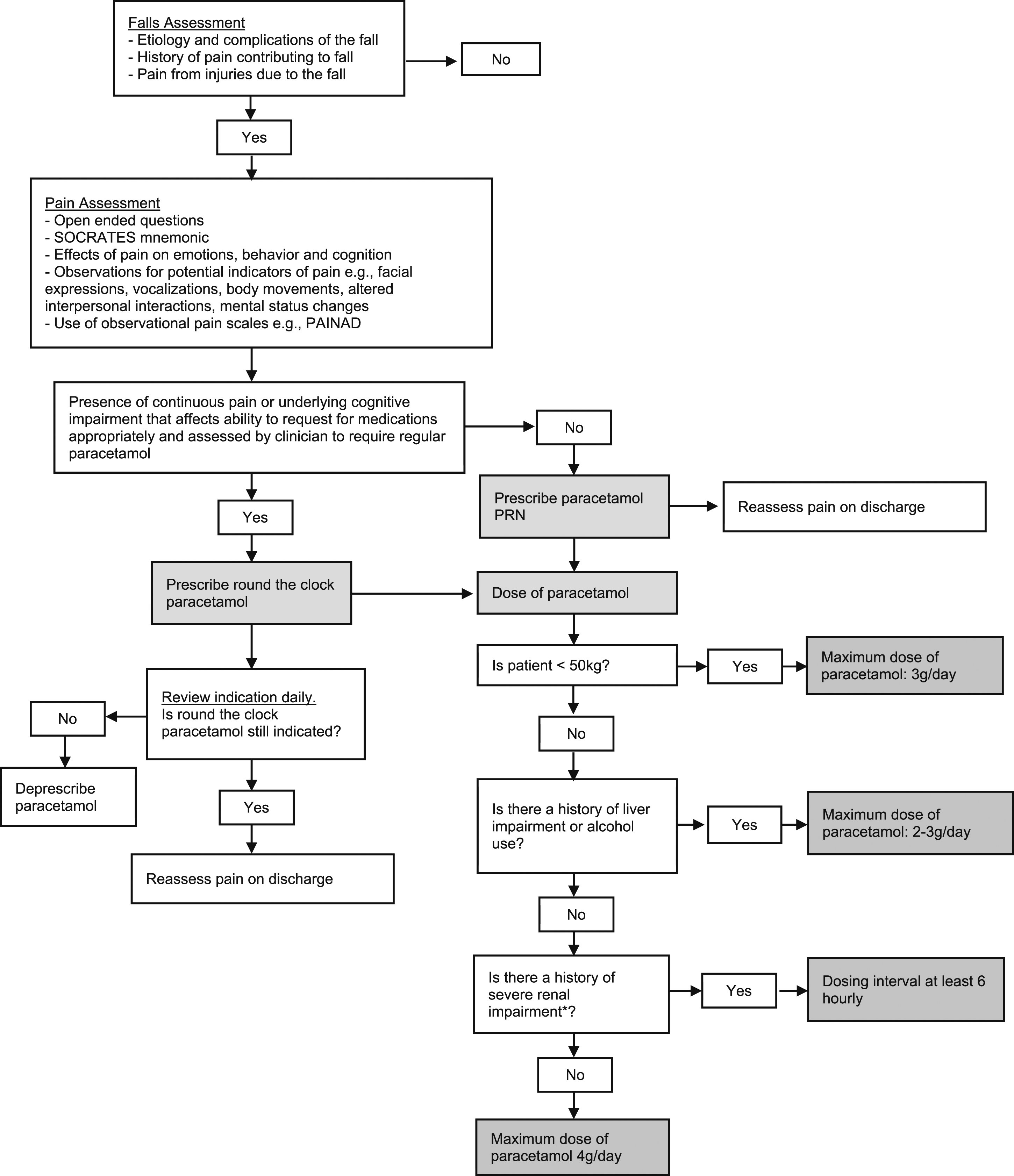
Inappropriate use of paracetamol in this study was defined as one out of the following three criteria: (1) Dose of paracetamol not adjusted according to body weight, renal or liver impairment and alcohol use; (2) Patients given a lower dose of paracetamol than what he or she should have received; (3) Patients who were prescribed round-the-clock paracetamol when there was no indication stated. For patients weighing <50 kg and those with underlying cirrhosis or consume regular alcohol, the maximum dose of paracetamol is 3 g/day. 7
Results
Summary of the demographics and medical history.
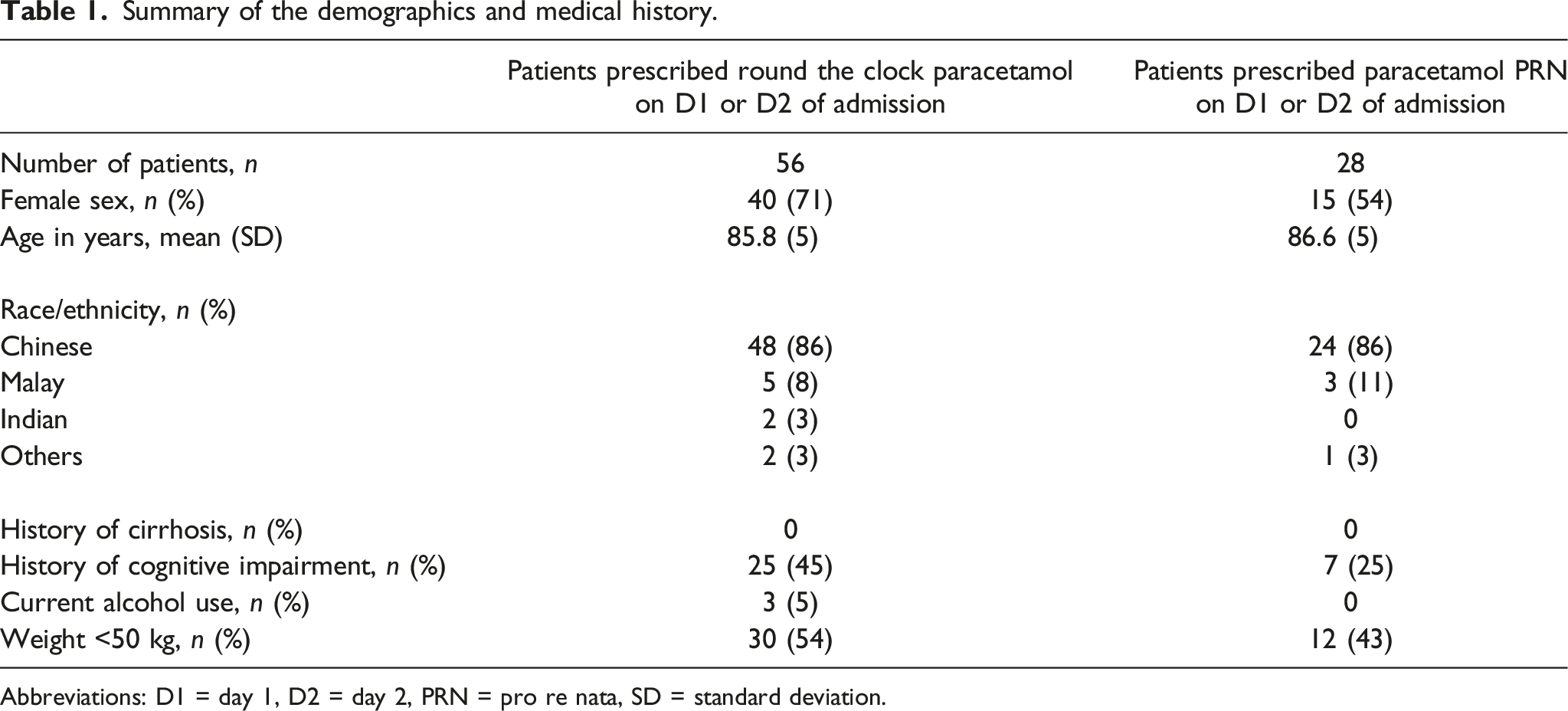
Abbreviations: D1 = day 1, D2 = day 2, PRN = pro re nata, SD = standard deviation.
Prescription pattern of paracetamol.

Abbreviations: D1 = Day 1, D2 = Day 2, PRN = Pro re nata, SD = Standard deviation.
In the group prescribed with round-the-clock paracetamol, 54 (96%) of them could indicate pain. This was based on clinical charts indicating patients verbalising pain or the ability of the patient to give a coherent history. The indication for round-the-clock paracetamol was not charted in 12 (27%) of the patients and 9 (82%) of them could indicate pain. The median number of other types of analgesics prescribed was 2 (IQR = 2).
Discussion
A thorough pain assessment is important for effective pain management. Components of pain assessment include the site and intensity of pain, effect of pain on affect, behaviour and function as well as the level of cognition affecting pain assessment. 11 An individual’s self-report on pain in the form of an interview or the use of standardised forms is the gold standard in pain assessment. 11
This clinical audit revealed a high prevalence of round-the-clock and inappropriate doses of paracetamol prescribed in elderly patients admitted for a fall. In addition, more than half of the patients who were prescribed round-the-clock paracetamol were discharged with round-the-clock paracetamol for a median duration of more than 2 weeks. Although paracetamol is recommended as a first-choice analgesic in various guidelines, 12 its use is not without the risk of adverse events especially in the elderly. Hence, it is prudent for paracetamol to be prescribed at the appropriate dose when indicated and to deprescribe whenever appropriate.
SOCRATES mnemonic for pain assessment.

If pain is assessed to be continuously present, round-the-clock paracetamol should be prescribed for pain with additional analgesic as appropriate based on the World Health Organisation (WHO) pain ladder. If pain is intermittent, paracetamol can be prescribed PRN. 15 In patients with an underlying cognitive impairment affecting their ability to request medications appropriately, 15 clinical judgement needs to be exercised in determining if round-the-clock paracetamol is indicated. Indications for round-the-clock paracetamol should be reviewed daily and paracetamol should be deprescribed whenever appropriate. Other considerations include weight, alcohol use, and the presence of kidney or liver impairment. On discharge, patients should be reassessed for pain again to determine if round-the-clock paracetamol is indicated.
This clinical audit highlights the prevalence of inappropriate paracetamol prescription in elderly patients admitted for a fall. It also emphasises the importance of judicious prescription of this commonly used analgesic considering the possible adverse events associated with its use, especially in the elderly. To our knowledge, this is the first article that proposes an algorithm to reduce the rates of inappropriate prescriptions of paracetamol in the elderly admitted for a fall. A limitation of this audit was the reliance on clinical documentation to ascertain whether prescription of paracetamol round the clock was indicated. Also, there were no patients with a history of cirrhosis or alcohol use in this clinical audit. As such, we were not able to glean insights to the prescribing pattern in this group of patients.
Conclusion
This clinical audit revealed a high prevalence of round the clock paracetamol prescribed and inappropriate doses of round the clock paracetamol prescribed in elderly patients admitted for a fall. Moving forward, we hope that with the implementation of this algorithm in our clinical setting, the rates of inappropriate paracetamol prescriptions in elderly patients admitted for a fall will be reduced. Other than serving as a reminder to clinicians of the need to be judicious in paracetamol prescription, it is also an opportunity to educate the junior doctors about the adverse events associated with paracetamol use and encourage good paracetamol prescribing habits.
Footnotes
Author contributions
AFY conceived and designed the programme, collected and analysed the data and wrote the manuscript. TKD conceived and designed the programme and edited the manuscript. SDV conceived and designed the programme and edited the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data
The datasets analysed during the current study are available from AFY.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.