
Abstract
Background
Preventing unwanted pregnancies, achieving optimal child spacing, and improving quality of life are benefits of modern family planning (FP). This study aimed to assess modern FP use, identify the factors influencing its use and determine the barriers to FP use among women of reproductive age.
Methods
A mixed-methods approach was conducted in the Iringa Region between March and July 2022. Conveniently, 368 women of reproductive age were included in the quantitative study, and 48 were purposively selected for the qualitative study based on reported barriers to using modern FP. Interviewer-administered questionnaires and interview guides were used for data collection. The factors of modern FP use were determined using multivariable logistic regression analysis. The p < 0.05 was considered to be significant. For qualitative data, all interviews were recorded and transcribed. Data were analyzed manually through thematic analysis.
Results
The prevalence of modern FP use was 181 (49%). Being married (adjusted odds ratio [AOR] = 5.44, 95% confidence interval [CI] = 1.77–16.73, p = .003), parity of 6 and more (AOR = 2.43, 95% CI = 1.99–5.95, p = .052), availability of modern FP methods (AOR = 1.71, 95% CI = 1.03–2.85, p = .038), and women with primary education level (AOR = 2.99, 95% CI = 1.03–3.25, p = .001), women with secondary and higher education (AOR = 3.53, 95% CI = 1.41–4.38, p = .001), were predictors for modern FP utilization. Four main themes merged (1) individual barriers, (2) hospital barriers, (3) cultural barriers, and (4) knowledge of modern FP methods.
Conclusion
The use of modern FP increases with women's education. There is a need for the government to invest in women's education and raise awareness and knowledge of the benefits of modern FP methods.
Introduction
Family planning (FP) refers to the use of contraception to prevent unwanted pregnancies, achieve the desired family size, and adequate child spacing. Traditional and modern methods are available, with modern methods increasingly popular among women of reproductive age. Globally, modern FP use has risen from 35% in 1990 to 45% in 2021. In sub-Saharan Africa, modern FP use has almost doubled from 24% in 1990 to 56% in 2021 (UNDESA, 2022).
Despite an increase in modern FP use, unacceptably high unmet FP needs (37%) persist in sub-Saharan Africa (UNDESA, 2022). In Tanzania, there has not been any significant change in the use of modern FP over the years. Tanzania Demographic Health surveys reported that the use of modern FP among married women had remained significantly low from 20% in 2004/05 to 32% in 2015/2016 (MoH, 2022), as compared to the national target of 60% of FP use by 2020 (Welfare & National, 2013). The low use of FP methods subjects women to a high risk of unintended pregnancies which can lead to unsafe abortions and puts women at high risk of complications and/or maternal death (Adane et al., 2020)
In the Iringa region, the estimated unmet FP needs are 12.7% (NBS, 2023), which impedes social and economic advancement, as women may be less able to contribute to the region and the country as a whole. Additionally, this impacts the achievement of the Millenium Development Goal, target 3.7 which calls on countries “by 2030, to ensure universal access to sexual and reproductive healthcare services, including modern FP information and education, and the integration of reproductive health into national strategies and programmes” (United Nations, 2020; p. 1).
Adequate use of modern FP reduces maternal death by 44% for unplanned pregnancies and unsafe abortions (Bhatt et al., 2021; Chekole et al., 2019). Modern FP use increases interpregnancy interval by over 2 years, preventing maternal and child mortality (Dierickx et al., 2018). Modern FP use also enhances women's education and economic growth by reducing dependence and increasing participation in national production activities (Dierickx et al., 2018).
Review of Literature
Evidence from various studies suggests that modern FP use is influenced by factors such as education level, economic status, attitude toward FP use (Imtishal et al., 2023; Oumer et al., 2020), knowledge of modern FP methods, husband approval, couple's discussion, male involvement in FP use decisions, desire for additional children, previous use of contraception (Asif & Pervaiz, 2019; Kassim & Ndumbaro, 2022; Moon et al., 2021; Mulatu et al., 2020), religious affiliation, low family income, fertility preference, negative perceptions of FP, preference for unproven FP methods, limited access to reliable sources of FP information, household responsibilities, and poor male partner support on FP matters (Akamike et al., 2020; Apanga et al., 2020; Kassim & Ndumbaro, 2022).
The Tanzanian government has been working on improving the accessibility and affordability of high-quality modern FP services in both public and private health facilities (MoH, 2022). The government have integrated FP services into reproductive health services and collaborated closely with nongovernmental organizations (NGOs) and development partners to provide free reproductive health services, including FP services (UNFPA, 2018). Despite free services, some women buy FP methods from pharmacies to avoid long waiting times (Keesara et al., 2015). National policies prioritize scaling up and strengthening contraceptive use for all women in need of FP services (MoH, 2022). However, despite government efforts, the Iringa region has a low use rate of modern FP (12.7%) (NBS, 2023). This raises questions about the factors influencing modern FP use for women of reproductive age in the region and the barriers that women face in accessing it. Therefore, this study aims to evaluate the use of modern FP, identify factors affecting its use, and determine barriers to its use by women of reproductive age in the region by answering the following questions:
What is the level of modern FP use among women of reproductive age? What are the factors that influence modern FP use? What are the barriers hindering women of reproductive age from using modern FP?
Materials and Methods
Study Design and Area
A community-based cross-sectional study using quantitative and qualitative methods was conducted in three districts (Mufindi, Mafinga, and Iringa Municipal) of the Iringa region from March to July 2022. The study was conducted due to the high fertility rate of 5.2 births per woman in the region, which was estimated to have a population size of 840,404 by the National Bureau of Statistics in Tanzania in 2020, also, the region is reported to have low rate (12.7%) of modern FP use among women of reproductive age (NBS, 2023).
Study Population and Recruitment Criteria
The study included all women of reproductive age (18–49 years) who lived in the selected study sites and agreed to participate. Both married and unmarried women in this age group who had lived in the study area for at least 1 year were eligible for inclusion. Women who did not give consent were excluded from the study.
Sample Size Estimation for the Quantitative Part of the Study
The sample size for this study was calculated using the Kish-Leslie formula for quantitative studies (Kish, 1957). A confidence interval of 1.96 was used, corresponding to a 95% confidence level, with 32% proportional to women of reproductive age using modern FP use as reported in the Tanzania Demographic Health Survey (NBS, 2016). A significance level of 5% (α = 0.05) was applied. The final sample size was adjusted to account for a nonresponse rate of 10% resulting in a total sample size of 368 participants. For the qualitative part of the study, six focus group discussions (FGDs) were conducted across the three selected districts. The researchers selected two FGDs from each district and each FGD had eight women making a total of 48 women participating across all six FGDs.
Sampling Technique and Recruitment of Study Participants
Simple random sampling using the lottery replacement method was used to select three districts out of seven, two wards were selected from each of the three study districts, and six villages in each of the selected wards. Households (205) were selected using a proportionate sampling method followed by extracting the 368 study participants from the households using convenience sampling methods as shown in Figure 1. For the qualitative approach, 48 study participants who participated in the quantitative study were purposively selected based on their reported experienced barriers to modern FP use. The researchers aimed to understand in detail what the barriers were. Women who refused to continue with qualitative study were excluded. The study used a face-to-face approach to interview them.
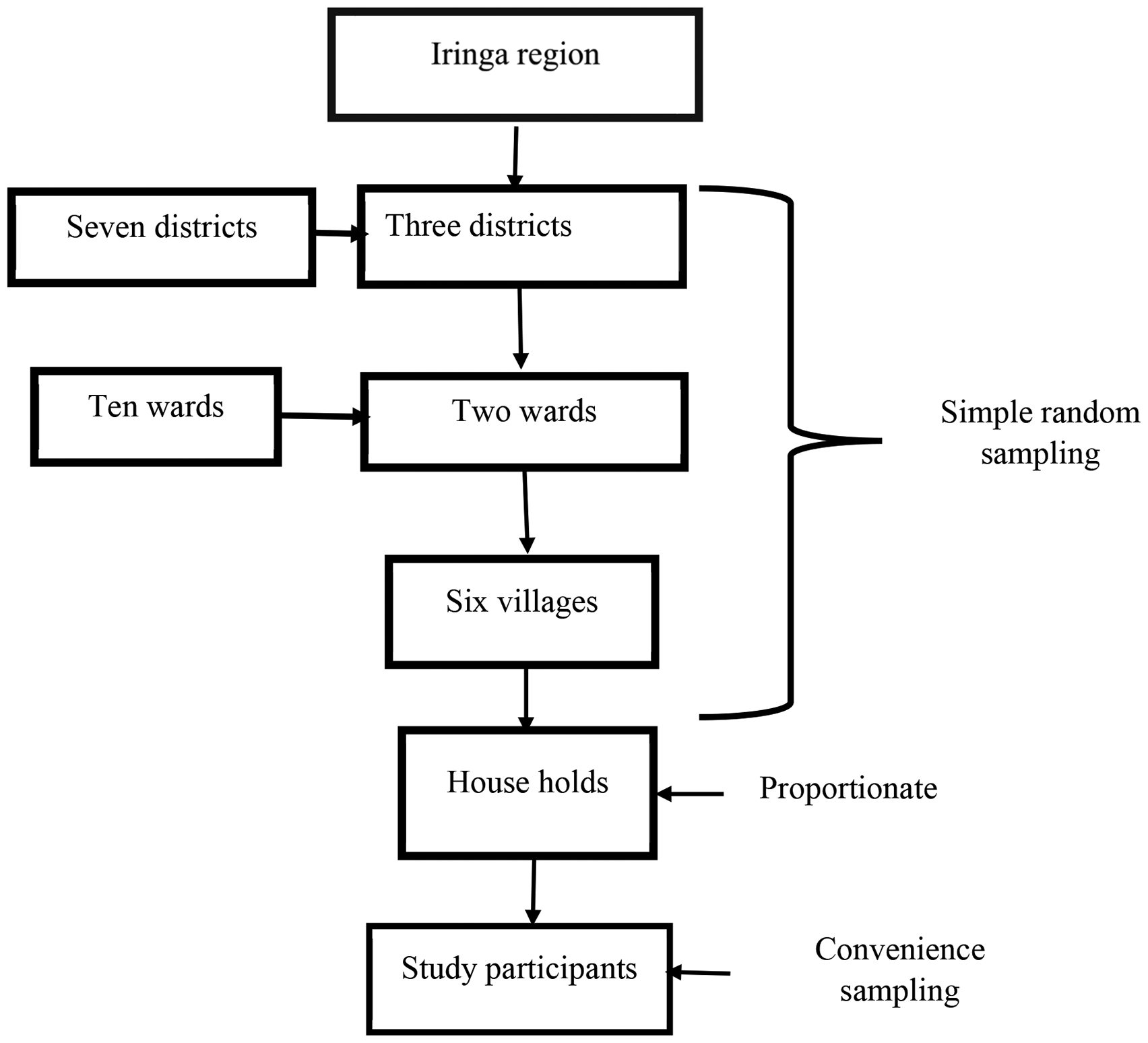
Flow chart for selection of study participants for the quantitative part of the study.
Definition of Variables
Participants were asked if they had used modern FP methods and responses were categorized as “yes” or “no.” The question was “Have you ever used a modern method of family planning?”
Data Collection Tools and Techniques
The study used an interviewer-administered questionnaire to collect relevant data. The questionnaire was adapted and modified from previous studies which were conducted in Western Ethiopia (Adane et al., 2020; Gizaw & Regassa, 2011), Nigeria (Ekpenyong et al., 2018), and Iraq (Alrawi, 2021). The questionnaire had three sections; sociodemographic characteristics, use of FP, and barriers to use of modern FP methods. The tools were prepared in English and translated into Swahili for easy understanding. The tools were pretested among 36 women of reproductive age, who were not included in the final study. Before using the questionnaire, its internal consistency was checked by calculating a Cronbach's alpha using data obtained from a pilot study which was found to be 0.782 for questions assessing barriers to using FP. Data were collected by the principal investigator and four assistant researchers (registered nurses) who were trained for 2 days before the process of data collection. In the qualitative part, the interview guide (Table 1) was used in FGD to collect qualitative data. During FGD conversations were recorded using an audiotape recorder and field notes were also taken, which took approximately 45 to 60 min. The discussions were conducted in Swahili with the aid of two skilled research assistants, BN/AJ, who have extensive experience in qualitative research. Probing questions were used when necessary to find out more detailed information regarding barriers to modern FP use. The study investigated different aspects of trustworthiness. To ensure the collected data was credible, researchers adopted the following strategies: peer debriefing, member checking, and prolonged engagement. Peer debriefing involved academic staff in the department who provided guidance and support from the proposal writing stage to the report of the findings. Member checking involved seeking approval from the participants for the transcripts and emerging codes from the interviews, establishing structural corroboration or coherence by testing all data to ensure that there were no internal conflicts or inconsistencies, and establishing referential adequacy. The research teams worked together to resolve any ambiguities in the coding process, categories, and themes. If the two researchers disagreed, they clarified definitions, collaborated, and continued with discussions until they reached a consensus. To ensure transferability, researchers used the purposive sampling method based on women who experienced barriers to using modern FP methods. To ensure privacy, data were collected in a separate location near the participant's residence. The FGD concluded that saturation was achieved when no new information was provided, and all data was transcribed into full text on the same day.
Interview Guide Used in the Qualitative Study to Assess the Barriers to the Use of Family Planning Among Women of Reproductive Age.

Data Analysis
Statistical analysis was performed using Statistical Package for Social Science (SPSS) version 25. Descriptive statistics were used to analyze the sociodemographic characteristics and the results were presented in proportions. Inferential statistics comprised binary logistic regression analysis for determining the predictors of modern FP utilization. All variables with p ≤.2 in univariate analysis were fitted into multivariable analysis for controlling confounding factors. Odds ratios (ORs) at 95% confidence interval (CI) were determined to assess the predictability of the independent variables. A two-tailed p < .05 was considered statistically significant.
In the qualitative part of the study, data were transcribed verbatim from the Swahili language to English and proofread by reading and re-reading by two researchers (BN/AJ) in the first instance to formulate units of meaning, followed by an interpretive phenomenological thematic data analysis approach. The researcher got familiarized with data, looked for similarities, and developed codes which were later polished to form subthemes and themes. Research teams cross-validated the emerging themes. The audio-recorded data were transcribed into full text on the same day but also field notes were taken parallel with the audio recorder and used as backup notes if the audio recorder failed. The interviews were transcribed and analyzed manually by thematic analysis.
Results
Sociodemographic Characteristics of the Study Participants
A total of 368 women of reproductive age were interviewed (response rate of 100%). The mean age of study participants was 20.5 ± 8.05 years ranging from 18 to 49 years. Most 155 (42.1%) of the study participants were aged 28 to 37 years. The majority 253 (68.8%) of the participants were married. Slightly more than half 203 (55.2%) of the participants had attained primary education and 200 (54.3%) were self-employed. More than half 206 (56.0%) of the study participants had a family income of less than 1.4 USD/100,000 TZS per day. The majority 232 (63.0%) of the study participants were Christians and 233 (63.3%) women had a history of use of FP methods (Table 2).
Sociodemographic Characteristics of the Study Participants (N = 368).
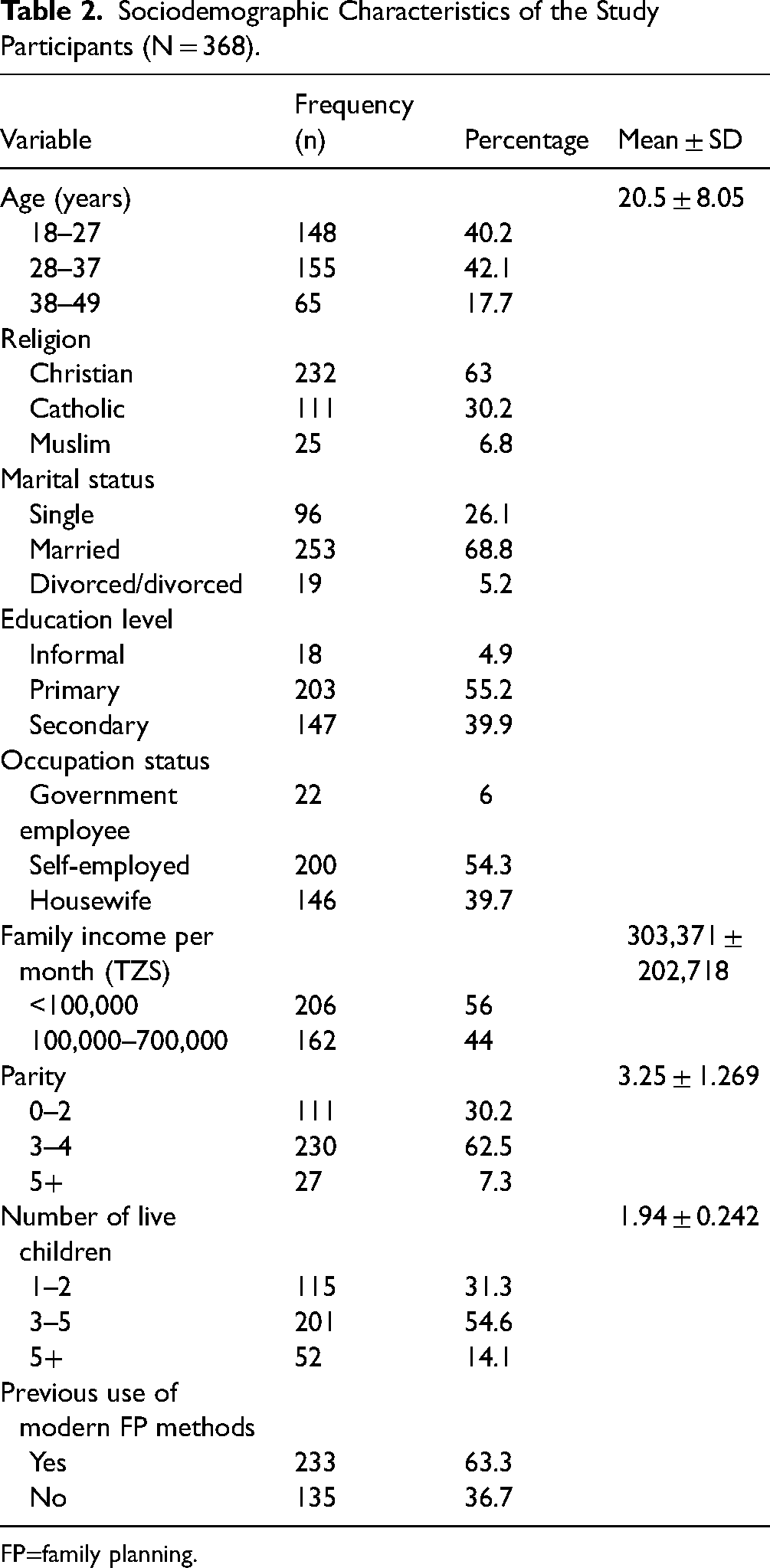
FP=family planning.
Prevalence of Modern Family Planning Methods Use
The prevalence of modern FP methods used by study participants at the time of data collection was 181 (49.2%) (Table 3).
Prevalence of Modern Family Planning Use Among Study Participants.

FP=family planning.
Reported Types of Modern Family Planning Methods Used by Study Participants
The most reported modern FP methods that were used by participants include implants 81 (44.8%), injectable 47 (25.9%), pills 31 (17.1%), male condoms 11 (6.1%), and intrauterine devices 11 (6. 1%) (Figure 2).

Types of family planning methods utilized by study participants (N = 181).
Source of Modern Family Planning Methods Among Women
Most 150 (40.8%) of the study participants reported obtaining modern FP methods from government health facilities, while 15 (4.1%) obtained FP methods from private facilities, 6 (1.6%) from pharmacies, and 10 (2.7%) from outreach clinics (Figure 3).

Source of modern family planning methods among study participants (N = 181).
Reasons for Discontinuation of Modern Family Planning Methods Use
Out of all the study participants, 233 individuals (63.3%) had stopped using contraceptive methods. Fear of side effects was the main reason cited by 94 (40.3%) participants. Other reasons were religious restrictions 22 (9.4%), long distances 14 (6.0%), partner opposition 13 (5.6%), preference for male babies 45 (19.3%), and intention to get pregnant 45 (19.3) (Figure 4).

Reasons for discontinuation of modern family planning methods among women with a history of using them (N = 233).
Barriers to Modern Family Planning Use by Women of Reproductive Age
The majority 278 (75.5%) of study participants reported waiting long hours, 256 (69.6%) husbands’ disapproval and 192 (52.2%) experienced side effects were the most barriers reported by women during the survey. However, the Tanzania government has its policy of free access to FP use, most 156 (42.4%) of study participants don’t go to the health facility but instead go to the small shops to buy modern FP (Table 4).
Barriers to Modern Family Planning Use by Women of Reproductive Age (N = 368).

FP=family planning.
Multivariable Regression Analysis for Factors Associated With Modern Family Planning Use Among Study Participants
After controlling for confounders (religions and husband approval to utilize modern FP methods) in multivariable regression analysis, age, married women, education level of participant, parity of 3 to 5, and availability of FP methods at the facility were found to be statistically significantly associated with modern FP utilization. Women aged 18 to 27 years were 57.8% significantly less likely to utilize modern FP when compared to women aged 38 to 49 years (adjusted OR [AOR] = 0.42, 95% CI = 02–0.91, p = .028), however, married women were five times more likely to utilize modern FP compared to single women (AOR = 5.44, 95% CI = 1.77–16.73, p = .003). Women with primary education were almost three-fold more likely to utilize modern FP compared to women with informal education (AOR = 2.99, 95% CI = 01.03–3.25, p = .001), while women with a secondary and higher level of education were almost four-fold significantly more likely to utilize modern FP compared to women with informal education (AOR = 3.53, 95% CI = 1.41–4.38, p = .001), women with parity of 3 to 5 were almost four times more likely to utilize modern FP compared to women with parity of 0 to 2 (AOR = 3.97, 95% CI = 1.35–2.72, p = .959), women with six and more children were 2.43 times more likely to utilize modern FP compared to women with parity of 0 to 2 (AOR = 2.43, 95% CI = 1.99–5.95, p = .052) and availability modern FP methods was 1.71 more likely to influence FP use compared to unavailability of FP commodities (AOR = 1.71, 95% CI = 1.03–2.85, p = .038; Table 5).
Factors Associated With Use of Modern Family Planning Among Women of Reproductive Age (N = 368).
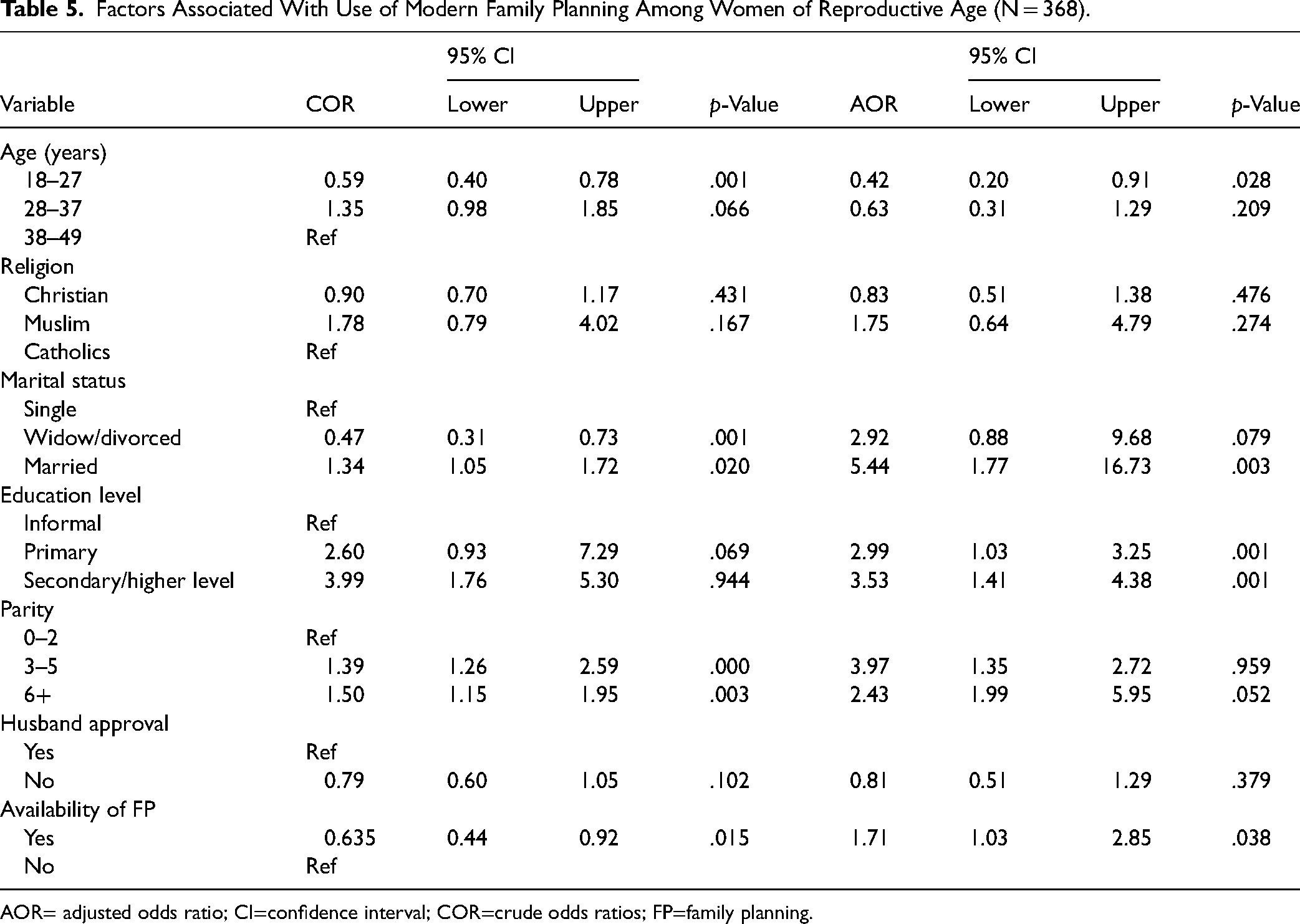
AOR= adjusted odds ratio; CI=confidence interval; COR=crude odds ratios; FP=family planning.
Findings of Qualitative Research Method
A total of 48 study participants from the selected communities participated in six focus group discussions (FGDs). Barriers were grouped into four themes: individual, hospital, cultural, and knowledge of modern FP methods.
Theme 1: Individual Barriers
Fear of Side Effects
Fear of side effects was reported by most of the participants as one of the bottlenecks for modern FP utilization. Rumors of side effects such as prolonged bleeding and infertility have contributed to increased fear among community members. Participants mentioned side effects as a barrier that hinders the use of modern FP services. This was also reported by one participant in the focus group discussion: “I had implants for three years, I experienced prolonged bleeding every month and spot most of the time, these side effects bring challenges on my marriage life, I decided to remove the implant” (M1P4 FGD).
Another participant reported
“I used injections for almost nine months and didn’t see my periods. I believed this was a side effect of the injections and worried that blood was accumulating in my abdomen, which could lead to a uterine tumor or infertility. As a result, I decided to stop using the injections.”(M12P3FGD)
Poverty
The majority of the participants in the study are currently unemployed and rely on their husbands for financial support. Due to their low financial status, some women are unable to afford basic medical supplies such as syringes, gloves, and even urine tests for pregnancy. This lack of financial resources often leads to the under use of modern FP methods. For instance, during one of the focus group discussions, a participant shared that
“My friend was unable to afford an implant insertion due to the cost of Tsh 4000 for the necessary hospital medical supplies. Unfortunately, her husband refused to give her money for modern FP methods.” (M2 P8 FGD)
Unsatisfactory Family Planning Services
Clients often have to wait in long queues before they are attended to, which can lead to delays and make it difficult for them to participate in daily economic activities. Many participants have cited long waiting times as one of the major barriers they face when trying to access modern FP services. This was also raised by one of the participants during FGD:
I arrived at the health facility at 7: am, but I had to wait until noon for modern FP services. Next time, I will go in the afternoon after my work (M10 P3FGD).
Opposition From Husband
In African culture, men hold the final decision-making power at the family level. Some women lack the authority to make decisions regarding fertility and FP utilization. They are required to seek permission from their husbands before using FP methods. Unfortunately, the majority of men prevent their wives from using FP, as they believe that the primary purpose of marriage is to bear children. During an FGD, one of the participants reported this issue:
My husband told me that, I permitted you to go with the baby at the under-five clinic only and not for family planning services, once I discover that you are utilizing modern family planning, I will harm you.” (M5P31 FGD)
“It is not easy to use modern FP methods without permission from our husbands because women have no power to decide. Also, convincing men on issues of FP is very difficult as our culture accepts many children as rich.” (M5P32 FGD)
Theme 2: Hospital Barrier
Effective FP services need the availability of a constant supply of FP commodities and hospital supplies. Stock out of FP commodities adversely affects women choosing the preferred FP methods and leads to underutilization. As shown in Table 5, 112 (30.4%) of the participants reported a lack of FP commodities as one of the barriers to the use of modern FP. This was also reported by one of the participants that:
I went to a health facility for implant insertion, but the health provider told me that there were no implants, the remaining commodity is IUCD because I don’t prefer IUCD, I went back home.” (M11P21 FGD)
Theme 3: Cultural Barriers That Hinder the Use of Modern Family Planning Methods
Societal Norms
Preference for many children is still being valued by some clans in rural villages. Some families have up to 10 children. Other women believe that they should give birth to all children until all eggs are finished in the ovary. Some women believe that by having many children, life will be improved. As shown in Figure 4, 5.17% of the participants who were not using modern FP reported that preference for male babies prevents them from using modern FP. One of the participants from the focus group discussion explained that:
In our culture women are not allowed to have fewer than 4 children, you will get pressure from your husband's family and mother-in-law, and they will ask you why don’t you add more children. you will be sent to different traditional healers available in the village to get treatment to unblock the tube to have another pregnancy. (M13 P33 FGD)
Religious Factors
In the conservative community, religion is an integral section of life and influences the use of modern FP. Religious teaching discourages the use of modern FP and advocates for natural FP. The effectiveness of the use of natural FP is challenging. As shown in Figure 4, 22 (18.9%) of the participants reported religion as a barrier that hinders the use of modern FP. The quotes below from participants explain how religion prevents using modern FP.
“Religious teaching prevents the use of modern FP methods but it encourages the use of natural FP methods for only those who are in a marriage, it is against God's will, the teachings said that those utilizing modern FP are killing and killing is a sin.” (M16 P13FGD)
Theme 4: Knowledge of Modern FP Methods
Low Awareness of Modern FP Methods
The majority of the participants are aware of different modern FP methods but others are not well informed on female condoms, and emergency contraceptives. Low awareness of modern FP prevents women from having the right to be informed of FP choices hence leading to underutilization. This has also been reported in the quantitative part of this study such as in Table 3, which presents 123 (33%) of the participants who reported to know female condoms. One of the participants from the focus group discussion reported that:
“I heard that there are female condoms, but I have never seen them in my life, and I don’t know how they are being utilized.” (M17 P1 FGD)
Misconception of Family Planning
Misconception on modern FP is a challenge that leads to low utilization. Any information that has an impact on future fertility brings fear among women in the community and must be rejected. One of the participants from the focus group discussion reported that:
“Oral pills are not good methods for family planning at all, women who utilize this method will never get children in their life, actually pills bring infertility.” (M18P25 FGD)
Discussion
The objective of the study was to assess modern FP use, identify the factors that influence modern FP use, and determine the barriers to modern FP use among women of reproductive age in the region. The prevalence of modern FP use in this study was higher than the reported rates in Guinea (12.8%), Bauchi (18.4%), Kenya (18.6%), Senegal (26.3%), Zambia (33.2%), Kagera and Mara, Tanzania (43%), Ethiopia (41.2%), and Burundi (23.8%) as documented by Sidibé et al. (2020), MS et al. (2018), Moon et al. (2021), Zegeye et al. (2021), Lasong et al. (2020), Massenga et al. (2021), Oumer et al. (2020), and Nkunzimana et al. (2021), respectively.
However, a higher prevalence of modern FP use was reported among women of reproductive age, with rates of 54.8% in Malawi (Forty et al., 2021), 54.7% in Jordan (Komasawa et al., 2020), and 63% in Kenya (Moon et al., 2021). The difference observed in the prevalence of modern FP use may be caused by differences in cultural beliefs (Ekpenyong et al., 2018), ethnicity (Zegeye et al., 2021), education level (Forty et al., 2021), religion (Akamike et al., 2020), partner support (Massenga et al., 2021), and FP services and different ways of providing health education from different settings globally (Komasawa et al., 2020; Sidibé et al., 2020).
This study found that being married was associated with modern FP use. This is similar to the findings in the studies done elsewhere. For example, in the study done in the Kagera and Mara region, Tanzania was reported that married women were more likely to utilize modern FP (Massenga et al., 2021). Another study which was done in Ethiopia reported that married women were more likely to use modern FP (Mulatu et al., 2020). Furthermore, it was observed that women with three to five children were associated with the use of modern FP methods. A similar finding was reported by various studies, such as the study conducted in rural Zambia (Lasong et al., 2020), Senegal (Zegeye et al., 2021), and Ethiopia (Endriyas et al., 2017). The reason that multipara women tend to use modern FP methods may be attributed to the reality of the increased cost of living in all aspects of life, such as food, healthcare services, and education.
Level of education influences health behavior, researchers found that women with secondary and/or higher levels of education were more likely to use modern FP methods. This is similarly reported by several previous studies, which reported a positive association between modern FP use and secondary and/or higher education levels in Rwanda (Kanakuze et al., 2020), Malawi (Forty et al., 2021), Ethiopia (Adane et al., 2020), rural Zambia (Lasong et al., 2020), northwest Ethiopia (Oumer et al., 2020), and Liberia (Tsegaw et al., 2022). The similarity observed may be attributed by the reality that education influences health behavior change. Women who have higher levels of education tend to be more empowered when it comes to making decisions about fertility control. Furthermore, women with higher levels of education are better equipped to comprehend health information related to the use of modern FP methods. It is also likely that women with more education have increased access to health services, including modern FP, as higher education can lead to higher income levels. Additionally, women with higher education levels are often employed or self-employed and tend to have fewer children due to busy schedules, as a result, they are more likely to utilize modern FP methods.
According to a recent study, women who did not receive approval from their husbands tended to use modern FP methods less frequently. However, this finding was not statistically significant. This result is consistent with previous studies conducted in the Mara region, Tanzania (Baritwa & Joho, 2024), Rural Eastern Ethiopia (Mulatu et al., 2020), Indonesia (Joesoef et al., 2016), Ethiopia (Chekole et al., 2019), and Turkey (Alan Dikmen et al., 2019). Traditionally in African culture, men are the head of the family, hence men had power in decision-making on issues of family size and FP utilization. Women prior use of FP needed to get approval from their husbands, the majority of men resisted the use of modern FP with their wives. This is among the barrier to access and choice of use of modern FP methods. This finding agrees with a study done in Congo and Tanzania (Baritwa & Joho, 2024; Muanda et al., 2017). This might be caused by the nature of patriarchal culture where men had the final say in reproductive health decisions. The lack of approval from husbands may be attributed to factors such as their level of education, inadequate knowledge about modern FP methods, cultural beliefs that having many children is a sign of prestige, and negative attitudes toward women who use modern FP methods, as some men may view them as promiscuous. Additionally, a husband who does not allow his wife to make decisions on reproductive issues exercises reproductive coercion (Baritwa & Joho, 2024; Silverman et al., 2020; Wood et al., 2020), which affects women psychologically (Silverman et al., 2020). Therefore, educational programs on modern FP methods must target men and women in the community.
In the current study, the availability of modern FP methods was positively associated with its utilization. The finding is in line with studies conducted in Bangladesh, the Democratic Republic of Congo (DRC), and Haiti (Fallon & Ijdi, 2022), Rural Eastern Ethiopia (Mulatu et al., 2020), in Ethiopia, Nigeria, and DRC (Riley et al., 2018), Nigeria (Akamike et al., 2020), and Bauchi state (MS et al., 2018).
In both quantitative and qualitative findings, it is indicated that several barriers may reduce the use of modern FP, including fear of side effects, opposition from husbands, religious factors, and waiting long times to be attended. Religious beliefs are a significant challenge in scaling up the use of modern FP services. Many community members do not use modern FP methods due to criticism from religious leaders and church members, which makes them afraid to use them (Muanda et al., 2017; Nakirijja, 2018). Furthermore, some community members believe that using modern FP methods is against God's will and is a sin. Similar findings were reported in previous studies conducted in Nepal (Bhatt et al., 2021), North West Tanzania (Sundararajan et al., 2019), and rural Burundi (Ndayizigiye et al., 2017). In this regard, it is essential for religious leaders to be well-informed about accurate information concerning FP, so they can share this knowledge appropriately. Encouraging women to have many children can increase their risks during pregnancy, potentially leading to higher rates of maternal morbidity and mortality. Moreover, women have the right to make decisions about their bodies and the number of children they wish to have, considering their health and financial circumstances. Families with low incomes often struggle to provide for their children's education, which can lead to children engaging in early employment, facing early pregnancies, or even becoming street children.
The negative health effects of modern FP have been overrated by the community due to their side effects. For instance, the loss of menses was believed to cause uterine tumor and infertility. In African culture, infertility is underrated, and women who cannot give birth often encounter social isolation, rejection, and are replaced by other women in their marriage. Therefore, any risks that threaten women's fertility should be avoided. Similar findings were reported from studies conducted elsewhere, for example, in Saudi Arabia (Abdel-Salam et al., 2020), Eastern Senegal (Cohen et al., 2020), Urban Gambia (Dierickx et al., 2018), and Tanzania (Mushy et al., 2020). To dispel rumors in the community, intervention is needed through the empowerment of community workers who can provide accurate information on modern FP and its side effects.
Also, the findings from both quantitative and qualitative studies indicated that many women do not use modern FP methods because their husbands do not permit them. This is consistent with studies conducted in various countries, including Tanzania (Baritwa & Joho, 2024), Pakistani (Sarfraz et al., 2023), India (Vishwakarma & Shekhar, 2022), and Uganda (Sarnak et al., 2021). Husband opposition to FP use may be due to several reasons, such as the belief that men are the decision-makers in the family and have control over their wives’ use of modern FP and child spacing. In addition, men in African regions often find it prestigious to have many children and consider the use of contraceptives as a threat to their masculinity. Male partners must be involved in health education and information, including learning about the advantages and disadvantages of modern FP methods. They need to understand that women have the right to make decisions about their own health, including the use of modern FP.
Both quantitative and qualitative data indicated that long waiting times to be attended by a healthcare provider are a prevalent issue. This is consistent with findings from various studies conducted in other regions, including peri-urban Nairobi (Hassan et al., 2022), the United States (Karra & Canning, 2020), and Appalachian (Swan et al., 2020). As a consequence, women may opt to purchase modern FP products from shops due to the discouragement caused by the long wait times.
Strengths
The use of both quantitative and qualitative approaches helped to explore detailed insights regarding modern FP use among women of reproductive age.
Limitations of the Study
The study was cross-sectional and relied on self-reporting of contraceptive use among women of reproductive age, which might not show a causal relationship.
Implications
This study has investigated the reasons for women not using modern FP methods and suggests that stakeholders such as policymakers and nongovernmental agencies should take action to address this issue. One suggestion is to provide educational interventions which emphasizing the importance of modern FP, clarify any misconceptions or concerns about side effects, and involve husbands in the process to ensure their understanding and approval of their wives using modern FP methods.
Conclusion and Recommendation
The proportion of modern FP use in the region is below the national target. To increase modern FP use there is a need to address solutions to the reported barriers to the utilization of modern FP methods by increasing the efforts on male involvement, raising awareness among community members including religious leaders on the benefits of modern FP methods, comprehensive counseling, and correct information regarding side effects of modern FP methods should be given to both partners for them to provide couple informed decision.
Footnotes
Acknowledgments
We appreciate the nonfinancial support which was provided by the University of Dodoma and we would also like to express our gratitude to all study participants, research assistants, and administrative leaders at all levels for their valuable contributions to this study.
Authors’ Contributions
The authors’ contributions to the research project are as follows: BN was responsible for conceptualizing the study, designing the research methodology, curating the data, analyzing the data, and writing the first draft of the manuscript. AAJ contributed by providing guidance and supervision throughout the study, conducting an in-depth literature search, and writing the first draft of the manuscript. All authors reviewed the final version of the manuscript and agreed to be held accountable for the intellectual content presented in the article.
Availability of Data and Materials
The data will be available upon special request from the University of Dodoma.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate and Study Approval Number
This research was approved by the research ethical committee of the University of Dodoma (Ref. no. MA. MA.84/261/02/ issued on March 18, 2022. The study obtained informed consent from participants after fully explaining the study's objectives and procedures.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.