
Abstract
Introduction
Data on how the health belief model constructs might predict the self-care behavior of patients with cardiovascular disease (CVD) post-coronavirus disease (COVID-19) 2019 pandemic are scarce.
Objective
This study determines the predictors influencing patients’ intention to adhere to self-care for CVD in the United Arab Emirates after the COVID-19 pandemic.
Methods
A descriptive cross-sectional design was used. A total of 222 patients with CVD were purposively selected. Three scales were used: Health Beliefs Related to Cardiovascular Disease, Physical Activity Measurement, and Behavioral Intention Measurement. Various socio-demographic and clinical characteristics and the participants’ health belief components were considered potential factors in the multivariate analysis to identify the independent predictors of the intention of self-care behaviors.
Results
The participants had a high level of perceived CVD risk (M = 4.02, SD = 0.714) and high level of perceived benefits regarding adopting healthy behavior (M = 4.30, SD = 0.817). The multiple linear regression revealed that not performing regular sweating exercises (β = 0.230), not receiving smoking cessation instructions (β = 0.214, p = .005), being sufficiently active (β = 0.304), and having no history of heart surgery (β = 0.155) were the independent predictors of low intention scores. The perceived benefits and perceived cues to the action of the Health Belief Model (HBM) were significant independent predictors of behavior intention and were responsible for a 22% increase in the participants’ intention variances.
Conclusions
In a post-COVID CVD, this investigation delineated perceived benefits and cues to action derived from the HBM as the most robust prognosticators of behavioral intention (accounting for 47% of the variance), superseding sociodemographic and clinical parameters (explaining 25% of the variance). These results advocate for tailored interventions accentuating individual advantages and explicit prompts for behavioral modifications within this demographic.
Introduction/Background
Cardiovascular disease (CVD) is the most significant cause of mortality and disability globally, accounting for 30% of all deaths (Ekong, 2021; Münzel et al., 2022; Ntusi, 2021; Toth, 2021). This category of diseases commonly referred as heart disease encompasses a range of conditions related to atherosclerosis, including heart attack, stroke, arrhythmia, and heart failure (American Heart Association, 2023).
In the United Arab Emirates (UAE), cardiovascular disease is the leading cause of mortality, accounting for 29.89% of all fatalities (Al Rawahi et al., 2017; Razzak et al., 2018). The UAE has the second-highest cardiovascular death rate after Saudi Arabia, which is higher than in the Gulf Cooperation Council nations and high-income countries like Germany, United States, and Sweden (World Heart Federation, 2017).
The post-COVID-19 era has uniquely impacted patient well-being and their perceptions of the severity of their ailments. The intense focus on preventing COVID-19 transmission had previously diverted attention, yet now, subsequent to the pandemic, patients afflicted with CVD encounter novel hurdles in reinstating and upholding their health regimens (Duffy et al., 2020). Lingering repercussions of the pandemic have reshaped patients’ outlook on their well-being and the imperative of continual self-care. Numerous CVD patients have endured disruptions in customary healthcare services and support networks, adversely impacting their adherence to lifestyle adjustments and healthful routines (Background, 2020). Amidst the pandemic's abatement, individuals with CVD necessitate the reestablishment and perpetuation of these lifestyle changes, particularly in view of sustained social distancing measures, heightened remote work practices, and the psychological aftermath of prolonged isolation (e.g., post-pandemic syndrome). The decrease in physical activity levels instigated during the pandemic remains a concern, as patients may encounter challenges in incorporating regular exercise into their daily routines. Additionally, the psychological toll of the pandemic has heightened stress and anxiety levels among CVD patients, further complicating their ability to comply with recommended self-care routines. Thus, the post-pandemic era presents a pivotal juncture to reassess and fortify the significance of healthful behaviors in managing CVD. Healthcare practitioners must concentrate on devising strategies to assist patients in navigating these obstacles, ensuring the resumption and perpetuation of efficacious self-care practices. This entails addressing the psychological ramifications of the pandemic, advocating for physical activity, and furnishing continuous education and support to underscore the importance of lifestyle modifications in the management of cardiovascular health.
Review of the Literature
Health authorities raised several health recommendations during the pandemic to encourage patients with CVD to engage in more physical activity, adhere to a healthy diet, and reduce their caloric intake to avoid weight gain (Duffy et al., 2020). These recommendations align with cardiac rehabilitation (CR), combining exercise, risk factor modification, and psychosocial support to minimize morbidity and mortality for patients with cardiovascular disease. However, research found that during the COVID-19 pandemic, there has been a decline in cardiac rehabilitation participation along with CR center closure (de Melo Ghisi et al., 2021). This, in turn, affected rural and low-income patients with CVD and the most socially vulnerable communities (Varghese et al., 2022). There is, therefore, a need to understand the changes in patient perception and intention when it comes to taking their cardiovascular medication, engaging in rehabilitation activities, and striving for a healthy lifestyle in the context of the COVID-19 pandemic.
In the aftermath of the pandemic, patients may encounter persistent challenges in complying with their pharmacological protocols, engaging in rehabilitative endeavors, and maintaining healthy lifestyles (Lovett et al., 2023). Concerns regarding nosocomial infections, financial hardships, and ongoing disturbances in healthcare services may further complicate patients’ ability to prioritize and effectively manage their cardiovascular well-being.
Understanding these transitions is crucial for formulating interventions to strengthen patient care in the aftermath of the pandemic, ensuring they receive the necessary care and resources for proficient management of their CVD. This necessitates a thorough exploration of the enduring impact of the pandemic on patient conduct and the healthcare infrastructure's capability to accommodate these needs.
The Health Belief Model (HBM) examines the link between health beliefs and self-care behaviors, suggesting that preventative activities are influenced by one's views (Chang & Lee, 2015; Kamran et al., 2014). According to this model, adopting self-care behaviors first requires recognizing that they are susceptible and liable to developing CVD complications (perceived susceptibility), that CVD and its complications worsen health outcomes (cardiovascular diseases) and cause harm to health (perceived severity), that self-care behaviors have some benefits (perceived benefits), that there are some barriers to behavior changes (perceived barriers), that their family members, relatives, neighbors, health care professionals, and the media (television, internet, newspaper, broadcast) encourage them to adopt healthy behaviors (cues to action), and finally, that they can control their CVD risk factors through self-care behaviors (perceived benefits) (self-efficacy) (Bayrami et al., 2021; Mohamed et al., 2021; Walker et al., 2021; Zamzuri et al., 2021).
The HBM has been extensively used in the literature to predict the self-care behavior of patients with chronic illnesses and cancer (Kirag & Kızılkaya, 2019; Willis, 2018). Nevertheless, its applicability in predicting the self-care behaviors of CVD patients post-COVID-19 pandemic remains unexplored and uncertain. Despite the World Health Organization no longer classifying COVID-19 as a pandemic, caution is warranted, as scholars advise. Recent evidence suggests that post-COVID syndrome may continue to affect a substantial proportion of patients with chronic conditions, necessitating integrated diagnostic and therapeutic approaches (Martín Sánchez et al., 2023). Likewise, a prospective study found that adopting a healthy lifestyle is correlated with a notably decreased risk of developing post-COVID-19 complications, such as cardiovascular dysfunctions (Wang et al., 2023). Consequently, the study seeks to identify the determinants influencing patients’ inclination to adhere to self-care practices for CVD in the United Arab Emirates (UAE) post COVID-19 pandemic.
The findings may illuminate key factors driving adherence to self-care behaviors, offering crucial insights for tailoring effective interventions. These interventions will be formulated to support residents in sustaining healthy habits, ultimately enhancing cardiovascular health outcomes in the post-pandemic context.
Methods
Design
A descriptive cross-sectional study was adopted. Hospitalized patients with chest pain related to cardiac disorder were recruited between January and July 2021.
Sample
A purposive sampling method was used at three hospitals in the Northern Emirates of the UAE.
Inclusion/Exclusion Criteria
Eligible patients were those (1) admitted to the hospital with chest pain secondary to cardiac disease as confirmed by the physician or their medical record, (2) had a previous history of CVD, (3) who had no cognitive and mental disorders, and (4) who agreed to join the study voluntarily. Patients diagnosed with acute myocardial infarction (MI) with severe complications (cardiac arrest, life-threatening cardiac dysrhythmias, acute renal failure), auditory or visual impairments, and who understand the questionnaire were excluded. Trained research assistants explained the study purpose and procedure to eligible patients. Based on the medium effect size (f2 = 0.15), alpha of 0.05, the power of 0.9, and 20 predictors, G*Power. The number of participants calculated was 148. Considering a dropout rate of 10%, which includes refusal to participate and failure to complete the survey, the minimum number of participants required for the study was 163. However, the researchers aimed to recruit a larger sample to represent the population better. Informed consent was obtained from eligible participants.
Materials
Independent Outcomes.
Health Beliefs Related to Cardiovascular Disease Scale
Initially, participants were asked to complete a self-reporting questionnaire and four parts before their hospital discharge. Part one included the patient's socio-demographic characteristics (i.e., sex, age, marital status, working status, residential area, and level of education). The part on clinical characteristics included the patient's history of comorbidities, their smoking status, and their adherence to a healthy diet. In this study, the term ‘comorbidity’ is defined as any long-term health condition that coexists in a patient with CVD (Russell et al., 2023).
The patient's beliefs about CVD were measured using a modified version of the HBM consisting of 25 items divided into five constructs (Tovar et al., 2010). These were perceived susceptibility or being at risk of CVD (five items), perceived severity (five items) or the seriousness of developing CVD, perceived benefits of adopting healthy activities for preventing recurrent CVD events (six items), perceived barriers to adopting healthy behaviors for the secondary prevention of CVD (nine items), and the perceived cues or influence by a significant other to perform the recommended behaviors (four items) (Goong et al., 2016). Each subscale was measured using a 5-point Likert scale ranging from strongly agree (5) to strongly disagree (1). Elevated scores on constructs, such as perceived susceptibility and severity, typically indicate that individuals perceive an increased risk of a health ailment and perceive the ailment to be more severe, potentially enhancing the propensity for adopting preventive measures.
Similarly, higher scores on perceived benefits indicate that individuals perceive greater advantages to engaging in preventive behaviors, while higher scores on perceived barriers suggest that individuals perceive more obstacles to engaging in these behaviors. Cues to action scores reflect the influence of external factors, such as healthcare provider recommendations or media campaigns on individuals’ motivation to engage in preventive behaviors. Finally, higher scores on self-efficacy indicate greater confidence in one's ability to successfully engage in preventive behaviors. The validity and the reliability of the instrument have been supported in previous studies in which all constructs met the minimum Cronbach's coefficient reliability of 0.70, and the convergent validity was significant at the 0.001 level (Ban & Kim, 2020; Ştefănuţ et al., 2022). The current study calculated the reliability through a test–retest on 20 patients with previous MI history. The Cronbach's alpha score was 0.73 for perceived susceptibility, 0.65 for perceived severity, 0.61 for perceived benefits, 0.68 for perceived barriers, and 0.80 for the cues to action subscale.
Physical Activity Measurement
The participants’ engagement in regular exercise was examined to evaluate the current activity level and its impact as an independent variable on the patient level to adopt healthy behavior. The Godin Leisure-Time Activity Questionnaire (Godin & Shephard, 1985) was utilized. It is a self-administered seven-day recall questionnaire with three levels of exercise: strenuous, moderate, and mild. The participants stated how often per week they engaged in these three exercise levels for 15 min or more during their free time. It also investigates the weekly frequency of their engaging in a sweat-inducing activity. The total activity score was calculated by multiplying the weekly frequencies of strenuous, moderate, and mild activities by 9, 5, and 3, respectively, and then summed together to measure the total leisure activity. A score ≥ 14 on the GLTEQ classified the patient as active (moderately, at least), and patients who scored < 14 were classified as insufficiently active (Godin & Shephard, 1985). The instrument's reliability across different populations has been well-established (Fattahi et al., 2021; Sari & Erdogan, 2016; Sikes et al., 2019). In the current study, the scale showed good internal consistency, and Cronbach's alpha of the scale was 0.876.
Behavioral Intention Measurement
The dependent variable in this study was the participants’ intention to adhere to the recommended behaviors, including exercise activity, healthy diet, and smoking cessation. This intention was measured using a Likert scale ranging from 1 (very unlikely) to 5 (very likely) (Ajzen, 1991, 2002). The total score of behavior intention ranged from 3 to 15; a score ≥ 8 is considered to be a high intention to adhere to the recommended behaviors, and a score < 8 means they are less likely to adhere to the recommended behaviors. Previous research has upheld the validity and reliability of this instrument (Carpenter, 2010; Fishbein & Ajzen, 1977; Jayanti & Burns, 1998). In the current study, the Cronbach's alpha of the scale was 0.858.
Tool Translation
The tools were distributed in two languages, Arabic and English. The Arabic version resulted from back translation with three bilingual experts in health-related fields. Initially, the English version was translated into Arabic, and then back to English. The two versions were compared to the original content. The back translation experts (n = 3) did not find any translation discrepancies; thus, the tool was deemed appropriate to use.
Ethical Considerations
The Ministry of Health and Prevention (MOHAP/DXB-REC/No. 9 2020) approved the study and the individual hospital where it was conducted. All participants were assured that this research was confidential, and there was no personal risk involved. Moreover, participants were given a copy of the informed consent prior to participating in the study. The signed consent form was then obtained from each participant. They were assured that participation in this study was entirely voluntary, and that they could withdraw at any time. Generally, the confidentiality was assured by replacing identified names with codes. At the completion of the study, the outcomes and results were reported as group data. All of the project details and data were kept in a locked file box in a secure office.
Statistical Analysis
The data were analyzed using SPSS for Windows, version 24. In addition to the descriptive analysis, Pearson's correlation coefficient was conducted to evaluate the association between the participants’ belief perception and the intention to adhere to healthy behaviors. The difference in the intentions based on the subjects’ general characteristics was analyzed using the independent t-test and one-way analysis of variance (ANOVA). The factors influencing health behavior intention were analyzed using multiple linear regression. A dummy variable was created for the categorical variables, and the first regression model was created using the variables that showed a significant association with intention in the univariate analysis. HBM concepts were added in the second model to determine the predictive value of HBM on behavioral intention. The researchers verified that all necessary assumptions of linear regression were met, including linearity, independence of errors, homoscedasticity, normality of residuals, absence of multicollinearity, and absence of significant outliers to ensure the appropriateness and reliability of the multiple regression analysis conducted in this study.
Results
Sample Characteristics
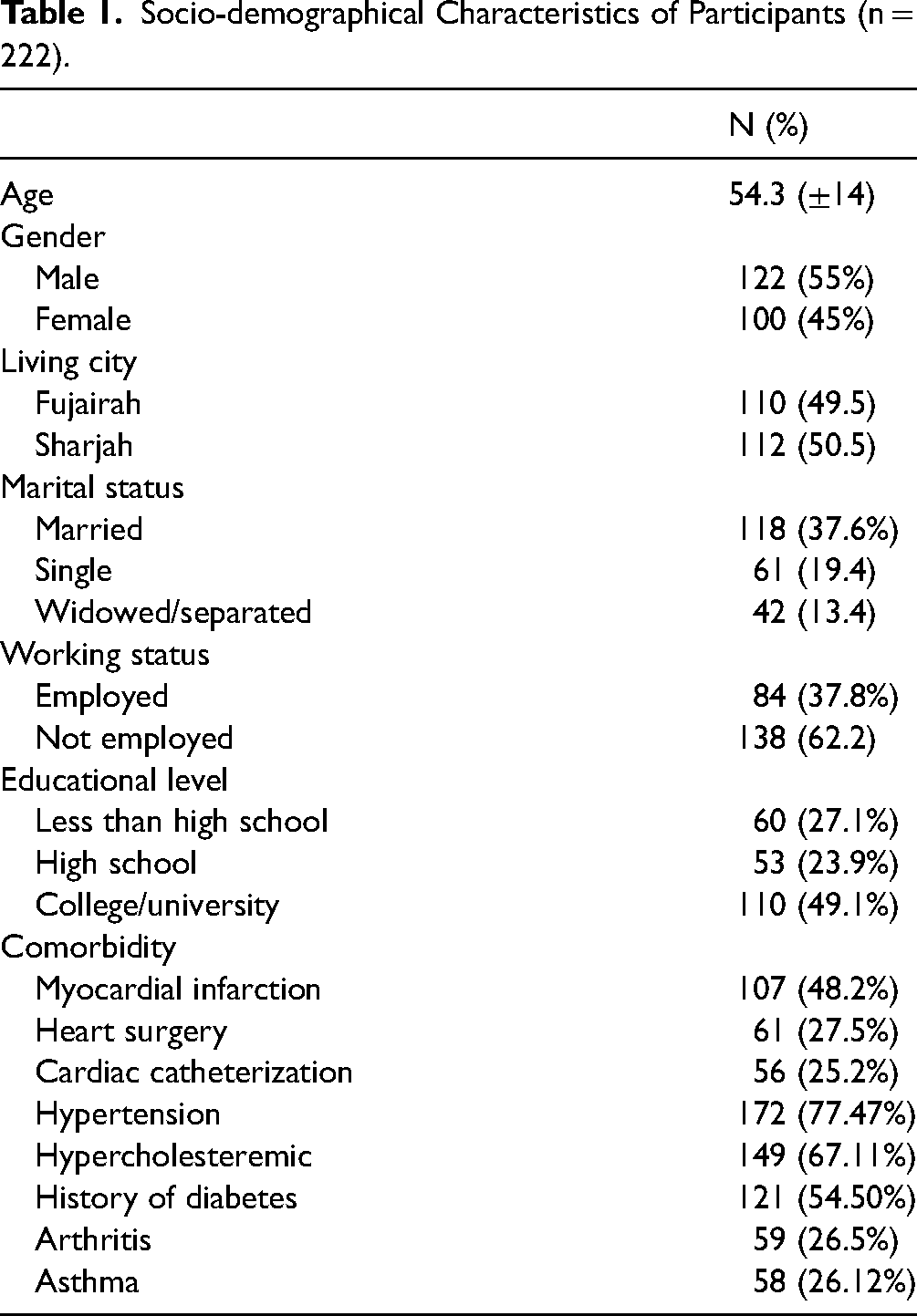
Of the 265 patients who were invited to participate in the study, 43 patients declined participation or returned the questionnaire with more than 35% missing items, while 222 participants were included in the final analysis (response rate: 83.7%). Table 1 shows the details of the participant characteristics. The mean age of the participants was 54.3 years old (SD = 14), ranging from 20 to 86 years old; 55% of the participants were male, and 37.6% of them were married.
Socio-demographical Characteristics of Participants (n = 222).
Current Healthy Behavior
According to the BMI categories, 43% of the participants were overweight, and 32.4% of them were obese (Table 2). Most participants were smokers (56.3%) and were not on a regular diet to reduce the risk of heart disease (65%). The golden leisure score indicated that 70% of the participants were active, and 50% were often engaged in regular, effective exercise activity.
Association Between Health Beliefs and Behavior Intentions (n = 222).

Pearson's correlation coefficient.
Perception of the Health Belief Model and Intentions Toward Behavioral Change
From the average score of the HBM subscales, the mean perceived susceptibility score was recorded at 4.02 (SD = 0.714), reflecting a heightened level of perceived susceptibility among participants. The mean perceived benefits score stood at 4.30 (SD = 0.817), indicating a substantial level of perceived benefits associated with adopting healthy behaviors among participants. Furthermore, the mean perceived severity score totaling to 3.16 (SD = 0.982) indicates a moderate level of perceived severity of CVD among the respondents. Finally, the mean perceived barriers score stood at 3.42 (SD = 0.623), indicating a moderate level of perceived barriers to performing preventive behaviors among participants (Table 2).
Overall, the participants reported a high level of intention to adopt healthy behavior (M = 10.44, SD = 2.50). The participants had a higher intention to perform regular exercise (M = 3.75, SD = 1.05) and adhere to a healthy diet (M = 3.52, SD = 1.19). The lowest intention was toward smoking cessation (M = 3.16, SD = 1.27). The associations between the HBM and the patient's intentions toward adopting healthy behaviors are presented in Table 2. Participant intention is associated positively with susceptibility (r = .343, p < .001), perceived benefits (r = .283, p < .001), and cue to action (r = .547, p < .001). This indicates that the participants who perceived themselves as at a higher risk of CVD and perceived more benefits and social support had higher level of intention to adhere to self-care behaviors.
Differences in Behavioral Intention Based on the Participant's Characteristics
The participants with higher BMI scores were more likely to adhere to the health behaviors (r = .238, p = .001) (Table 3). The independent t-test showed that high intentions toward behavior change were significantly found among the patients with a history of MI and cardiac surgery. The results of the one-way ANOVA revealed that the participants with less than a high school education held higher intentions than those educated to college level (F = 4.967, p = .002). The participants who were currently engaged in less regular exercise (golden leisure score < 15) had a significantly higher intention to adhere to healthy behavior compared to the participants who were currently considered to be sufficiently active (golden leisure score > 15).
Differences in Behavior Intention by Demographic and Clinical Characteristics.
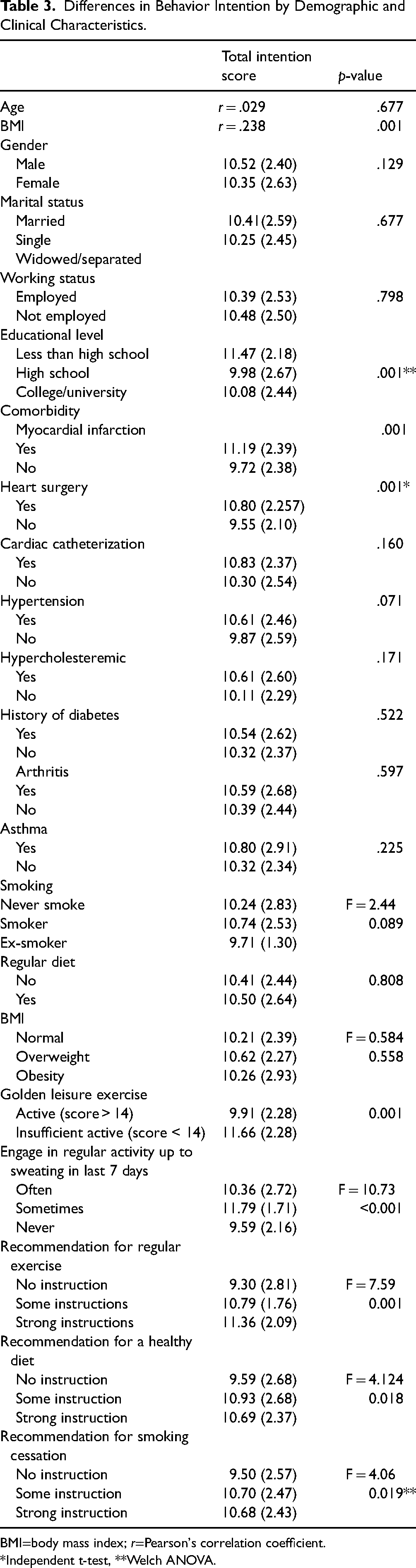
BMI=body mass index; r=Pearson's correlation coefficient.
*Independent t-test, **Welch ANOVA.
Predictors of Behavioral Intention
Multiple linear regression was performed, and the first model was structured using the significant factors revealed from the univariate analysis in Tables 3 and 4. The model shows that participants’ socio-demographic and clinical characteristics predict 25% of the total intention variances (F = 7.17, p < .001). Being sufficiently active (β = 0.304, p < .001), having no history of heart surgery (β = 0.155, p = .02), not performing regular sweating exercises (β = 0.230, p < .001), and not receiving smoking cessation instructions (β = 0.214, p = .005) were the independent predictors for low intention scores.
Regression Coefficients of Independent Variables to Predict Behavior Intention.
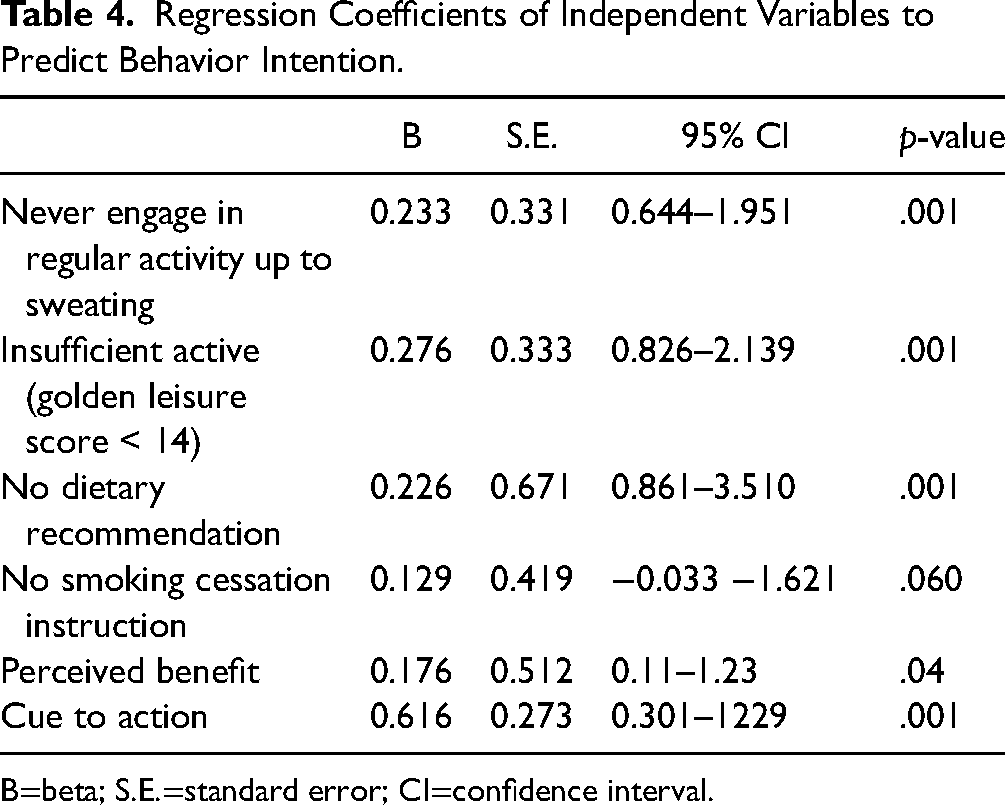
B=beta; S.E.=standard error; CI=confidence interval.
To evaluate the predictive value of the HBM, the significant HBM concepts (perceived susceptibility, perceived benefit, perceived cues to action, and the total HBM score) that are shown in Table 3 were added to the second regression model. The model explains 47% of the intention variances (F = 9.76, p < .001). Perceived benefit and perceived cue to action from the HBM were determined to be significant independent predictors of behavior intention and were responsible for a 22% increase in participant intention.
Discussion
This study examined the predictive value of HBM in predicting the patients’ intention to adhere to self-care behaviors (performing regular exercise, being on a regular healthy diet, and ceasing smoking). The participants had a high level of perceived risk of CVD and its complications (perceived susceptibility). Simultaneously, the participants had a high level of perceived benefits of self-care behaviors (perceived benefit). The HBM suggests that a person must feel susceptible to disease to change their behavior (Lim et al., 2021). The previous research has found that the perceived susceptibility and benefits suggest a low knowledge of disease outcomes and preventive behaviors (Der Ananian et al., 2018; Kim et al., 2021; Lim et al., 2021). Poudel's study showed that adults who performed more than two activities for health promotion had a better knowledge of CVD and perceived themselves as having more susceptibility. Thus, a person who engages in more physical activity is perceived as having a higher knowledge of CVD than those who do not (Poudel & Sumi, 2017). Previous studies have found similar results among various patients with CVD (Habibzadeh et al., 2021; Ma, 2018). These studies focused on increasing the patients’ knowledge about the CVD risk factors and the benefits of CVD self-care behaviors.
The results of the multivariate analysis revealed that the perception of the benefits and cues to action based on HBM were the independent predictors for high intention and were responsible for a 22% increase in participant intention. A previous study found a more substantial predictive power related to self-care behaviors based on the HBM. For example, Chang and Lee (2015) found that the HBM accounts for 57.0% of the variance in self-care behaviors. Other researchers have found that the HBM explains 47% to 55% of the variance in adherence to physical activity for patients with hypertension (Ma, 2018; Sun et al., 2016).
Cue to action reflects a strong belief in the support from the different parties, such as the health care team, family members, and friends, to adhere to the self-care behaviors. The results of this study suggest that patients who perceived the benefits and perceived cues were influenced by their significant others to engage with the recommended self-care behaviors and were more likely to adhere to them. This result is comparable with a recent study by Amdemariam et al. (2022), who found that the cues to take action predictor are related to CVD prevention activities among general health people (Amdemariam et al., 2022). Earlier data on Healthcare Network of Tehran employees showed that cues to action significantly influenced the respondents’ engagement in CVD preventive health behaviors (Rahmati-Najarkolaei et al., 2015). According to the HBM, the perceived benefit promotes health behavior. This study also shows that the perceived benefit was related to the intention to adopt self-care health behaviors. However, some of the emerging results from this study are unexpected. After controlling for the participant characteristics and the perceived HBM constructs, susceptibility was found to be an insignificant predictor. This is not in line with the results from previous studies where participants with a high level of susceptibility perception were more likely to perform self-care (Kim et al., 2021; Poudel & Sumi, 2017). Other studies have found that perceived susceptibility and seriousness might play a significant role in seeking medical help among young adults with chronic diseases (Luquis & Kensinger, 2019).
There is no consistent agreement on the predictive value of the HBM concept between studies. This variation could be related to the variation in the socio-demographic context between studies and chronic diseases. Moreover, some studies were limited to only a few HBM concepts. For example, Luquis and Kensinger only examined perceived susceptibility and perceived seriousness. Other studies have not examined the association between self-care behaviors and actions among adults with hypertension (Ma, 2018). The result of this study is incomparable with previous literature as no study has examined the association between the intention of self-care behavior and HBM among CVD patients in the Middle East, particularly in the UAE. Therefore, the current study is the first conducted in Gulf countries engaging multiple cultural populations. However, when it comes to comorbidity and clinical characteristics, it was found that having no history of heart surgery (β = 0.155, p = .02) was the independent predictor for low intention scores. This would suggest that those patients with comorbidity will likely have a stronger intention to adopt a healthy lifestyle than their counterparts.
The study enriches the existing literature by raising intriguing questions about the interplay between health beliefs, past medical encounters, and prospective health behaviors, particularly in the post-COVID period. One possible explanation revolves around the constructs of perceived vulnerability and personal significance. Individuals who have undergone cardiac surgery might have faced a substantial health crisis prompting a heightened commitment to health priorities and a more rigorous adherence to self-care regimens. In contrast, those lacking such experiences may perceive themselves as less susceptible to cardiovascular ailments and may not feel the same urgency to engage in preventive behaviors. Moreover, individuals with no history of cardiac surgery may lack direct exposure to the challenges and repercussions of cardiovascular diseases, resulting in a diminished sense of urgency towards preventive measures.
Additionally, psychological factors, such as denial, apprehension, or aversion to confronting health hazards, could influence the inclination toward adhering to self-care practices. Given the heightened health consciousness in the post-pandemic era, it is imperative to discern these subtleties and tailor interventions to accommodate individuals’ distinct motivations, barriers, and risk perceptions. Healthcare professionals are pivotal in imparting awareness about the significance of preventive behaviors and aiding patients in embracing healthier lifestyles, irrespective of their medical histories.
Despite the high intention toward self-care behavior found in this study, the self-report of current behavior revealed a high percentage of participants who were smokers (56%), who were not on a regular healthy diet (65%), and 75% who had an abnormal BMI (obese or overweight). These findings are particularly concerning in the context of the post-COVID-19 pandemic, where individuals with cardiovascular disease (CVD) confront elevated risks of complications. The intention is essential to self-management behavior, but will not grant the commitment needed to transform intention into action. Previous studies have found that long-term follow-ups and encouragement are required to shift intention into action (Mohammadi et al., 2018).
In addition, the previous literature suggests that the level of education is a significant predictor of CVD self-care behavior: the higher the education level, the better the knowledge about CVD, and the better chance of long-term adherence to self-care behavior (Allegrante et al., 2019; Amdemariam et al., 2022; Habibzadeh et al., 2021; Kim et al., 2021; Ma, 2018). Educational instructions for a healthy diet before hospital discharge predicted the participants. These expected results should be interpreted with caution as there is no standard formal education program for CVD patients across the UAE health services. Previous studies found a strong positive correlation between educational interventions, such as cardiac rehabilitation and the intention to engage in healthy behaviors (Jung & Yang, 2021; Kim et al., 2021).
Strengths, Limitations, and Recommendations
The researchers were unable to collect data while supervising the behavior. However, the previous meta-analysis found a substantial effect size regarding the association between actual behavior and intention (Rich et al., 2015). It is recommended that future research use a longitudinal design to determine the association between intention prior to hospital discharge and the level of adherence to self-care behavior after hospital discharge. This is an important issue where the HBM does not offer room to uncover the sociocultural factors in a diverse population.
Univariate analysis revealed that participants reporting lower current activity levels tended to exhibit higher initial intentions. Nevertheless, the influence of physical activity could potentially complicate the association between the HBM factors and behavioral intention. Those with lower activity levels may perceive greater benefits from exercise, thus initially expressing a stronger intention to become more active. This initial intention, however, might not necessarily translate into long-term behavioral changes as captured by the HBM factors. Alternatively, it is possible that strong initial intentions for healthy behaviors might lead someone to start exercising more; yet, without clear perceived benefits or clear cues to action, they might struggle to maintain these behaviors over time. Moving forward, it is imperative for future research to delve into the intricate interplay among physical activity, HBM factors, and behavioral intention, thereby addressing potential confounding variables comprehensively.
Implications for Practice
The study results highlight the possible impact of an education program on self-care behavior intention, which suggests the need for future research to examine the effect of follow-up educational programs on long-term adherence to self-care behavior. Such programs need to be culturally sensitive, considering the religious beliefs of a diverse population in the UAE. Following the COVID-19 pandemic, people with comorbidities who have CVD require more complex clinical care. Healthcare systems are now faced with the intricate challenge of managing the unique complexities arising from the convergence of CVD and the lingering impacts of the pandemic. Consequently, there is an urgent need for tailored clinical protocols that account for the distinctive circumstances of CVD patients in the post-pandemic era. According to recent research, it is critical to adapt management approaches to align with the evolving needs and intricacies of CVD patients, taking into account each person's individualized risk profile, medical histories, and potential sequelae stemming from COVID-19.
Conclusion
This study explored the characteristics of individuals with CVD post-COVID pandemic who expressed strong intentions for adopting healthy behaviors. Interestingly, initial intentions seemed to be higher among those with a higher body mass index, lower education level, and lower current activity levels. However, regression analysis revealed that perceived benefits and clear cues to action, as defined by HBM, were the strongest independent predictors of behavioral intention in this post-COVID CVD population. These HBM factors explained a substantial 22% more of the variance in intention scores compared to sociodemographic and clinical characteristics alone.
These findings suggest that for individuals with CVD recovering from COVID-19, initial intentions to improve health behaviors may not fully translate to long-term commitment. Therefore, interventions designed for this specific population should prioritize fostering a strong understanding of the personal benefits of healthy behaviors and provide clear prompts for action. Tailoring communication strategies based on individual characteristics, such as education level or current activity level, may further enhance the effectiveness of such interventions in promoting healthy lifestyle changes among this vulnerable population.
Footnotes
Acknowledgments
The authors acknowledge all the participants of the study.
Data Availability
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The datasets during the current study are confidential and available from the corresponding author on reasonable request.
Ethical Statement
Ethical approval was sought from the Ministry of Health (MOHAP/DXB-REC/JJF/NO.9 2020), then from the designated hospital.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.