
Abstract
Introduction
Sleep is one of the most crucial basic human needs in Maslow's hierarchy, while sleep disorders are the most commonly occurring complications of chemotherapy.
Objective
This study was conducted to determine the effect of progressive muscle relaxation techniques on the sleep quality of patients with cancer undergoing chemotherapy.
Methods
This study was a randomized clinical trial performed on patients with cancer undergoing chemotherapy. Ninety cancer patients were selected by the convenience sampling method and randomly assigned into two groups; the progressive muscle relaxation group and the control group. Before the intervention, the Pittsburgh Sleep Quality Questionnaire (PSQQ) was completed for patients in both groups. In the intervention group, progressive muscle relaxation was performed for 4 weeks (twice daily and 20 min each time). In the control group, patients only received routine care. After the intervention, the PSQQ was completed again for patients in both groups. The data were analyzed using SPSS version 23.
Results
The mean and standard deviation of age were 45.95 ± 10.26 years. The samples of the intervention and control groups were homogeneous in terms of demographic characteristics. The results showed a significant improvement in the Pittsburgh Sleep Quality Index in the intervention group before and after the intervention (P < .001, Z = 5.09). However, this rate was not different in the control group. The sleep level of the intervention and control groups was not different at the beginning of the study. However, at the end of the study, the sleep score in the intervention group had decreased significantly (P < .001, Z = 3.52).
Conclusion
The results of the present study showed that progressive muscle relaxation improves the sleep quality of patients with cancer undergoing chemotherapy. Therefore, relaxation can be considered a useful and effective intervention for improving sleep quality of patients with cancer.
Introduction
Sleep is one of the most important elements in the circadian rhythm, which is accompanied by the rehabilitation of physical and mental abilities (Eugene & Masiak, 2015), and in Maslow's hierarchy of needs, it is one of the most basic human needs (Hale et al., 2019). Furthermore, sleep is an integral part of human life and one of the most important biological cycles that relieves fatigue and makes people ready for daily activities. Human health at any age is associated with the quantity and quality of sleep (Dehghan Nayeri et al., 2012). More than 30% of human life is in the process of sleep (Wolk & Somers, 2007). With the changes in human lifestyle in recent decades, sleep disorders are increasingly on the rise in today's societies and millions of people suffer from these disorders (Anothaisintawee et al., 2016). More than 30% of the world's population suffers from sleep disorders (Eugene & Masiak, 2015). Research has shown that sleep deprivation causes impaired immune function and decreased hypothalamus, pituitary, and adrenal function during the following days; decreased glucose tolerance; increased blood pressure and increased risk of cardiovascular problems independently; and decreased activity level, personal aptitude, and anaerobic strength (Bagheri et al., 2007).
Cancer is the second leading cause of death in the United States and the third leading cause of death in Iran. According to the estimations of the World Health Organization (WHO) in 2009, the number of patients diagnosed with cancer is increasing from 11.3 million in 2007 to 15.5 million in 2030. In Iran, according to the statistics in 2008, about 70,000 new cases of cancer have been diagnosed annually and its prevalence is 200–250 thousand patients. New cases of cancer in Southeast Asia have increased from 1.3 million in 2002 to 2.1 million in 2020 (Mousavi et al., 2009). Treatments of cancer are associated with complications and toxicity that can endanger the quality of life of a person in the short term or long term (Quinn, 2008). Surgical methods, radiation, chemotherapy, or hormone therapy may be used to treat cancer based on the stage of cancer and medical history (Coles et al., 2018). One of the cancer treatments is chemotherapy, which is used to destroy cancer cells. Chemotherapy is an essential treatment method, but it can have serious side effects for the patient. Studies showed that chemotherapy is associated with several complications such as fatigue, nausea, vomiting, anemia, alopecia, and sleep disorders (Jalali et al., 2016).
Sleep disorders are one of the paramount clinical problems in patients with cancer. The prevalence of this disorder in patients with cancer is almost three times that of the normal population in society, and they have poorer sleep quality compared to other patients. That is why it has become a serious challenge for treatment in this population of patients (Coles et al., 2018; Jalali et al., 2016). In the Jalali et al. study, sleep disorder was reported in 51.4% of patients undergoing chemotherapy (Jalali et al., 2016), and in the Mansano et al. study, it was reported in 9.62% (Mansano-Schlosser & Ceolim, 2012). Also, this disorder was reported in 52% of these patients in the Chen et al. study (Chen et al., 2008) and 56.6% in the Gooneratne et al. study (Gooneratne et al., 2007).
Adequate sleep is essential for the growth, evolution, and survival of patients diagnosed with cancer. Many cancer patients require more sleep to improve the organization of their immune system. Unfortunately, the treatment of sleep disorders in these patients is not given the attention it deserves (Jalali et al., 2016). Both pharmacological and nonpharmacological methods can be utilized to address sleep disorders (Karadag et al., 2017), and benzodiazepines are the most common drugs used (Kanji et al., 2016). The use of short-acting and medium-acting benzodiazepines for 1–2 weeks can lead to drug resistance, which can cause symptoms such as anxiety, dizziness, insomnia, and cognitive and perceptual changes in patients when abruptly discontinued. Long-term use of these drugs is associated with drug dependence and drug tolerance (Johnson & Streltzer, 2013). Therefore, nonpharmacological methods are useful. Approved nonpharmacological treatments (light therapy, relaxation techniques e.g., yoga, hypnotherapy, and complementary medicine) are mentioned (Jankovic et al., 2021). Nonpharmacological methods that are referred to as complementary therapies are safer than pharmacological methods and have fewer side effects than them (Kauffmann et al., 2018). The fear of drug side effects may be a reason for the increased use of complementary medicine by patients (Mohammadpour et al., 2013).
One of the most common forms of complementary therapies is the progressive muscle relaxation technique, which has been considered in contemporary nursing as a nursing procedure (Charalambous et al., 2016; Novais et al., 2016). Progressive muscle relaxation was introduced and used by Jacobson in 1938. Progressive muscle relaxation is an active technique that makes the patient feel calm by actively contracting and then relaxing specific muscles progressively (Yoo et al., 2005). Jacobson stated that muscle relaxation leads to mental relaxation (Roozbahani et al., 2017). On the other hand, it increases the activity of the parasympathetic cycle, which in turn neutralizes and reduces muscular tension and can effectively reduce stress, sleep disorders, mood disturbances, and fatigue symptoms in patients suffering from cancer (Conrad & Roth, 2007).
Review of Literature
Numerous studies have been conducted on the effectiveness of progressive muscle relaxation techniques, which have shown that receiving this strategy improves sleep quality (Rahmatpour et al., 2019). Additionally, muscle relaxation can relieve migraine pains (Keyghobady & Asadi, 2000), reduce stress, and improve cardiac function in patients with cardiovascular disorders (Chaudhuri et al., 2016). However, it does not affect menstrual pain in women (Asgariani et al., 2018). In some studies, the effect of progressive muscle relaxation on patients with cancer has been evaluated. In a study conducted by Yoo et al. in 2005 on 60 patients with breast cancer undergoing chemotherapy in South Korea, the results showed that progressive muscle relaxation does not affect the quality of life of these patients (Yoo et al., 2005). Similarly, a study conducted by Bordeleau et al. in 2003 on patients with metastatic breast cancer, concluded that relaxation exercises do not affect the quality of life of these patients (Bordeleau et al., 2003). However, In Shariati et al. study in 2010, the effect of relaxation on the quality of life of 25 patients with breast cancer undergoing chemotherapy was evaluated and the results showed that relaxation can be an effective, convenient, and affordable method to improve the quality of life in this population of patients (Shariati et al., 2011). In a systematic review by Samuel et al. (2021), which assessed three randomized clinical trial (RCT) studies on the effect of relaxation therapy, it was concluded that there is a lack of statistically significant evidence regarding the efficacy of relaxation therapy on the sleep of cancer survivors. Furthermore, there was a noted deficiency in authentic evidence supporting this purpose. Therefore, the authors suggested conducting more clinical trials (Samuel et al., 2021).
Charalambous et al. believe that the relaxation technique is one of the nursing interventions that can be effective, convenient, and can be considered a complementary therapy (Charalambous et al., 2016). However, few studies have investigated its effects on the sleep of patients with cancer undergoing chemotherapy. Thus, this study was conducted to determine the effect of the Jacobson relaxation technique on the sleep quality of patients with cancer undergoing chemotherapy.
Methods
Design and Population
The present study was a RCT which was accomplished in October 29, 2018 to October 24, 2019. The study population consisted of all patients with cancer undergoing chemotherapy who were referred to oncology departments. Based on the required relationship for determining the sample size, we considered a confidence level of 95% (α = .05), the success rate in the population (P), and the estimation accuracy (ε) to obtain the desired sample size. In this case, α/2 was equal to .025 and Z 0.025 was equal to ±1.96 with P being .5 and ε being 0.1. Thus, the sample size was determined to be 96, and we considered a total of 100 samples for data gathering.
Inclusion and Exclusion Criteria
The inclusion criteria were age between 18 and 65 years, informed consent to participate in the study, full consciousness, obtaining a score equal to or more than 5 from Pittsburgh Sleep Quality Index (PSQI) questionnaire, communicating verbally with the researcher, undergoing chemotherapy based on the treatment protocol, acceptable hearing and speaking ability to learn relaxation techniques, having the literacy in reading and writing and the possibility of using educational compact disc (CD), not having any of known mental illnesses such as anxiety and severe depression, having a minimum of one month of chemotherapy history or a minimum of two chemotherapy sessions, and not undergoing any other treatment at the same time as chemotherapy (such as radiotherapy or hormone therapy). Patients` death, deterioration of the patient's condition during the study, not performing intervention for more than three sessions, and lack of patient's willingness to continue cooperation were exclusion criteria.
Data Collection
For data collection, the researcher explained the aims of the study for patients who met the inclusion criteria. Those who were willing to participate entered the study after being explained the process and obtaining informed written consent. In the next step, by using the randomization method, the samples were allocated as follows: numbers 1–100 were placed inside a container and the patient was asked to randomly select a number, so that the even number was allocated to the intervention group and the odd number to the control group. Patients were divided into two groups: the intervention group and the control group (each with 50 subjects).
In this study, data collection instruments included a demographic information questionnaire and sleep quality index. The PSQI questionnaire was used to determine sleep quality. PSQI questionnaire is a standard instrument whose validity and reliability have been confirmed in various studies. The internal consistency of the questionnaire using Cronbach's α coefficient is reported as .83. This is a self-report questionnaire that examines sleep quality over the past month. The validity of this instrument has been confirmed in different studies (Sohn et al., 2012). In the Reza et al. study (2010), the reliability of the questionnaire was 0.88 (Reza et al., 2010). This questionnaire consists of nine questions, but question number 5 has 10 subquestions. Therefore, in total, this questionnaire has 19 questions that are scored on a 4-point Likert scale from 0 to 3. The PSQI has seven subscales, including 1, subjective sleep quality; 2, sleep latency; 3, sleep duration; 4, sleep efficiency; 5, sleep disorders; 6, use of sleeping pills; and 7, daytime dysfunction. Each subscale score ranges from 0 to 3. A score of 3 indicates a severe problem. The sum of the scores of the seven subscales forms the total score, which ranges from 0 to 21. A total score of 5 or more indicates poor sleep quality (Reza et al., 2010).
After obtaining written approval from the authorities of oncology centers and hospitals, the researcher referred to the selected hospital and obtained the written consent of the authorities and oncologists and nurses of the relevant center by presenting the letter of introduction. Then, the first researcher referred to the oncology department and clinic of the hospital introduced herself and stated the aims of the research. After that, the researcher identified the patients with cancer undergoing chemotherapy who met the inclusion criteria. Finally, after obtaining informed consent from these patients, they were asked to fill out the demographic and PSQI questionnaires.
Intervention
To perform the interventions, patients in the intervention group received two 45-min individual in-person sessions by the first author (who has been an experienced nurse for 5 years) to learn progressive muscle relaxation techniques, with a 2-day interval between sessions. In the present study, in order to perform progressive muscle relaxation techniques, the patients were asked to focus on each group of muscles from the legs to the head for 5–10 s to contract them slowly and then relax them for 10–15 s and focus on the emotions that arise in the body at each stage after relaxation (Saeedi et al., 2012). This method is usually feasible for 20 min. A CD containing relaxation steps was provided for the patients in the intervention group, and they were asked to perform relaxation exercises twice a day for four weeks according to the scheduled program at home. Specifically, one of the relaxation sessions should be performed definitely before bedtime. During this period, the researcher regularly monitored the progress of work through in-person visits and follow-up calls. In the final evaluation, those patients who did not participate more than three scheduled sessions were excluded from the study. In the control group, no specific intervention was performed, and the patients were only evaluated before and after the intervention using data collection instruments. After the end of the intervention period of 4 weeks, the PSQI questionnaire was given to the samples again, and the obtained scores before and after the relaxation training were examined in both groups.
Ethical Consideration
The study received approval from the research ethics committee of the Kermanshah University of Medical Sciences under numbers IR.KUMS.REC.1397.135, and all methods were conducted following the guidelines and regulations outlined in the Declaration of Helsinki. Before the interviews, written informed consent was obtained from all participants or their legal representatives.
Data Analysis
Data analysis was performed using SPSS 23 statistical software. Descriptive statistics were utilized to report the demographic characteristics of the samples, while the chi-square test was employed to compare the demographic information in both groups. The effect of relaxation on the total sleep quality score was determined using the Wilcoxon test. Additionally, the Mann–Whitney U test was used to compare the two groups before and after the intervention. The significance level of the analytical tests was considered as .05.
Results
Sample Characteristics
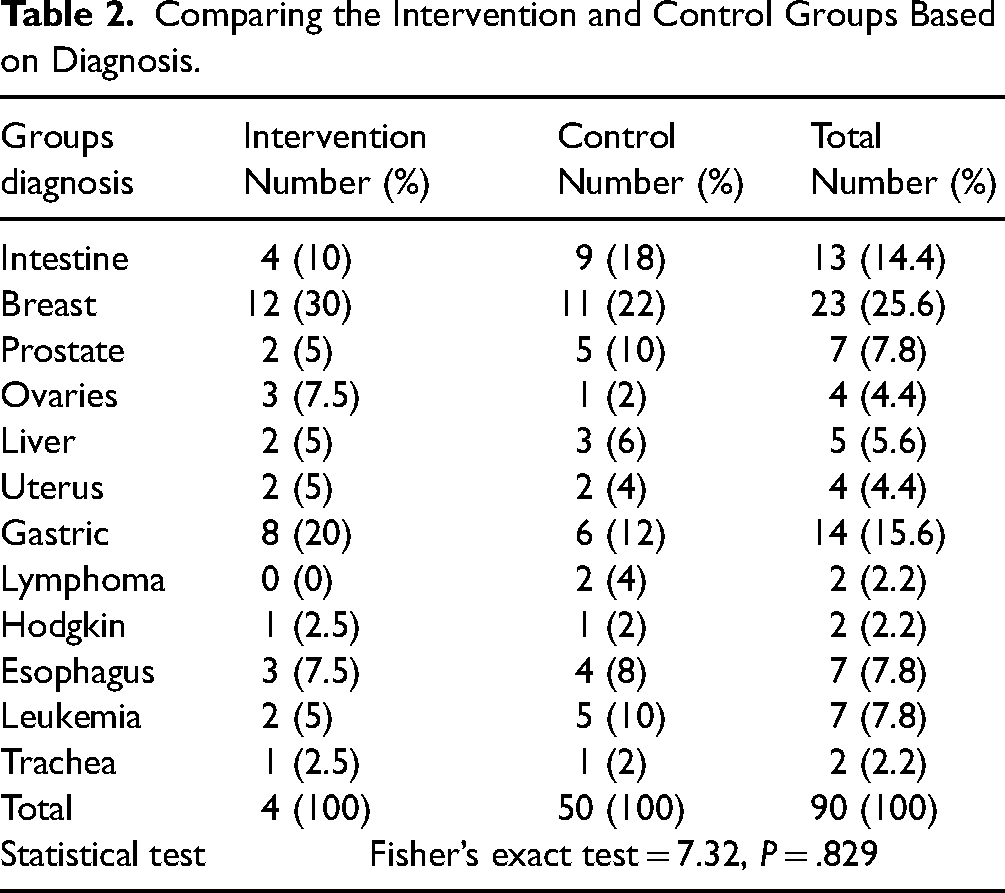
In the present study, the sample size was 100. The intervention group and the control group consisted of 40 and 50 patients, respectively. Ten patients from the intervention group were excluded from the study due to deterioration of their condition, hospitalization, and not participating in more than three intervention sessions. The samples were in the age range of 21–64 years, with a mean and standard deviation of age of 45.95 ± 10.26 years. Almost 84% of patients (76 patients) were married, 62.2% of them (56 patients) were female, 80% (72 patients) had no history of using sleeping drugs, 47.8% (43 patients) were housewives, and 28.9% of the patients (26 patients) had a history of drug abuse. The results of the chi-square test for demographic variables showed that there is no difference between the two groups in terms of demographic variables (Table 1). Most of the patients (25.6%) were diagnosed with breast cancer, and there was no significant difference between the two groups in this variable (P = .829) (Table 2).
Comparison of Demographic Information of the Study Samples in the Intervention Group and the Control Group.

Comparing the Intervention and Control Groups Based on Diagnosis.
Research Aim Results
Considering that the two groups were independent and had abnormal distribution, the Mann–Whitney U test was used to compare the two groups in terms of sleep quality before the intervention. Accordingly, there was no significant difference between the two groups in terms of the Pittsburgh sleep variable before the intervention, but after the intervention, sleep quality improved in the intervention group (P < .001, Z = 3.52) (Table 3).
Comparison of the Two Groups in Terms of Sleep Variables Before and After the Intervention With Mann–Whitney U Test.

* indicates significant value.
Furthermore, based on the Wilcoxon test in the intervention group, PSQI improved after the intervention compared to before the intervention, but this rate was not significant in the control group (Table 4).
Comparison of Before and After of the Intervention and Control Groups in Terms of Sleep Variable With the Wilcoxon test.

Discussion
In the present study, the effect of progressive muscle relaxation techniques on the sleep quality of patients with cancer undergoing chemotherapy was investigated. Results showed that progressive muscle relaxation techniques are effective in improving the sleep quality of these patients. This finding is consistent with the results of Saeedi et al. study that showed that muscle relaxation methods can reduce sleep disorders in patients with renal failure (Saeedi et al., 2012). Amini et al. study (2016) showed that muscle relaxation techniques as an effective intervention reduce anxiety, fatigue, and sleep disorders in parents of children with leukemia undergoing chemotherapy (Amini et al., 2016), which is consistent with the results of the present study. In other words, relaxation training can reduce anxiety and psychological and physical stress, and by increasing parasympathetic system activity and reducing sympathetic nervous system stimulation, it improves sleep quality in patients. Since the main cause of sleep disorders among different people is high levels of anxiety and stress, the effectiveness of this intervention in improving the sleep quality of patients with cancer can be explained (Keyghobady & Asadi, 2000).
Ducloux et al. (2013) showed that relaxation techniques did not affect sleep quality in patients with advanced stages of cancer (Ducloux et al., 2013), which is inconsistent with the results of the present study. The reason for this inconsistency may be the differences in the type of disease, the stage of cancer, and the treatments. Zupanec et al. (2017) reported the positive effects of progressive muscle relaxation exercises on sleep disorders in children with lymphoblastic leukemia, which is consistent with the results of the present study (Zupanec et al., 2017). Chen et al. (2015) reported that combining guided imagery and relaxation techniques improves sleep quality in patients with breast cancer (Chen et al., 2015), which is in line with the results of the present study. Rambod et al. (2013) and Amini et al. (2016) reported the effectiveness of progressive muscle relaxation exercises on sleep disorders in hemodialysis patients, which is consistent with the results of this study (Amini et al., 2016; Rambod et al., 2013). Demiralp et al. (2010) demonstrated that relaxation techniques reduce fatigue and sleep disorders in patients with breast cancer undergoing chemotherapy (Demiralp et al., 2010), which is in line with the results of the present study. Matourypour et al. (2012) reported that the use of progressive muscle relaxation techniques does not effectively reduce work-related stress in nurses working in the Intensive Care Unit (ICU) as an emotion-focused coping strategy, which contradicts the results of the present study (Matourypour et al., 2012). The reason for the differences in these results is probably due to the differences in the conditions or nature of the disease, the differences in the questionnaires, and the spatial and temporal differences. Roozbahani et al. (2017) stated that relaxation techniques have been effective in the sleep quality of preuniversity students (Roozbahani et al., 2017), which is in line with the results of the present study. Since the main cause of sleep disorders among patients with cancer is high anxiety and tension, it can be possible to reduce anxiety and physical stress in this population of patients by training and performing relaxation techniques. Therefore, the effectiveness of this intervention in improving the sleep quality of patients with cancer can be explained.
There are multiple reasons for the effectiveness of progressive muscle relaxation. Some researchers have examined its effects on the autonomic nervous system and have stated that frequent muscle contractions and expansions lead to the dominance of the parasympathetic tone, resulting in relaxation, and decreased heart rate and blood pressure (Conrad & Roth, 2007). Some researchers suggest that progressive muscle relaxation is effective due to the release of endorphins, reduction of pain, lowered cellular oxygen demand, and decrease of certain metabolic wastes, such as lactic acid (Akmeşe & Oran, 2014). These factors can contribute to an improvement in sleep quality (Costa et al., 2018; Gökşin & Ayaz-Alkaya, 2018).
Strength and Limitations
Our study possesses several strengths, such as a relatively large sample size, randomization, and a 4-week intervention period. However, it also has some limitations, including a notably high attrition rate in the intervention group. Despite this, the demographic characteristics of both groups were statistically similar. Further research on this topic is recommended to corroborate our findings.
Implication for Practice
This study highlights that the Jacobson Relaxation Technique can significantly improve sleep quality in cancer patients undergoing chemotherapy. Given its simplicity and effectiveness, this technique should be integrated into routine care for these patients. Nurses and healthcare providers can easily teach and implement it, providing a valuable tool to enhance patient well-being without additional costs or medications. Encouraging the use of progressive muscle relaxation could make a meaningful difference in the daily lives of those battling cancer. Further studies could explore the long-term benefits and other potential uses of this relaxation technique.
Conclusion
The results of the present study indicated that progressive muscle relaxation can reduce sleep disorders in patients with cancer and improve their sleep quality. Therefore, progressive muscle relaxation can be recommended as a safe, affordable, and convenient method to improve sleep quality in cancer control and treatment programs. Based on the results of this study, it is recommended that the clinical practitioners working in the treatment of patients with cancer pay more attention to nonpharmacological methods such as muscle relaxation techniques in their care programs.
Footnotes
Acknowledgements
The authors of the present study extend their gratitude to the esteemed authorities of Kermanshah University of Medical Sciences. They would also like to thank the nurses of the oncology department at Bustan Hospital, as well as the patients with cancer for assisting them in this research project. This article is excerpted from a master's thesis, which has been approved as a research project at the School of Nursing and Midwifery under the code of ethics: IR.KUMS.REC.1397.135 from the ethics committee of the Kermanshah University of Medical Sciences. Also, it has been registered at the Iranian Clinical Trials Center under the code IRCT20170619034641N 4.
Author Contributions
FSK, AA, AK, and BKP contributed to the study design. Data were collected by FSK, MA, and BKP and analyzed by NS, AN, and MM. The final report and manuscript were written by AA, FSK, AK, AN, and MM and reviewed and approved by all authors.
Availability of Data and Material
The datasets generated and analyzed during the current study are not publicly available due to our institution's regulations but are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Standards
The study received approval from the research ethics committee of Kermanshah University of Medical Sciences under number IR.KUMS.REC.1397.135, and all methods were conducted in accordance with the guidelines and regulations outlined in the Declaration of Helsinki. Prior to the interviews, written informed consent was obtained from all participants or their legal representative.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Deputy for Research and Technology, Kermanshah University of Medical Sciences (grant number 97260).