
Abstract
Introduction
To improve the capacity of diabetic foot ulcer (DFU) patients for self-management of wound care, there is a renewed need for self-care on their part, as well as an increase in their readiness to deal with issues and heal their wounds. Therefore, this review empirically assessed contemporary evidence on how patients with DFU can perform self-treat wound care.
Methods
This integrative literature review assessed how patients with DFU could perform self-treat wound care. Whittemore and Knafl integrative information literature review involved searching four databases (Scopus, PubMed, Web of Science, and Google Scholar), which resulted in 2,595 published articles, between 2010 and 2023. Nineteen articles satisfied the requirements for inclusion and quality assessment, and the PRISMA review checklist was followed.
Results
No research has addressed DFU patients’ self-treatment of wound care. The integration of evidence from quantitative and qualitative studies was achieved in three categories: (1) motivation, (2) self-wound care strategy, and (3) self-wound care performance by DFU patients.
Conclusion
To equip themselves to perform wound care independently, patients with DFU must receive training to clean wounds, apply wound medication, and perform dressings. There is a need for research that develops a self-treat wound care intervention model in patients with DFU.
Introduction
A diabetic foot ulcer is a common complication of diabetes mellitus, a chronic condition characterized by elevated blood sugar levels. This condition specifically refers to open sores or wounds that develop on the feet of individuals with diabetes. Diabetic foot ulcers often occur because of a combination of factors, including nerve damage (neuropathy) and poor circulation. Common causes of DFUs include excessive pressure on the foot, fungal infections, peripheral neuropathy, poor circulation, irritation, and wounds on the feet. Poorly fitting shoes are also a leading cause of foot ulcers (Bell, 2022). The degree of DFU, according to the Meggitt-Wagner system, is grade 0 (a closed wound), grade 1 (shallow wound), grade 2 (wound reached the tendon), grade 3 (abscess formation wound), grade 4 (gangrene has not yet spread), and grade 5 (gangrene has spread) (Onni, 2020). Patients with this condition require intensive and continuous foot care to ensure that the wound heals properly and prevents more severe complications.
Studies have highlighted that DFU foot care is essential for preventing infection and accelerating wound healing (Bakker & Schaper, 2000; Game et al., 2018). However, in research on the motivation and strategies of DFU sufferers in caring for their wounds, patients reported individually that it was crucial for them to develop self-care behaviors to minimize the risk of amputation (Selma & Cingil, 2020). Therefore, reports of consolidated evidence in this area are required. There is a need to understand the motivating factors for people with DFU, the factors that affect the treatment of their foot wounds, and the strategies they use to deal with wound healing problems in terms of knowing what approaches and wound care techniques are practical and performed by the patients themselves. In addition, this information will help DFU patients plan and manage their wounds. A researcher's understanding of the elements that are globally consistent is similarly essential. This integrative literature review summarizes information on motivational wound care abilities, self-efficacy-boosting techniques, and factors affecting their ability to care for wounds (Guest et al., 2018).
Access to necessary medical care is not always easy for patients with diabetic foot ulcers, especially in developing countries or rural areas. High treatment costs, lack of health facilities, and long distances can be barriers for patients to receive proper medical care. Therefore, it is vital to learn how patients with diabetic foot ulcers can properly perform self-treatment of wound care (Alexandrescu et al., 2009).
There is not much clinical foot care advice or self-wound care techniques for DFU patients. There are discrepancies between DFU patients’ beliefs and behaviors and the clinical advice on self-wound care provided by the American Diabetes Association (ADA). (Ploderer et al., 2018). Improvements must be made for self-wound care, and novel approaches are required to involve patients in self-care. Daily maintenance is one of the greatest strategies for preventing foot issues, and preventive treatment is essential (Polikandrioti et al., 2021). Blood sugar management is critical, and other good diabetes management habits such as healthy eating, physical activity, and regular doctor's appointments can also help prevent foot complications.
This review empirically assesses contemporary evidence on how patients with DF U are able to care for their own wounds. Three questions support the review objectives: (1) How do DFU patients motivate themselves to perform self-wound care (2) How do DFU patients perform self-wound care strategies? (3) What is the perception of DFU patients to perform self-wound care? This review is very important to support DFU patients in their progress of wound healing, especially when professional care is not available in their area.
Methods
Design
An integrative review is the best strategy for properly understanding the phenomenon. This research used Whittemore's five-stage integrative review process, which includes (1) problem formulation, (2) data collection or literature search, (3) evaluation of data, (4) data analysis, and (5) interpretation and presentation of results (Whittemore & Knafl, 2005).
The investigation of research evidence and literature from both quantitative and qualitative approaches is a characteristic of the integrative review technique (Toronto & Remington, 2020). To gather evidence regarding the review's stated purpose and aims, both quantitative and qualitative studies were methodically reviewed. Below is a further explanation of the steps and procedures involved in the review.
Search Methods
The initial search for literature was conducted from 2010 to February 2023. Literature was searched from online databases such as Scopus, PubMed, Web of Science, and Google Scholar. The main search terms used in the databases were “diabetic foot ulcer AND self-wound care AND motivation AND strategy.” To guarantee clear reporting of reviews, the PRISMA checklist was used (Appendix A). The process of an integrated review may include the analysis of accumulated research data and literature (Toronto & Remington, 2020).
Inclusion/Exclusion Criteria
Inclusion Criteria
All articles were required to be about DFU patients, they were required to be primary research studies, and they needed to address in combination or separately DFU patients’ motivation, strategy, and self-wound care. Articles published in English between January 2010 and February 2023.
Exclusion Criteria
The following exclusion criteria were used: (1) DFU caused by Peripheral Artery Disease; (2) Patients who have significant neuropathy, retinopathy, or other diabetic issues may find it difficult to take care of their wounds on their own; (3) Patients with significant cognitive or physical impairment, which may affect their ability to understand and perform wound care instructions on their own; (4) Patients with grade 3 and 4 diabetic foot ulcers; (5) There was no published research article; for instance, literature reviews, opinion pieces, editorials, and commentaries were not included.
Selection of Studies
All database search results were exported to the Mendeley reference manager software, and duplicate search results were deleted. Next, a two-step selection process was undertaken by the covidence application. First, three reviewers (NVM, SK, EM) scanned the title and abstract of all articles reporting self-wound care of DFU patients. In the second step, the reviewers screened full text to determine their eligibility. Finally, fully eligible articles were selected for further analysis (Figure 1). Evaluators’ disagreements were resolved via the two reviewers (EY, AY).

PRISMA flow chart covidence.
Data Extraction, Analysis, and Synthesis
The data were extracted using the covidence application. Initially, articles were re-read to gain a comprehensive understanding of their methodologies and findings. Patterns in each article were identified. The authors abstracted variables that were relevant to the review question. Consequently, the authors recorded the author, year of publication, country, aim, study setting, design, sample size, and main findings of each article. Finally, the findings were synthesized according to the study characteristics and the aim of the review.
Quality Assessment
The methodological quality of the articles was evaluated using the JBI quality assessment checklist for cross-sectional studies (Appendix B).
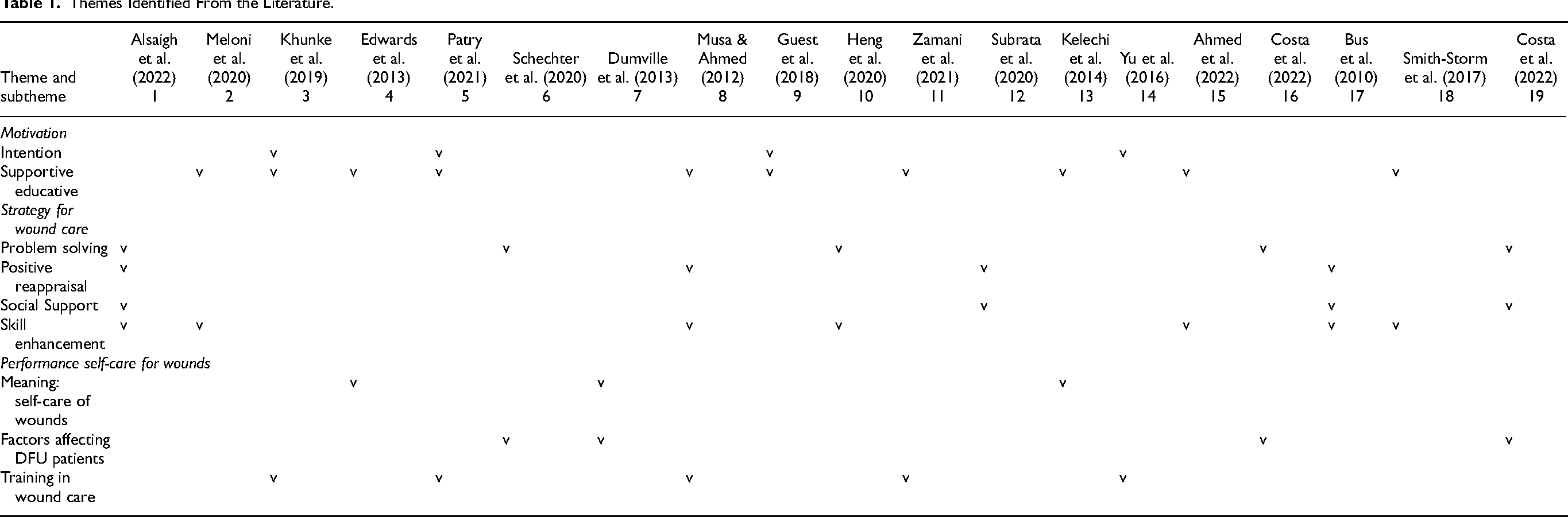
The number of respondents in each study's sample ranged from 10 minimum to 323 maximum, depending on the study. The majority of respondents and participants were DFU patients. Table 1 lists the major themes and subthemes of the study articles. The outcomes of integrating the findings from the research investigations into each study are detailed in the following sections.
Themes Identified From the Literature.
Results
Characteristics of the Studies
The literature search generated 2,595 articles, and 1,103 articles were assessed for relevance by title and abstract after duplicate articles were eliminated. In total, 1,429 articles were eliminated after titles were examined. After analyzing the abstracts, another 1,324 articles were discarded, leaving 168 articles that could be evaluated in full. Because 149 complete articles did not match the inclusion and exclusion requirements, they were excluded. Following a quality assessment by three reviewers using evidence, 19 complete articles were included in the evaluation for analysis and thematic integration of the research findings (Figure 1). These studies were conducted in the United States of America (n = 2), Saudi Arabia (n = 1), Canada (n = 5), Australia (n = 1), the United Kingdom (n = 2), Singapore (n = 1), Indonesia (n = 1), Sudan (n = 2), Rome (n = 1), Norway (n = 1), Texas (n = 1), and the Netherlands (n = 1). The number of respondents in each study's sample ranged from 10 to 323. The total sample size from these studies was 1,885 patients with DFU, and the majority (n = 15) of the studies were conducted in at least two or more healthcare settings. Regarding study design, six were retrospective studies, four were cross-sectional studies, five were RCTs, two were qualitative studies, and one was a prospective study, while only one was mixed. Furthermore, a correlation analysis was performed in all articles to show how diabetic foot ulcer patients can perform self-treat wound care (Table 2).
Summary of the Articles.

Quality Appraisal of the Review
As a result, using JBI quality assessment tools, 19 studies were of high methodological quality because all these articles received a “yes” rating for all relevant elements (Appendix B). No article was excluded based on this data evaluation rating system.
How Diabetic Foot Ulcer Patients Can Self-Treat Wound Care
The themes identified from the literature are motivation to perform self-treatment of wound care, self-wound care strategy, and DFU patients’ self-treatment of wound care (Table 1).
Motivation to Perform Self-Treatment for Wound Care
DFU patient motivation means having the intention to care for themselves. In two of the study articles, it was stated that to avoid prolonged recovery durations, hospital stays, amputations, and decreased quality of life after DFU treatment, patients were consistently motivated to practice self-care (Guest et al., 2018; Patry et al., 2020). In addition, some patients are motivated to engage in self-care because of their beliefs about DFU and the importance of self-wound care (Yu et al., 2016). However, more investigation is required to pinpoint the elements that boost DFU patients’ enthusiasm for self-care and create practical plans to encourage their adoption of self-wound care management techniques (Kuhnke et al., 2019). Several articles (Guest et al., 2018; Patry et al., 2020; Yu et al., 2016) discuss factors related to motivation and its impact on wound self-care. Related studies highlight three key elements: the desire to recover, personal involvement in wound care, and enhanced quality of life. Findings were categorized as connected to motivating intention or supporting education due to data integration. Meanwhile, the supportive education provided by the wound nurse during discharge had an impact on the independence of DFU wound care, which resulted in maximum wound healing (Ahmed et al., 2022; Guest et al., 2018; Kuhnke et al., 2019; Meloni et al., 2020; Musa & Ahmed, 2012; Patry et al., 2020; Smith-Strøm et al., 2016; Zamani et al., 2021).
Self-Wound Care Strategy
Research shows that effective strategies for wound self-care include problem solving, positive reappraisal, social support, and skill improvement (Costa et al., 2022). Patients used problem solving to identify and overcome barriers to self-wound care, such as limited health literacy and social support (Alsaigh et al., 2022; Costa et al., 2022; Costa et al., 2017; Heng et al., 2020; Schechter, 2020). Positive reappraisal helps patients reframe negative thoughts and emotions related to their condition and improve a positive outlook (Alsaigh et al., 2022; Bus et al., 2010; Musa & Ahmed, 2012; Subrata et al., 2020).
Social support from healthcare providers, family, and friends provided emotional and practical support to patients managing their wounds and promoted self-wound care training, which is vital for their problem solving to achieve good wound healing (Alsaigh et al., 2022; Heng et al., 2020; Innocent et al., 2019; Meloni et al., 2020; Musa & Ahmed, 2012; Smith-Strøm et al., 2016).
Skills enhancement from wound care experts, like a nurse, assisted patients in acquiring the information and abilities necessary to effectively manage their wounds, including wound care, glucose management, and infection avoidance (Alsaigh et al., 2022; Meloni et al., 2020; Musa & Ahmed, 2012). Therefore a comprehensive approach to wound care includes strategies addressing the underlying factors influencing patients’ ability to engage in self-wound care and support their self-management practices (Heng et al., 2020; Innocent et al., 2019; Smith-Strøm et al., 2016).
DFU Patients’ Self-Treatment of Wound Care
Self-treatment of wound care performance involves several factors, including independent wound care, factors that influence DFU patients, and training in wound care. To avoid protracted healing durations, hospital stays, amputations, and a decreased quality of life, patients must comprehend the value of self-care and be encouraged to do it regularly during the months of DFU treatment. Some patients do it conventionally, and others use modern wound care methods that have been taught by wound experts. Even though they are not as good as expert wound nurses, DFU patients are considered quite successful with sustainable wound healing results (Dumville & Deshpande, 2013; |Edwards & Stapley, 2010; Kelechi et al., 2014).
Factors affecting patients with DFU's ability to engage in self-care include limited health literacy, social support, and motivation, which can be addressed through education, social support, and motivational strategies (Costa et al., 2020; Guest et al., 2018). Only a few studies have included patients gaining the knowledge and skills necessary to effectively manage their wounds, including wound care, off-loading, glycemic management, and infection prevention (Costa et al., 2020, 2022; Dumville & Deshpande, 2013; Schechter, 2020; Yu et al., 2016).
Therefore, a comprehensive approach to wound care must include strategies that address the underlying factors influencing patients’ ability to engage in self-care, provide education and training in wound care, and support their involvement in self-management practices (Kuhnke et al., 2019; Meloni et al., 2020; |Musa & Ahmed, 2012; Patry et al., 2020; Yu et al., 2016; Zamani et al., 2021).
Discussion
This is the first review that comprehensively combines research studies and examines how DFU patients deal with and motivate themselves to take care of their wounds. This review's key finding is the absence of any single study that combines independent wound care management, supportive educational, and persuasive wound care viewpoints. This finding, which is important, establishes the need for further study to close this skill and knowledge gap.
However, there are some studies that focus on each area separately. This review, which offers fresh perspectives on the subject, summarized and extracted the findings.
The findings from this review reveal that DFU patients’ motivation can be intentional, supportive, and educative. This is consistent with the study that DFU patients with intention motivation are probably more involved and dedicated to their wound care and consistent with research related to supportive education (Fife et al., 2016; Wang et al., 2010). Innovative educational pilots supporting literacy for independent wound care have been found to be effective in increasing knowledge and skills among uninsured patients who do not have access to healthcare resources (Young & Bullen, 2016).
However, there is limited proof that health literacy affects DFU patients; therefore, literacy-sensitive training initiatives are required to address wound knowledge and abilities. Practice-based learning can also effectively enhance wound care education, but skilled professionals are needed to facilitate the process and support learners. Therefore, supportive educative interventions that address the underlying factors influencing a patient's ability to engage in self-care and provide education and training on wound care can be effective in improving independent wound care (Costa et al., 2022).
Practical strategies for independent wound care include collaboration, self-care, optimal self-care, wound cleaning, wound inspection, application and removal of wound dressings, and recognition of the warning signs of infection. Education focusing on wound care for patients is critical for optimizing patient outcomes and healing rates (Moore & Coggins, 2021). The Association of Diabetes Care & Education Specialists (ADCES) and the ADA can provide wound care professionals with access to educational materials and resources, including wound care educational opportunities featuring the latest standards of practice presented by top leaders in the field. Consequently, a thorough strategy for wound care must incorporate tactics that discuss the underlying reasons affecting patients’ capacity for self-care, offer education and training on wound care, and support their participation in self-management techniques (ADCES, 2021).
Effective wound care involves several factors, including optimal self-care, recognizing the warning signs of infection, cleaning, inspection, applying and removing wound dressings, and good nutrition. The movement toward self-care is primarily driven by rising healthcare costs, increasing numbers of people living with injuries, and the understanding that patients can take an active role in their care. Health education interventions can also be effective in improving wound care independently of patients, especially in patients at home (Zhu et al., 2023).
The review's findings highlight what is understood about DFU patients’ motives and coping mechanisms for dealing with daily challenges and responsibilities. They also found factors influencing their ability to provide independent wound care. These results indicate the need for additional education and dissemination and implications for future studies. It is crucial that patients with DFU are given the opportunity to think about how learning about their intentions and motives might improve their future wound care and recovery as well as strategies for preventing recurrent wounds. Community service initiatives can include discussions on these topics. Additionally, DFU patients in wound care and self-care management roles might think about how these findings can affect local wound care policy and government funding to promote sustainable health.
No research has connected DFU patients’ motivation, self-care, and self-perform of wound care. This is a crucial research gap that will aid patients’ ongoing self-treatment of wounds. Only the findings of this integrative review covered the inclusion and exclusion criteria. Data integration should be handled independently because none of the articles that assessed or described the three topics (motivation, self-care, and wound care) were found together. Another drawback is that not all regions have been adequately covered by the scientific evidence that is now available.
Implications for Practice
In this literature study, several practice areas were found that wound care and medical professionals might address to provide self-directed wound care environments and guidelines that can sustain and boost DFU patients’ motivation and intention to continue caring for their wounds. Overall, from reading this literature review, patients with DFU will clearly understand the importance of motivation and wound care strategies to defend themselves and care for their wounds in their daily needs.
The identified intentional and supportive educative factors related to motivation, intention, will, and involvement are essential because they can advance wound care and healing continuity. Additionally, DFU patients manage stress and stressful situations by using independent wound care techniques because they better understand their physical condition, have the time to care for their own wounds, and see the progress of wound healing, thus eliminating anxiety due to diabetic foot wounds. Patients with DFU may require counseling or training to enable them to employ adaptive rather than maladaptive techniques. They can assist themselves in efficiently caring for their wounds using adaptive methods, including problem solving, positive reframing, and seeking help. To assist DFU patients in setting and achieving holistic wound healing and health objectives, a better grasp of self-care is required.
Conclusion
The growing understanding of wound care and its relationship to wound healing necessitates the concurrent accumulation of data on the factors influencing DFU patients’ intentions for autonomous wound care and how they handle its requirements and environment. In this integrative literature review, we combine and emphasize key facts about DFU patients’ motivation and wound care techniques that will help them continue to treat their wounds independently.
Intentional and supportive educative motivation is found in patients with DFU, and this motivation is crucial for altering behavior, intention to remain, and involvement. DFU patients employ adaptive and maladaptive wound care techniques to maintain their will, abilities, and motivation. The perspectives of patients with DFU on effective wound care and its associated elements are crucial for sustaining their beliefs, even though reasons for and techniques for providing wound care are critical.
Considering the available research, key aspects of motivation, wound care techniques, and DFU patients’ attitudes toward independent wound care are discussed. The evidence has a significant gap that highlights the need for further study, especially in the sustainability of self-sustained wound care. The evidence results produced by this integrative review must be retrieved and used by patients with DFU.
Footnotes
Acknowledgment
The authors thank for the mentoring publication program from the Research Centre of Research Excellent in Advancing Community Health (REACH), Surabaya, Indonesia.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Appendix A. Literature searching strategies and results (February 2023).

| Database | Query | Search result |
|---|---|---|
| Google Scholar | "Self-wound care” AND “diabetic foot ulcer” AND “motivation*” Filters applied: 2010–2023, |
1,000 |
| Web of Science | (ALL = (Self-wound care) AND ALL = (diabetic foot ulcer) AND ALL = (motivation)) AND (PY == (“2023” OR “2022” OR “2021” OR “2020” OR “2019” OR “2018” OR “2017” OR “2016” OR “2015” OR “2014” OR “2013” OR “2012” OR “2011” OR “2010”) AND DT == (“ARTICLE”) AND LA == (“ENGLISH”)) | 996 |
| PubMed | ((“independent"[All Fields] OR “self-care"[All Fields]) AND (“wound care"[MeSH Terms] OR “self-wound care"[All Fields] AND (“diabetic foot ulcer"[MeSH Terms] OR (“DFU"[All Fields] AND “self-wound care"[All Fields]) OR “DFU"[All Fields]) AND “patient"[All Fields]) AND ((fft[Filter]) AND (english[Filter]) AND (2010:2023[pdat])) | 399 |
| Scopus | (self-wound care) AND (diabetic foot ulcer) AND (patient) Filters applied English, 2010–2023 |
200 |
| Total | 2,595 | |
| Final full text relevant to our review | 19 |
Appendix B. JBI critical appraisal checklist for analytical studies.

| Articles | Parameter | Score out of 8 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Clear inclusion criteria | Clear study setting and subject | Valid and reliable exposure measurement | Standard objective | Identification of confounding factors | Strategies to deal with confounding factors | Valid and reliable outcomes measurement | Appropriate statistical analysis | ||
| Ahmed et al. (2022) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Alsaigh et al. (2022) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Bus et al. (2010) | √ | √ | √ | √ | N/A | N/A | √ | √ | 6 |
| Costa et al. (2020) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Costa et al. (2022) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Dumville and Deshpande (2013) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Edwards et al. (2013) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Guest et al. (2018) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Heng et al. (2020) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Kelechi et al. (2014) | √ | √ | √ | √ | N/A | N/A | √ | √ | 6 |
| Kuhnke et al. (2019) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Meloni et al. (2020) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Musa & Ahmed (2012) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Patry et al. (2021) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Schechter et al. (2020) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Smith-Storm et al. (2017) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Subrata et al. (2020) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Yu et al. (2016) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |
| Zamani et al. (2021) | √ | √ | √ | √ | √ | √ | √ | √ | 8 |