
Abstract
Introduction
Globally, chronic kidney disease (CKD) has emerged as one of the leading causes of mortality and it is one of a small number of noncommunicable diseases that have shown an increase in associated deaths over the past two decades. Chronic kidney disease affects approximately 50% of patients with type 2 diabetic mellitus (DM).
Objective
To determine CKD preventive attitude, practices, and associated factors among type 2 DM (T2DM) patients attending follow-up in a diabetic clinic at Asella Referral and Teaching Hospital.
Methods
Institutional based cross-sectional study was conducted at Asella Referral and Teaching Hospital among T2DM patients from December 23, 2021, to January 23, 2022. Data were entered into EpiData 4.2.00 and analyzed by Statistical Package for the Social Sciences version 23.0.
Result
A total of 216 study participants were included in to this study. The level of good preventive attitude and practice toward CKD among T2DM patients were 61.6% (n = 133, 95% CI: 55.6–68.0) and 54.6% (n = 118, 95% CI: 47.7–60.6), respectively. Age (50–59 years) (adjusted odds ratio [AOR] = 0.351, 95% CI: 0.125–0.988, p = .047), married (AOR = 4.423, 95% CI: 1.366–14.314, p = .013), urban residents (AOR = 0.321, 95% CI: 0.152–0.680, p = .003), and governmental employed (AOR = 0.269, 95% CI: 0.076–0.954, p = .042) were significantly associated with CKD preventive attitude. Formal education (AOR = 1.686, 95% CI: 1.416–5.502, p = .043), an average monthly income of ≥8000 ETB (AOR = 4.048, 95% CI: 1.129–14.520, p = .032), family history of CKD (AOR = 1.417, 95% CI: 1.231–7.136, p = .045) were significantly associated with CKD preventive practice.
Conclusion
The level of good preventive attitude and practice toward CKD among T2DM patients was 61.6% and 54.6%, respectively. Age, marital status, residence, and occupation were significantly associated with good preventive attitude of T2DM patients. Whereas educational status, average monthly income, and duration since diagnosed with T2DM were significantly associated with good CKD preventive practice. Health educational program needs to occur to improve the preventive attitude and practice toward CKD among T2DM patients.
Introduction
Chronic kidney disease (CKD) is a type of kidney disease in which there is kidney disability and gradual loss of kidney function over a period of months to years (Wikipedia, 2023). Chronic kidney disease can be caused by diabetes, hypertension, glomerulonephritis, pyelonephritis, and interstitial nephritis (Kidney Education, 2023). The modifiable risk factors for CKD are uncontrolled high blood pressure, type 1 diabetic mellitus (DM) with onset before age 20, cigarette smoking, and obesity, while the nonmodifiable risk factors are genetics, race, age >65 years and low birth weight (Veeraish, 2021).
At an early stage, CKD does not show any symptoms, but at later stages it starts to show symptoms such as shortness of breath, edema, increased urination especially at night, blood in urine, itching, insomnia, headache, tiredness, muscle crumps, loss of appetite, and erectile dysfunction (Kidney Resource center, 2023; NHS, 2023). Chronic kidney disease can be classified into five stages based on the estimated GFR; Stage 1 is when e-Gfr is ≥90 ml/min, and this indicates as the kidneys are healthy, but some signs can be seen like protein in the urine. Stage 2 is when GFR is 60–89 ml/min, and this indicates mild kidney damage. Stage 3 is when GFR is 30–59 ml/min, which indicates some kidney damage. Stage 4 is when GFR is 15–29 ml/min and this shows as there is moderate to severe kidney damage. Stage 5 is when GFR is less than 15 ml/min. At this stage, the kidney is very close to failure or has completely failed (Stages of Kidney Disease, 2020).
Review of Literature
Type 2 DM (T2DM) is the leading cause of end-stage renal disease (ESRD) in developed countries (Stages of Kidney Disease, 2023). In 2017, the prevalence of CKD was estimated as 9.1% globally (Bikbov et al., 2020). There is a high prevalence of CKD in patients with T2DM (Calvo-Hueros et al., 2021). Chronic kidney disease globally affects about 50% patients living with T2DM (Rajput et al., 2017; Thomas et al., 2016). The prevalence of CKD among T2DM patients was 43.5% in USA (Rahim et al., 2017), 27.5% in UK (Rahim et al., 2017), 47.1% in Australia (Rahim et al., 2017), 24.3% in Spain (Calvo-Hueros et al., 2021), 23% in Palestine (Naser et al., 2021), 32.07% in Saudi Arabia (Naser et al., 2021), 60.78% in Oman (Naser et al., 2021), 33.6% in Yemen (Naser et al., 2021), 35.4% in Thailand (Jitraknatee et al., 2020), and (13.9–63.5%) in Bangladeshi (Mondal et al., 2021d). In Africa, the prevalence of CKD among T2DM patients ranges from 2% to 41%. Whereas it was 94.9% in South Africa (Geletu et al., 2018), 28.5% in Ghana among T2DM and hypertension (Tannor et al., 2019), and 18.2% in Ethiopia among DM patients (Shiferaw et al., 2020).
Type 2 DM is the leading cause of CKD in the United States, with around 40% of patients with T2DM showing evidence of CKD (Ephraim et al., 2018). Type 2 DM became the second-leading cause of CKD and CKD-related death and the third leading cause of CKD-related disability-adjusted life-years in 2019 (Deng et al., 2021). Chronic kidney disease is associated with premature morbidity and mortality and the risk of progressing to ESRD and mortality rates rise with the advancing severity of CKD (CDC, 2022).
A study done in 2017 showed that T2DM patients having CKD were associated with 2.5 million incident cases, 129.56 million patients, and 405.99 thousand deaths. Chronic kidney disease resulted in 1.2 million deaths globally (Bikbov et al., 2020). The burden of CKD is greater among minor ethnic groups due to increased prevalence of comorbidities and reduced access to health care and due to limited services for the diagnosis, management, and monitoring of CKD at the primary health care level especially in low-income countries like Africa there is a high burden of CKD (Luyckx et al., 2021).
A study done in Palestine showed that prevention and early detection of CKD practice were significantly associated among normal body mass index, urban residents, high educational level, less tobacco use, last HbA1c below 7, and higher knowledge, attitude, and Michigan Diabetic Knowledge Test score (Badran et al., 2023). Besides, a study done in Bangladesh showed that CKD attitude was significantly associated with sex, occupation, and income in T2DM (Mondal et al., 2021a).
Thus, the importance of early CKD detection is to prevent CKD progression and associated complications, thus improving patient outcomes and reducing the impact of CKD on health care resources (Levin & Stevens, 2011). Knowing the magnitude of CKD among T2DM patients is important to prevent cardiovascular complications, kidney failure, ESRD, and to advice if diabetic patients develop CKD not to take certain medicines, such as nonsteroidal anti-inflammatory drugs and to modify their diet to prevent kidney disease from progressing (NIH, 2020).
The previous studies done in different settings indicate that the prevalence of CKD among T2DM is increasing at an alarming rate in both developed and developing countries. It causes a great number of mortalities and morbidities worldwide and it may have an economic impact on patients and to nations. However, even if it causes this entire problem, there is limitation of the study that addressed CKD preventive attitude, practice, and associated factors among T2DM attending follow-up clinic in the study area while also globally. Therefore, this study was aimed to assess the CKD preventive attitude, practice, and associated factors among T2DM patients attending follow-up clinic in Asella Referral and Teaching Hospital, Oromia Regional State, Ethiopia.
Methods
Study Area
The study was done at DM clinic in Asella Referral and Teaching Hospital. This Hospital serves as teaching and at the same time it gives health services for the patients. It is a governmental hospital located in Asella, Arsi zone, Oromia regional state, Ethiopia. Asella is located in the Arsi Zone of the Oromia Region, about 175 km from Addis Ababa, the capital city of Ethiopia (Wikipedia, 2024).
Study Period
The study was conducted from December 23, 2021, to January 23, 2022.
Study Design
Institutional-based cross-sectional study was conducted as per the “Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines and methodologies” (von Elm et al., 2007).
Research Questions
▪ What is the level of CKD preventive attitude among T2DM patients attending follow-up clinic in Asella Referral and Teaching Hospital, Oromia Regional State, Ethiopia?
▪ What is the level of CKD preventive practice among T2DM patients attending follow-up clinic in Asella Referral and Teaching Hospital, Oromia Regional State, Ethiopia?
▪ What are the factors associated with CKD preventive attitude among T2DM patients attending follow-up clinic in Asella Referral and Teaching Hospital, Oromia Regional State, Ethiopia?
▪ What are the factors associated with CKD preventive practice among T2DM patients attending follow-up clinic in Asella Referral and Teaching Hospital, Oromia Regional State, Ethiopia?
Population
Source Population
All T2DM patients attended DM follow up clinic at Asella Referral and Teaching Hospital.
Study Population
All randomly selected T2DM patients attended DM follow up clinic at Asella Referral and Teaching Hospital.
Eligibility Criteria
Inclusion Criteria
All T2DM patients age ≥ 18 years old.
Exclusion Criteria
Type 2 DM patients who have already developed CKD were excluded from this study.
Sample Size Determination
A single population proportion formula was used to determine the sample size. During this, we assumed the prevalence of CKD preventive attitude and practice (p = 50%), because there was no study that was done in Ethiopia. Therefore, the sample size was determined by using the following assumptions;
▪ N = total T2DM patients with monthly follow-up = 400 ▪ P = Proportion 50%, ▪ d = margin of error 5% ▪ Z @/2 = 1.96 corresponding to 95% CI. ▪ no = initial sample size ▪ nf = final sample size ▪ 10% for nonresponses
Since the total T2DM patients with monthly follow-up were 400, which is less than 10,000, the sample size was adjusted by using correction formula:

Sampling Techniques and Procedures
The logbook of all T2DM patients who were attending the diabetic follow-up clinic at Asella Referral and Teaching Hospital was checked carefully. Two of T2DM patients who have already developed CKD were excluded from this study. Whereas those T2DM patients who have attended the diabetic follow-up clinic during data collection and fulfilled the inclusion criteria and volunteer to participate were included in to this study.
Then, all T2DM patients who were attending the diabetic follow-up clinic were numbered in sequence from 1 to 398. Next, a simple random sampling technique; Table of random numbers was used to select the study participants until it reach the detrmined sample size (216).
Study Variable
Dependent Variable
Chronic kidney disease preventive attitude
Chronic kidney disease preventive practice
Independent Variable
Sociodemographic variables: Gender, age, educational level, average monthly income, and marital status.
Clinical-related variables: Duration since diagnosed with T2DM, family history of CKD, number of drugs currently taking, presence of comorbidities, and glycemic control.
Operational Definition
Good preventive attitude: If participants scored greater than or equal to the mean score of preventive CKD attitude-related questions (Mondal et al., 2021c).
Poor preventive attitude: If participants scored less than the mean score of preventive CKD attitude-related questions (Mondal et al., 2021c). This outcome variable was measured by computing the raised attitude-related questions and categorized by using a mean value.
Good preventive practice: If participants scored greater than or equal to the mean score of preventive CKD practice-related questions (Mondal et al., 2021c).
Poor preventive practice: If participants scored less than the mean score of preventive CKD practice-related questions (Mondal et al., 2021c). This outcome variable was measured by computing the raised practice-related questions and categorized by using a mean value.
Good glycemic control: When HbA1c level <7 (Hussain et al., 2019).
Poor glycemic control: When HbA1c ≥ 7 (Hussain et al., 2019).
Data Collection Tool, Procedures, and Quality Control
Data were collected by using face-to-face interviewer questionnaires and medical chart review. Questionnaires were adapted from the relevant literatures (Mondal et al., 2021c) (Hussain et al., 2019) (Mondal et al., 2021b). The English version of the questionnaire was translated in to Afan Oromo by language experts for better understanding. It was reviewed and approved by senior experts in the field.
The first part of the questionnaire includes sociodemographic characteristics of the study participants, the second part includes clinical related variables, the third part includes questions related to CKD preventive knowledge, the fourth part includes questions related to CKD preventive attitude and the fifth part includes questions related to the CKD preventive practice.
Data quality was ensured by providing training to data collectors on interview process techniques and ways to collect data. Data were collected by Bachelor of Science (BSc) nurses and supervised by Master of Science (MSc). A pretest of the questionnaire was done on 11 T2DM patients, which were out of the study setting and a reliability of the questionnaire was checked. The Cronbach's alpha value was 0.842 and 0.807 for attitude and practice, respectively.
Statistical Analysis
Data entry was done by Epi data version 4.2.0.0, exported and analyzed by using Statistical Package for the Social Sciences version 23.0. The questionnaires were coded as “0” and “1” while “1” represented the correct answers and “0” represented incorrect answers. The outcome variable was dichotomized and coded as “0” and “1” represented (good attitude = 1 and poor attitude = 0) and practice (good practice = 1 and poor practice = 0). Descriptive statistics such as percent, frequency, and mean were conducted, and the result was presented by using tables, figures, and text. Moreover, bivariable and multivariable logistic regression model were used to check the association between the independent variables and dependent variables. For screening of the variables to move to the multivariable logistic regression analysis, we used p-value of <.25 for the variables in bivariable logistic regression analysis. Hosmer–Lemeshow's goodness-of-fit test was used to check for model fitness and got p-value = 0.714 for CKD preventive attitude, and p-value = .801 for CKD preventive practice. Crude odds ratio and adjusted odds ratio (AOR) with the corresponding 95% CI was calculated and with p values <.05 was considered as statistically significant.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Ethical Review and Research Committee of the Nursing Department, College of Health Sciences, Arsi University, Ref. No./AU/H/S/C/CN/272/21. Then, permission was obtained from Asella Referral and Teaching Hospital. The objectives of this study were discussed with all study participants recruited for this study. Besides, the study participants were assured about the confidentiality of the information attained. Lastly, written informed consent was received from the study participants. All methods were performed in accordance with the ethical standards as laid down in the Declaration of Helsinki and its later amendments or comparable ethical standards.
Results
Sociodemographic Characteristics of T2DM Patients
Two hundred sixteen T2DM patients were participated in our study and given a response rate of 100%. More than half 114 (52.8%) of T2DM patients were male. About 90 (41.7%) of them were aged ≥60 years. The majority 160 (74.1%) of them have attended formal education. More than half 191 (88.4%) of them were married. Whereas 158 (73.1%) lived in urban, 92 (42.6%) were working in private business, 87 (40.3%) were orthodox followers, and more than half 150 (69.4%) of them were Oromo by ethnic background (Table 1).
Sociodemographic Characteristics of T2DM Patients Who Were Attending a Diabetic Follow-up Clinic at Asella Referral and Teaching Hospital, 2022 (n = 216).
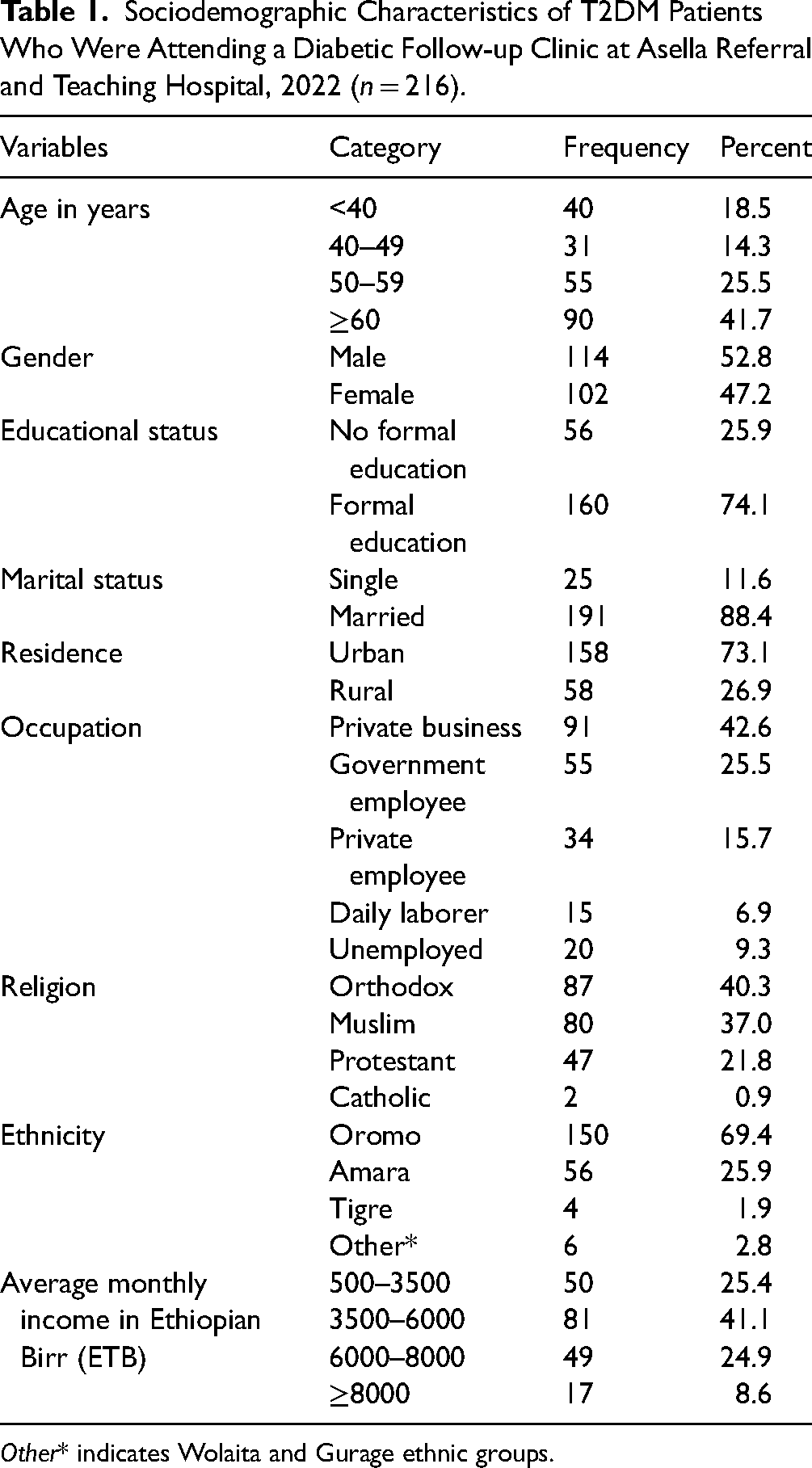
Other* indicates Wolaita and Gurage ethnic groups.
Clinical-Related Characteristics of T2DM Patients
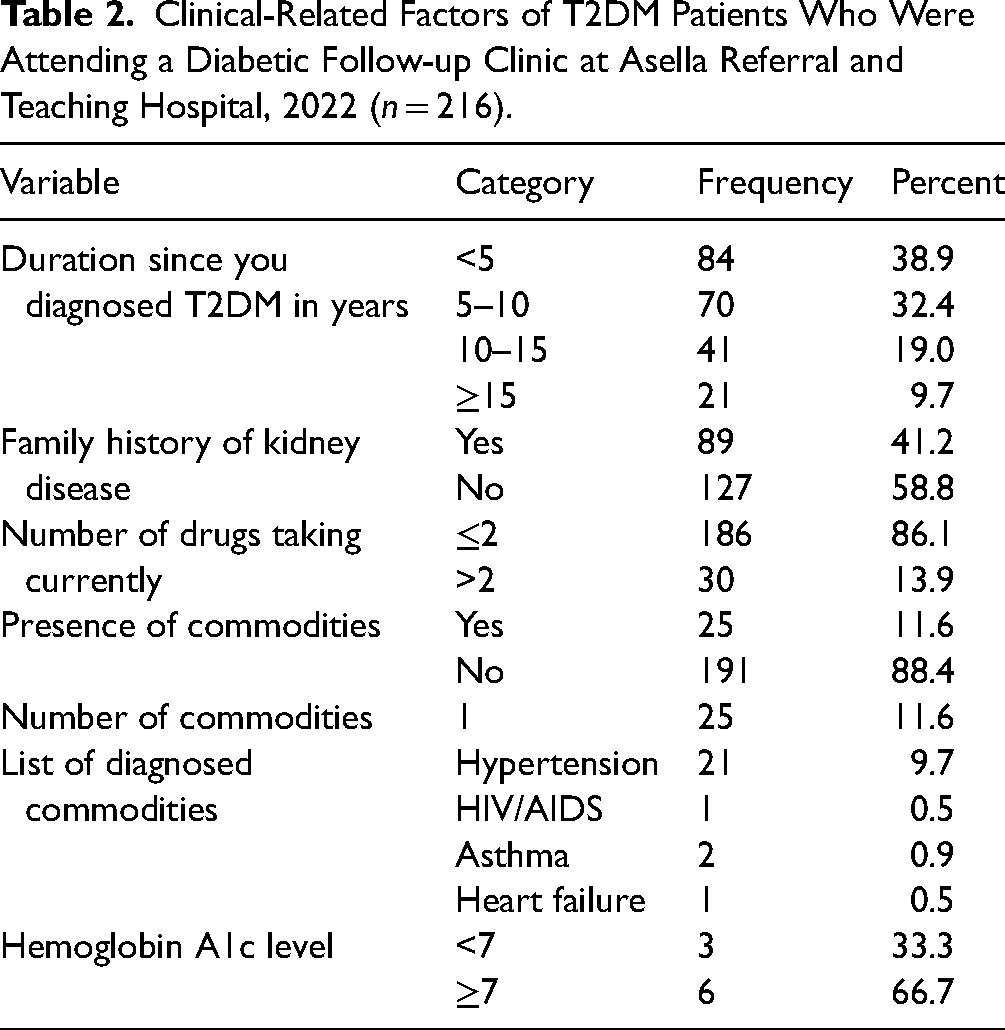
Among 216 T2DM patients, the majority 84 (38.9%) of them had a duration of less than 5 years since diagnosed with T2DM. Around 89 (41.2%) of them had a family history of kidney disease, 186 (86.1%) of them have taken ≤2 drugs currently, around 25 (11.6%) of them had comorbidities. Regarding the Hemoglobin A1c level, 6 (66.7%) of them had ≥7 levels (Table 2).
Clinical-Related Factors of T2DM Patients Who Were Attending a Diabetic Follow-up Clinic at Asella Referral and Teaching Hospital, 2022 (n = 216).
Preventive Attitude of CKD among T2DM Patients
The level of good preventive attitude of CKD among T2DM patients who were attending a diabetic follow-up clinic was 61.6% (n = 133, 95% CI: 55.6–68.0) (Figure 1).
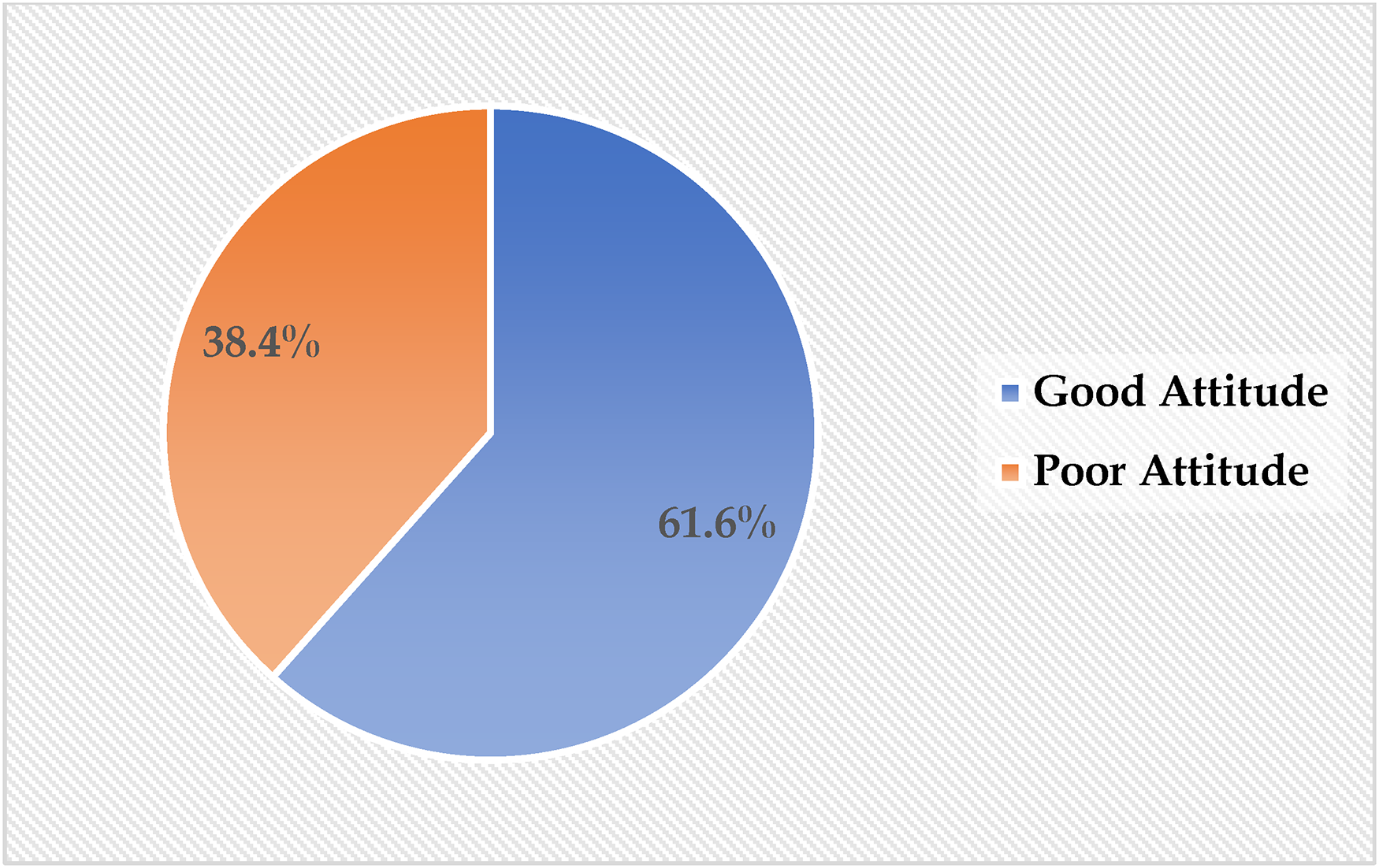
Level of CKD preventive attitudes among T2DM patients who were attending a diabetic follow-up clinic at Asella Referral and Teaching Hospital, 2022 (n = 216).
Preventive Practice of CKD among T2DM Patients
The level of good preventive practice of CKD among T2DM patients who were attending a diabetic follow-up clinic at Asella referral and teaching hospital was 54.6% (n = 118, 95% CI: 47.7–60.6) (Figure 2).
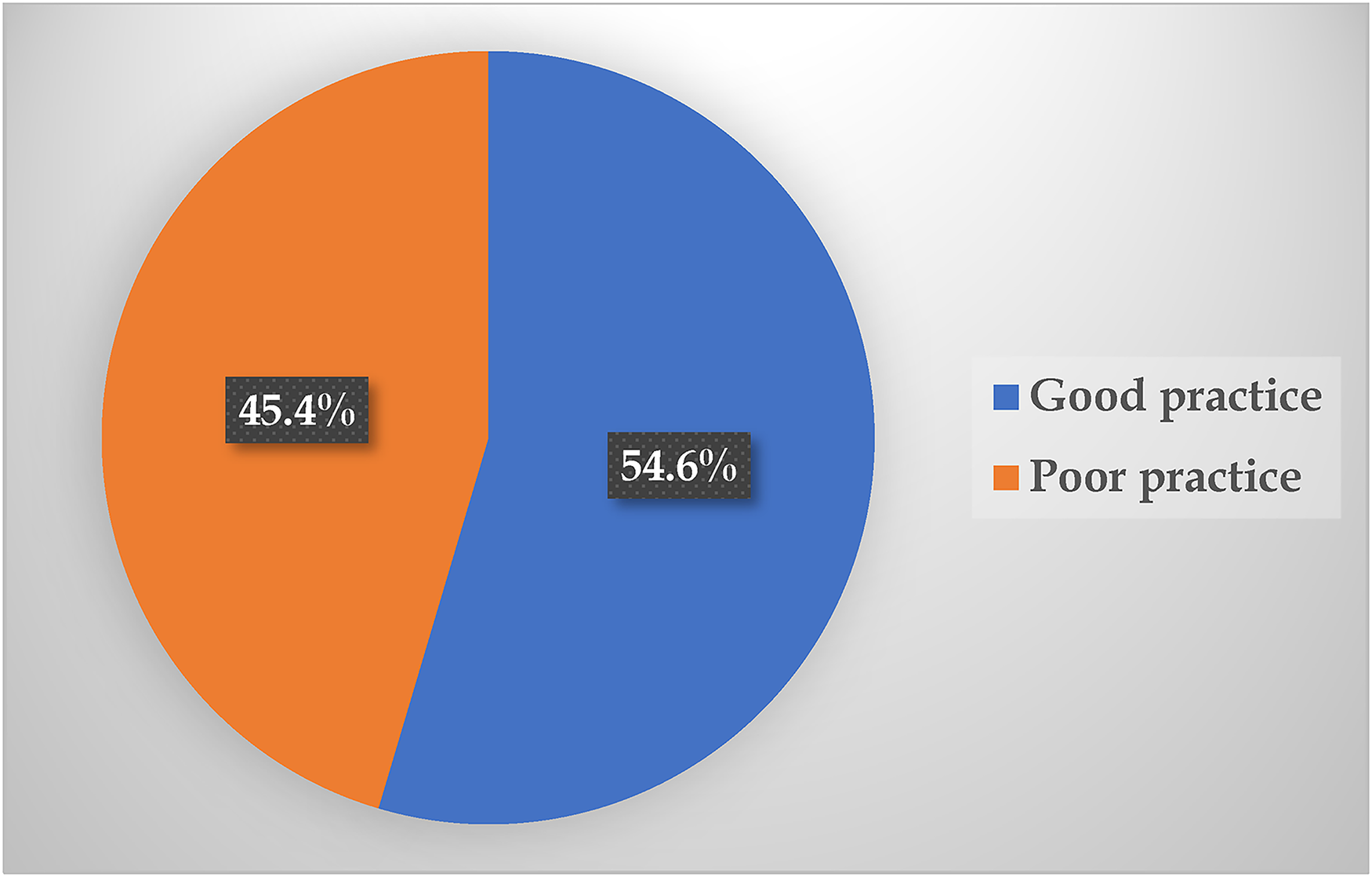
Level of CKD preventive practice among T2DM patients who were attending a diabetic follow-up clinic at Asella Referral and Teaching Hospital, 2022 (n = 216).
Factors Associated with Preventive Attitude of CKD among T2DM
To check the association of independent variables with good preventive attitude: age, gender, educational status, marital status, residence, occupation, average monthly income, duration since diagnosed with T2DM, family history of kidney disease, number of drugs currently taking, and presence of comorbidities were checked in a bivariable logistic regression analysis. In bivariable logistic regression analysis, age, marital status, residence, occupation, duration since diagnosed T2DM, and presence of comorbidities were shown a p-value of <.25. But, only age, marital status, residence, and occupation were significantly associated with CKD preventive attitude among T2DM patients in multivariable logistic regression analysis.
The odds of having a good CKD preventive attitude among T2DM patients aged (50–59 years) was 35.1% times (AOR = 0.351, 95% CI: 0.125–0.988, p = .047) more likely when compared with T2DM patients aged ≥60 years old. The likelihood of having a good CKD preventive attitude among T2DM patients who were married was 4.423 times (AOR = 4.423, 95% CI: 1.366–14.314, p = .013) more likely than single T2DM patients. The odds of having a good CKD preventive attitude among T2DM patients’ urban residents was 32.1% times (AOR = 0.321, 95% CI: 0.152–0.680, p = .003) more likely than rural residents. The likelihood of having a good CKD preventive attitude among T2DM patients who were governmental employed was 26.9% times (AOR = 0.269, 95% CI: 0.076–0.954, p = .042) more likely when compared with T2DM patients who were unemployed (Table 3).
Bivariable and Multivariable Logistic Regression Analyses of Factors Associated with Preventive Attitude of CKD among T2DM Patients Who Were Attending a Diabetic Follow-up Clinic at Asella Referral and Teaching Hospital, 2022 (n = 216).
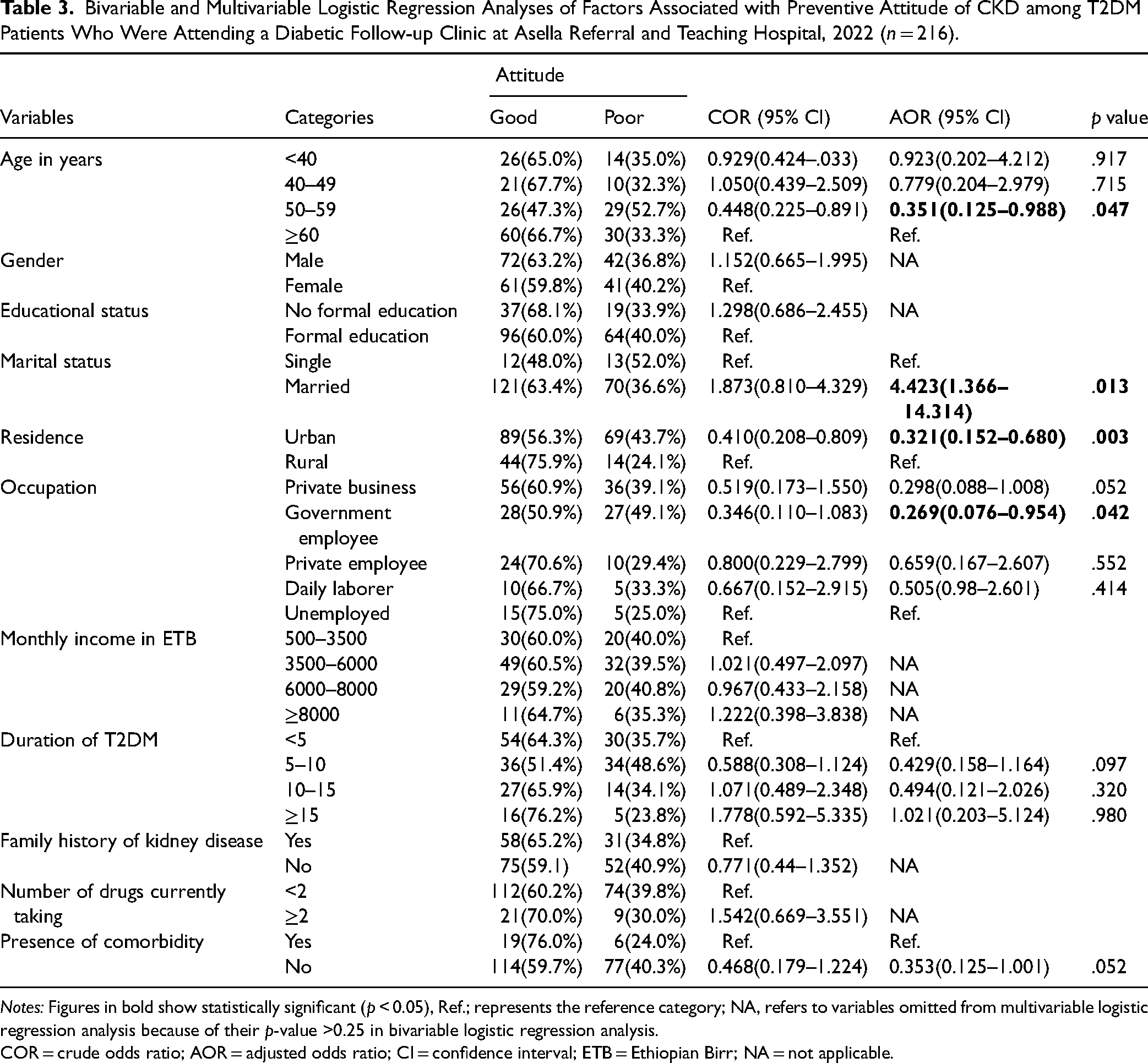
Notes: Figures in bold show statistically significant (p < 0.05), Ref.; represents the reference category; NA, refers to variables omitted from multivariable logistic regression analysis because of their p-value >0.25 in bivariable logistic regression analysis.
COR = crude odds ratio; AOR = adjusted odds ratio; CI = confidence interval; ETB = Ethiopian Birr; NA = not applicable.
Factors Associated with Preventive Practice of CKD Among T2DM
Similarly, bivariable and multivariable logistic regression analyses were done to check the association of the independent variables with good CKD preventive practice. Primary age, gender, educational status, marital status, residence, occupation, average monthly income, duration since diagnosed with T2DM, family history of kidney disease, number of drugs currently taking, and presence of comorbidities were checked in bivariable logistic regression analysis for their association with good CKD preventive practice. Then, age, gender, educational status, occupation, average monthly income, duration since diagnosed with T2DM, and family history of CKD were shown a p-value of <.25 in bivariable logistic regression analysis. However, only educational status, average monthly income, and duration since diagnosed T2DM were significantly associated with good CKD preventive practice in multivariable logistic regression analysis.
The odds of having good CKD preventive practice among T2DM patients who were attending formal education was 1.686 times (AOR = 1.686, 95% CI: 1.416–5.502, p = .043) more likely when compared with their contrary. The likelihood of having good CKD preventive practice among T2DM patients who had an average monthly income of ≥8000 ETB was 4.048 times (AOR = 4.048, 95% CI: 1.129–14.520, p = .032) more likely when compared with T2DM patients who had an average monthly income of 500–3500 ETB. The odds of having good CKD preventive practice among T2DM patients who had a family history of CKD was 1.417 times (AOR = 1.417, 95% CI: 1.231–7.136, p = .045) more likely when compared with their contrary (Table 4).
Bivariable and Multivariable Logistic Regression Analyses of Factors Associated with Preventive Practice of CKD among T2DM Patients Who Were Attending a Diabetic Follow-up Clinic at Asella Referral and Teaching Hospital, 2022 (n = 216).
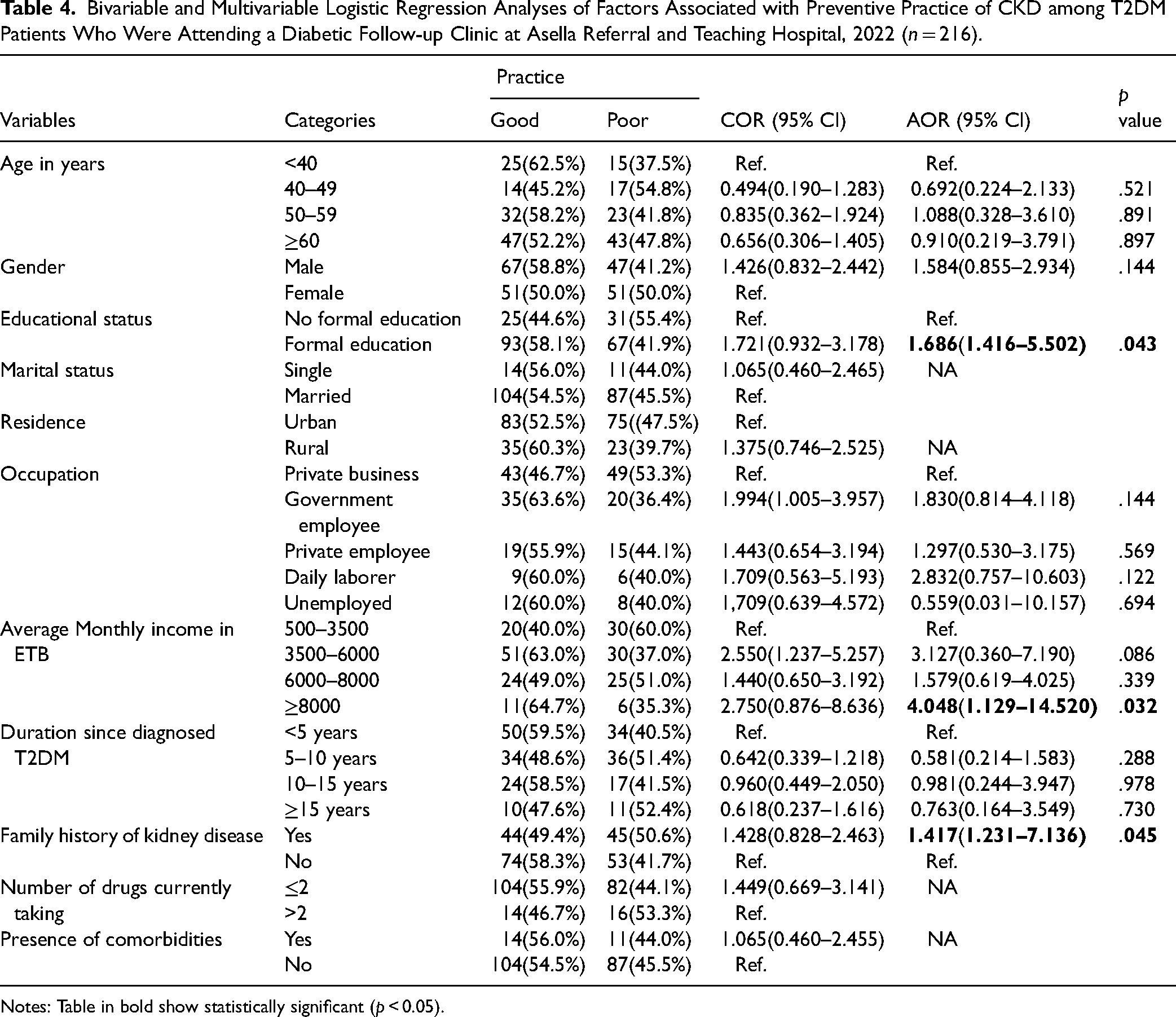
Notes: Table in bold show statistically significant (p < 0.05).
Discussion
In this study, the level of good CKD preventive attitude among T2DM patients who were attending a diabetic clinic at Asella Referral and Teaching Hospital was 61.6% (n = 133, 95% CI: 55.6–68.0). This study finding was higher than the study conducted in Bangladesh, 28.6% (Mondal et al., 2021b). This might be due to the study period differences; the study was conducted in 2019. There is also a study population difference. In the study conducted in Bangladesh, it included only T2DM patients who had a follow-up for ≥1 year and excluded T2DM patients aged >70 years.
This study finding was lower than the study conducted in Fiji Islands, 68.9% (Zibran & Mohammadnezhad, 2019). This might be because of study population differences; the study conducted in Fiji has included T2DM patients diagnosed with CKD. But in this study, we have excluded T2DM patients who had already confirmed for CKD. There is also a sociodemographic difference; they have included only participants aged ≥30 years.
The odds of having a good preventive attitude among T2DM patients aged (50–59 years) was 35.15 times (AOR = 0.351, 95% CI: 0.125–0.988, p = .047) more likely when compared with T2DM patients aged ≥60 years old. This study finding was supported by a study done in Fiji Island (Zibran & Mohammadnezhad, 2019). The likelihood of having a good preventive attitude among T2DM patients who were married was 4.423 times (AOR = 4.423, 95% CI: 1.366–14.314, p = .013) more likely than single T2DM patients. This finding was supported by a study done in Fiji Island (Zibran & Mohammadnezhad, 2019).
Furthermore, the odds of having a good preventive attitude among T2DM patients’ urban residents was 32.1% times (AOR = 0.321, 95% CI: 0.152–0.680, p = .003) more likely than rural residents. The likelihood of having a good preventive attitude among T2DM patients who were governmental employed was 26.9% times (AOR = 0.269, 95% CI: 0.076–0.954, p = .042) more likely when compared with T2DM patients who were unemployed. This study was supported by a study conducted in Bangladesh (Mondal et al., 2021a).
The level of CKD good preventive practice among T2DM patients who were attending a diabetic clinic at Asella Referral and Teaching Hospital was 54.6% (n = 118, 95% CI: 47.7–60.6). This study finding was lower when compared with a study done in Bangladesh, 82.1% (Mondal et al., 2021b). This might be due to sociodemographic and study population differences. This study finding was also lower than the study conducted in Fiji Islands, 88.3% (Zibran & Mohammadnezhad, 2019). This could be due to that study population differences, and they have included patients confirmed for CKD. There is also sociodemographic difference.
The odds of having good preventive practice among T2DM patients who were attending formal education was 1.686 times (AOR = 1.686, 95% CI: 1.416–5.502, p = .043) more likely when compared with their contrary. This study was supported by a study done in Palestine (Badran et al., 2023). The likelihood of having good preventive practice among T2DM patients who had an average monthly income of ≥8000 ETB was 4.048 times (AOR = 4.048, 95% CI: 1.129–14.520, p = .032) more likely when compared with T2DM patients who had an average monthly income of 500–3500 ETB. The odds of having good preventive practice among T2DM patients who had a family history of CKD was 1.417 times (AOR = 1.417, 95% CI: 1.231–7.136, p = .045) more likely when compared with their contrary.
Strengths and Limitations
Since there was no study done at the study setting, this could give essential insights for the concerned bodies. The study design used for this study was a cross-sectional study. This study design does not help to determine the cause and effect. Furthermore, there were limitations of the literatures on this essential topic globally. This study would lessen the challenges for future researchers who will be concerned to do a study on this topic. Moreover, since this study was done at a single hospital, the findings of this study may not be generalizable to the national level.
Implications for Practice
This study gives important evidence to support T2DM patients to minimize the occurrence of CKD among them. These findings would also deliver vital information for healthcare providers, policy makers and implementers, government, and researchers to provide a special attention for T2DM patients in order to prevent the development of CKD. Health education programs need to occur to improve the preventive attitude and practice toward CKD among T2DM patients.
Conclusion
The level of good preventive attitude and practice toward CKD among T2DM patients who were attending a diabetic clinic at Asella Referral and Teaching Hospital was 61.6% (n = 133, 95% CI: 55.6–68.0) and 54.6% (n = 118, 95% CI: 47.7–60.6), respectively. The multivariable logistic regression analysis indicated that age, marital status, residence, and occupation were significantly associated with good preventive attitude of T2DM patients. Whereas educational status, average monthly income, and duration since diagnosed with T2DM were significantly associated with good CKD preventive practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.