
Abstract
Introduction
Coronary artery disease is the leading cause of death, and one of the major health burdens worldwide. The prevalence of coronary artery disease in Ethiopia is increasing steadily irrespective of age and gender. Some of the risk factors are preventable and modifiable.
Objective
The aim was to examine the levels of knowledge, attitude, and practice of cardiac patients toward preventive measures of coronary artery disease.
Methods
An institution based cross sectional study was conducted in Tikur Anbessa Specialized Hospital between March and April 2022. A total of 402 patients were randomly selected. Interviewer guided standardized questioners were used to gather information from participants. Descriptive statistics was utilized to describe participant's characteristics and logistics regression analysis was employed to examine the relationship between independent and outcome variables. Level of significance was determined at p < .05 and 95% CI.
Result
A total of 320 participants with response rate of 83.3% were included. The mean age was 46.74 ± 14.15SD. Most (67.2%) of the respondents demonstrated good knowledge with mean knowledge score of 58 ± 15.96 SD. More than half of the respondents (54.4%) had good attitude, with mean attitude score of 60.4 ± 25.33SD. Half (50%) of respondents mean showed good practice with mean practice score of 55.13 ± 17.365. Upon logistic regression, variables namely, sex (AOR = 0.578, 95%CI: 0.332–0.879), and presence of comorbidity (AOR = 2.818, 95%CI: 1.029–7.713), were significantly associated with knowledge. Similarly, occupation (AOR = 0.66, 95%CI: 0.330–0.968), marital status (AOR = 0.545, 95%CI: 0.333–0.893), and sex (AOR = 0.506, 95%CI: 0.313–0.819), were significantly associated with practice of coronary artery disease prevention.
Conclusion
The study found that 67.2% of cardiac patients had good knowledge, 54.3% had a positive attitude, but only 50% practiced effective coronary artery disease prevention. Male gender, single marital status, unemployment, and presence of comorbidities were significantly associated with lower knowledge and poor preventive practices.
Introduction
Background
Cardiovascular disease (CVD) is a noncommunicable condition and remains the leading cause of death worldwide. It is the single largest cause of mortality in developed countries and is also a major contributor to the disease burden in developing nations (Health, 2022). Among the different types of CVD, coronary artery disease (CAD) is particularly concerning, affecting approximately 126 million individuals globally about 1.72% of the world's population (Khan et al., 2020). The burden of CAD is increasing and is projected to exceed 1,845 cases per 100,000 people by 2030.
Coronary artery disease is a major health challenge in both high-income and low-income countries, an estimated 3.8 million men and 3.4 million women die each year from CAD. Countries in Africa and the middle east bear a particularly heavy burden, largely due to the high prevalence of risk factors such as smoking, hypertension, dyslipidemia, diabetes, and sedentary lifestyles (Almahmeed et al., 2012). The situation is worsening in developing nations, where increasing trends of CAD-related mortality have been reported (Institute, 2010).
The Ethiopian Medical Association Annual conference on September 29, 2021, reported that, according to the WHO's 2018 report, coronary heart disease death in Ethiopia reached 47,712, accounting for 7.81 of all total deaths that year (Tesfye, 2021).
Assessment of the population's knowledge, attitude, and practice (KAP) toward CAP preventive measures has been effective in guiding the development of primary and secondary prevention programs in various countries (Organization, 2008; Saadia et al., 2010). Studies from Bangladesh, Namibia, Saudi Arabia, Nepal, Kirkuk city, and Malaysia indicate generally low awareness and inadequate preventive behaviors related to CAD, particularly among individuals with lower educational or socioeconomic status (Alwakeel et al., 2018; De Klerk, 2018; Al-Naimi, 2020). Research also shows that cardiac patients typically possess moderate knowledge about CAD risk factors such as hypertension, smoking, unhealthy diets, and physical inactivity but have limited understanding of secondary prevention strategies, including cardiac rehabilitation and long-term medication adherence (Liu et al., 2024). For instance, a study in China found that while many patients were aware of the need to manage blood pressure and cholesterol, few could recognize early symptoms or adopt essential lifestyle changes (Liu et al., 2023). Similarly, in Jordan, a structured education program significantly improved patient knowledge one-month post intervention (Al-Smadi et al., 2013).
Attitude toward CAD prevention is generally positive. Most patients recognize the importance of lifestyle changes and adherence to medications (Ahmad et al., 2022). However, attitude alone often fails to produce behavioral change. In Canadian cardiac rehabilitation programs, education improved beliefs, but motivation was found to be more decisive factor in adopting preventive behaviors (Sweet et al., 2021). Other influential factors include cultural beliefs, health literacy, and fear of recurrence (Zhao et al., 2024).
Despite reasonable knowledge and positive attitude, actual preventive practices are often inadequate. A study among Iranian CAD patients revealed that only one-third engaged in regular physical activity, and fewer than 35% followed a heart-healthy diet (Mirzaei-Alavijeh et al., 2024). Similarly, in Shanghai, patients showed moderate adherence to therapies and life style changes, with rural residents lagging significantly behind urban populations (Wang et al., 2024).
Prevention remains the most effective approach to combat the rising epidemic of CAD, particularly in developing countries (Al-khlaiwi et al., 2023). Enhancing public knowledge, shaping favorable attitudes, and improving preventive practices are crucial steps. Yet, despite the increasing prevalence of CAD and the importance of public awareness, there is a lack of comprehensive studies assessing KAP toward CAD prevention in the Ethiopian population. Therefore, this study was aimed to assess the levels of KAP, and associated factors of CAD prevention among CAD patients in the area.
Literature Review
The literature reviewed highlights the complex pathophysiology and public health burden of CAD, emphasizing its classification into acute and chronic syndromes resulting from coronary atherosclerosis and microvascular dysfunction (Gaze, 2012). Several modifiable and nonmodifiable risk factors such as hypertension, smoking, diabetes, obesity, age, and family history significantly contribute to CAD progression. Numerous studies conducted globally ranging from Bangladesh, Namibia, Saudi Arabia, Nepal, Kirkuk City, and Malesia demonstrate varying levels of KAP toward CAD prevention, generally indicating limited awareness and inadequate preventive behaviors, particularly among populations with lower educational or socioeconomic status (Alwakeel et al., 2018; De Klerk, 2018; Al-Naimi, 2020). While some respondents across these studies were aware of key risk factors and symptoms, such as chest pain and smoking, many failed to recognize atypical signs or fully comprehend preventive strategies such as physical activity and dietary modifications (De Klerk, 2018). Attitudinal responses were generally more positive than actual practice, with a significant gap between knowledge and behavior, revealing a critical need for targeted education and intervention programs (Al-Naimi, 2020). More recent studies support these findings. A national survey in Saudi Arabia found that the general population had moderate awareness of CAD and its risk factors, particularly around lifestyle-related prevention, but limited recognition of early symptoms (Alaamri & Naser, 2025). Similarly, a multicenter study in 2024 involving patients after coronary stenting reported moderate KAP scores, with higher engagement among urban residents and those with prior cardiac events, while insurance gaps and comorbidities were associated with lower practice levels (Zhou et al., 2025). Furthermore, factors such as gender, education level, access to healthcare resources were found to significantly influence CAD-related knowledge and preventive practice across populations (Al-Naimi, 2020).
Methods and Materials
Study Area, Period, and Design
An institutional based cross-sectional study was conducted in Tikur Anbessa Specialized Hospital in Addis Ababa, the capital city of Ethiopia from March 2022 to April 2022. The hospital is one of the tertiary referral hospitals among the five hospitals, and the largest and the last referral hospitals in the country. Moreover, the hospital is an educational center for medical, nursing, pharmacy, laboratory, and other health professionals organized under the umbrella of AAU. The hospital provides specialty service including cardiology referral services from all regions of the country (AAU, n.d.). An estimated total of 2000 patients are seen in the cardiac referral clinic each month. Therefore, the hospital was selected purposively, since it receives all types of cardiac patients from all regions, and presence of adequate flow of patients.
Population
All patients who were attending care and treatment in the cardiology unit in Tikur Anbessa Specialized Hospital were included.
Sample Size Determination
The sample size was determined using a single population proportion formula with an assumption of 50% prevalence, 95% confidence level and 0.05 marginal error, since there was no similar study found in the area:
Sampling Technique
The list of patients was obtained from the cardiac referral clinic registry and coded, using a simple random sampling method, study participants were selected and subsequently approached for interviewer-administered questionnaires, which were completed with the support of trained data collectors.
Eligibility Criteria
All adult patients diagnosed with CAD who were attending follow-up at the cardiac referral clinic during the study period were included; however, critically ill and mentally incompetent patients were excluded.
Data Collection Instrument
A structured interviewer guided instrument adopted from similar studies in the literature was used to gather the information from participants (Muhamad et al., 2012). The instrument was tested for its validity and reliability scoring Cronbach's alpha of KAP of 0.73, 0.71, and 0.60 respectively. Moreover, it has been used among nurses to evaluate KAP preventive strategies regarding CAD (Ammouri et al., 2016). The instrument was initially prepared in English. To ease participants understanding, it was translated to the local language “Amharic” by language experts in both languages. The questionnaire was also pretested among 5% of the total sample in Zewditu Memorial Hospital to check for its consistency and clarity.
The questionnaire constitutes a total of 45 questions with: (1) Sociodemographic variables containing 10 questions assessing general information about patients, (2) Knowledge questions containing 10 items to assess the level of understanding of CAD, its risk factors, and sign and symptoms with yes or no responses, each question may have correct answer that refers to one point for positive response and zero for negative response. (3) Attitude questions also contain 12 items to assess level of sociobehavioral perspectives and preconceived notions about CAD. These were measured using Likert scale scoring based on (Strongly Agree = 5, Agree = 4, Uncertain = 3, Disagree = 2, strongly Disagree = 1). Mean attitude score was calculated and used as a reference for classifying level. Those who scored mean and above mean were consider having good attitude and those below the mean were considered to have poor attitude. (4) Practice questions contain 13 items to assess health seeking behaviors and preventive behaviors. Each question contains 1 point for positive life style practice and 0 point for negative life style practice and the score was classified in to levels, good practice for those who score mean and above and poor practice for those who scored less than the mean.
Data Collection Procedure
Nurses holding BSc degree with rich experience of data collection were recruited and trained prior to the actual data collection period. Selected study units were approached, and informed about the purpose of the study. Verbal consent was obtained from participants willing to take part in the study were included into the study, and data collection process was guided by the data collectors.
Data Quality Assurance
To assure quality, a standardized valid data collection instrument was used, the instrument was translated to the local language by language experts. The instrument was also pretested in 5% of the total sample in a hospital other than the study setting. Data collectors were trained for one day. The data collection was closely supervised on daily base.
Analysis
The data were cleaned, coded, and entered in to a Statistical Package for Social Science software version 26 for analysis. Descriptive statistics including frequencies, percentages, mean, and standard deviations were used to describe participant's characteristics, and logistic regression analysis which include bivariate and multivariate analysis were used to examine association between independent and outcome variables. Mean score was used to describe knowledge and practice since mean score preserves scale sensitivity, capturing slight differences in individual responses that might be lost when data is dichotomized into good versus poor (Burns & Grove, 2010). Variables with p < .2 in bivariate analysis were included into the multivariate model and those variables with p < .05 at 95% CI on the multivariate analysis were considered significant.
Results
Sociodemographic Characteristics of the Study Subjects
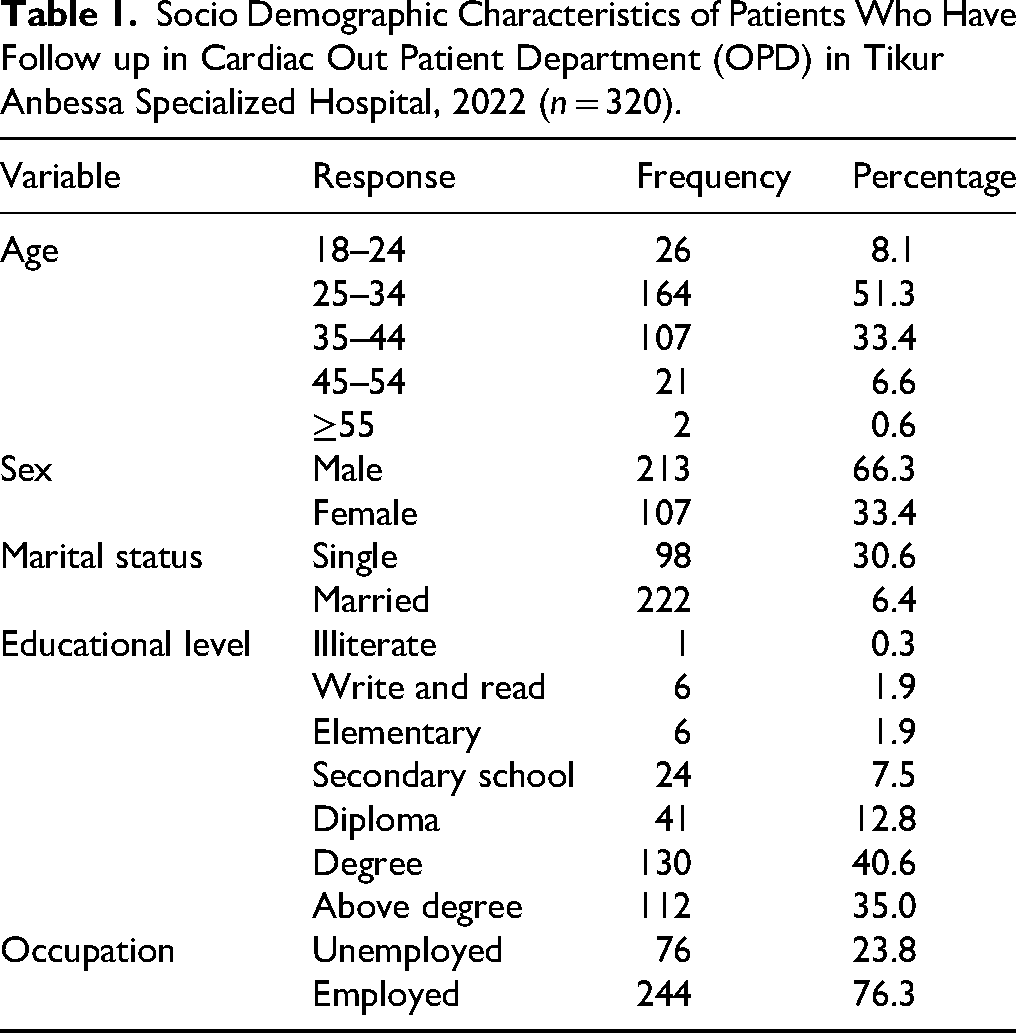
A total of 320 patients were included, making the response rate of 83.3%. Concerning their clinical characteristics, 46.9% were diagnosed as hypertension, 28.1% CAD, and the remaining 25% with other cardiac and other comorbid illnesses. The mean age with standard deviation of the respondents was 46.74 ± 14.150. Among them 164 (51.3%) were between the age of 25–34 years. Majority of the participants were males (66.3%) and majority of them attended formal education (99.7%). More than 66% (n = 222) of the respondents are married and more than three-forth (76.3%) were employed (Table 1).
Socio Demographic Characteristics of Patients Who Have Follow up in Cardiac Out Patient Department (OPD) in Tikur Anbessa Specialized Hospital, 2022 (n = 320).
Knowledge of Patients About CAD Prevention
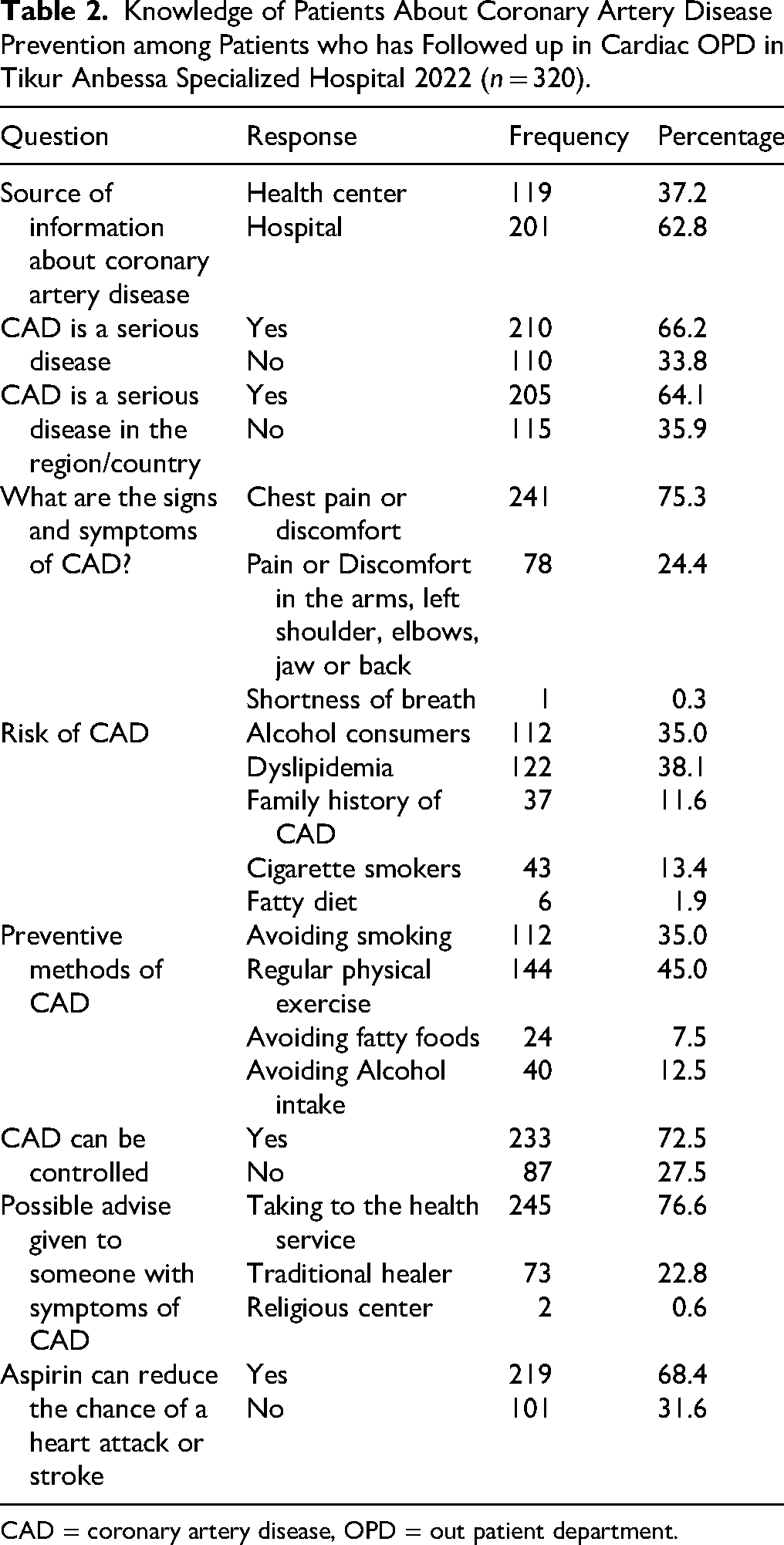
Knowledge score was measured using a standardized instrument adopted from previous studies in the literature containing 10 knowledge questions assessing the level of understanding risk factors, and sign and symptoms of CAD (Muhamad et al., 2012). Accordingly, the overall knowledge of participants who demonstrated good knowledge of CAD prevention was 67.2%, with mean knowledge score of 58 ± 15.96. Moreover, most (62.8%) of the respondents reported that they received information about CAD prevention from hospitals, and three quarters (75.3%), of the respondents listed chest pain or discomfort as signs and symptoms of CAD, 38.1% identified dyslipidemia as the main risk factor for CAD, 144 (45%) stated regular exercise, and 112 (35%) picked cessation of smoking, 219 (68.4) reported aspirin reduces the chance of heart attack or stroke (Table 2).
Knowledge of Patients About Coronary Artery Disease Prevention among Patients who has Followed up in Cardiac OPD in Tikur Anbessa Specialized Hospital 2022 (n = 320).
CAD = coronary artery disease, OPD = out patient department.
Attitude of Patients Toward CAD Prevention
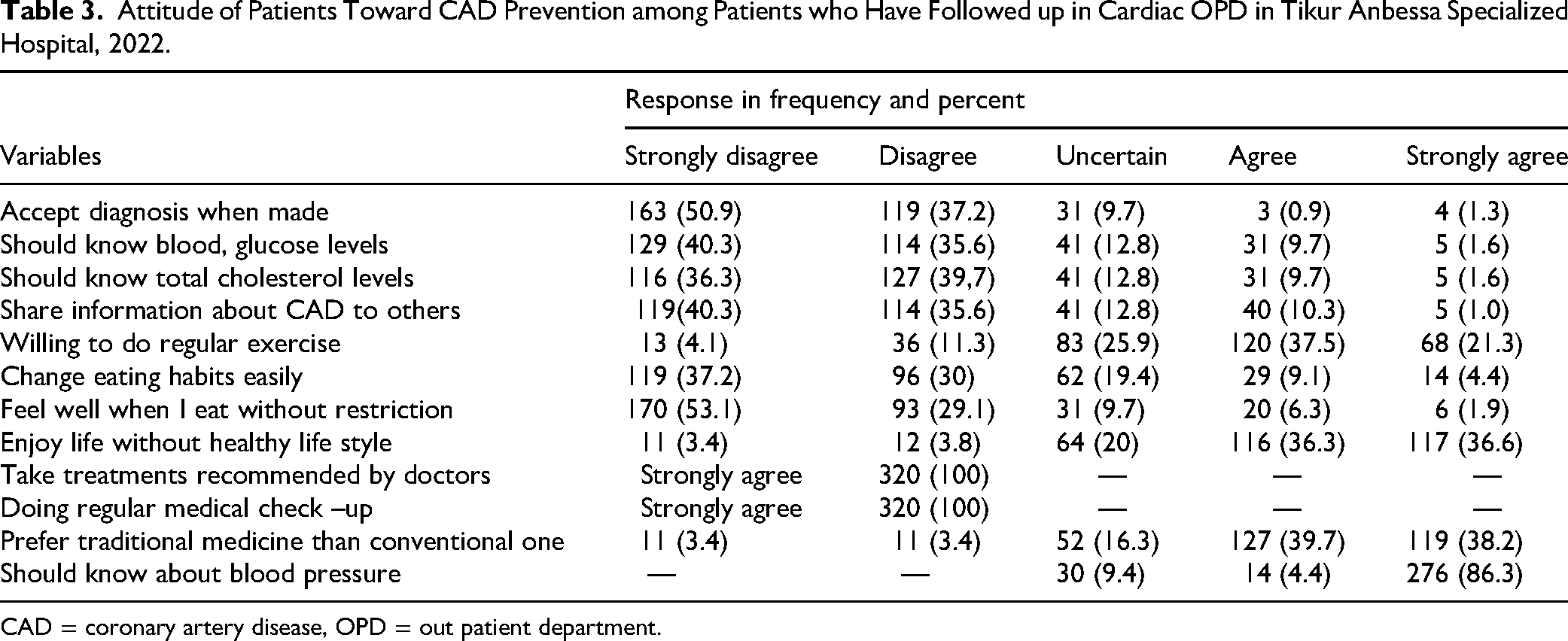
The attitude score was measured using a standardized instrument adopted from previous studies in the literature containing 12 Likert scale-based attitude questions assessing the level of sociobehavioral perspectives and preconceived notions about CAD (Muhamad et al., 2012). Thus, the overall attitude score of participants was (54.3%) demonstrated good attitude toward CAD prevention with the mean attitude score of 6.04 ± 2.533. More than half (50.9%) of respondents reported they disagree to accept diagnosis when told by their doctor, all respondents strongly agreed to taking treatments recommended by their doctors, 37.5% agreed they are willing to do regular exercise, 40.3% disagree the need to know their blood glucose level, 39.7% disagrees to know their cholesterol levels, and 38.2% strongly agreed they prefer traditional medicine than conventional one (Table 3).
Attitude of Patients Toward CAD Prevention among Patients who Have Followed up in Cardiac OPD in Tikur Anbessa Specialized Hospital, 2022.
CAD = coronary artery disease, OPD = out patient department.
Practice of Patients Toward Prevention of CAD among Patients who Attained Cardiac OPD in Tikur Anbessa Hospital, 2022
Practice score was measured using a standardized instrument adopted from previous studies in the literature containing thirteen items assessing health seeking and preventive behaviors (Ammouri et al., 2016). The overall good practice was 50% with mean practice score of the study participants were 55.13 ± 17. 365. Majority of the respondents (70%) reported that, they seek medical attention in a health facility when they experience symptoms of CAD, and when asked the time length between symptom and seeking medical care, three quarters 246 (76.9%) said immediately. Concerning physical exercise, more than half (51.9%) reported they do vigorous exercise for 20 or more minutes three times a week, about 57.5% reported they reduce salt from their diet, 61.9% said they prefer low fat and cholesterol containing diets, 70% reported they strictly follow doctor's prescription (Table 4).
Practice of Patients Toward CAD Prevention among Patients who Have Followed up in Cardiac OPD in Tikur Anbessa Specialized Hospital, 2022.

CAD = coronary artery disease, OPD = out patient department.
Factors Associated with KAP of Participants Toward CAD Prevention
Bivariate and multivariate analyses were employed to examine whether a statistical association exists between independent and the outcome variables and find patterns and correlations between the variables. All variables were included into the bivariate regression model, and variables having p-value <.2 were included into the multivariate, then those variables with p-value <.05 in the multivariate regression model were considered significant. Moreover, while 54.3% showed a good attitude toward CAD prevention (mean score 6.04 ± 2.533), many held misconceptions, over half rejected diagnosis, 38.2% preferred traditional medicine, and fewer supported regular physical exercise or monitoring glucose and cholesterol levels.
Accordingly, variable namely, sex and presence of comorbidity showed significant correlation with knowledge, whereas occupation, marital status, and sex of the respondents were significantly associated with practice toward CAD prevention.
Being male gender showed significant negative correlation with knowledge of CAD prevention. Those male patients were 0.58 time less likely to have good knowledge compared to female patients (AOR = 0.578; 95% CI 0.340–0.981). Comorbid illness was another predictor found to be correlated with knowledge of CAD prevention. The odds of good knowledge toward CAD in those patients who doesn’t have other comorbidities were 2.8 times higher compared to those who had comorbid illness (AOR = 2.818, 95%CI = 1.029–7.713).
Moreover, occupation is another predictor found to be linked with patients “practice toward CAD prevention.” Those unemployed patients were negatively associated with good practice toward CAD Prevention. Unemployed patients were 1.8 times less likely to have good practice compared to employed patients (AOR = 0.66, 0.333–0.893). Similarly, marital status of patients revealed association with practice toward CAD prevention. Single patients were negatively associated with CAD prevention among the patients. Those patients with single marital status were 0.55 times less likely to have good practice compared to married patients (AOR = 0.545, 95%CI = 0.330–0.968), and male gender was also negatively associated CAD prevention (AOR = 0.506, 95%CI = 0.313–0.819) to have good practice as compared to females (Table 5).
Factors Associated with Knowledge, Attitude, and Practice of Coronary Artery Disease Prevention among Patients Attained Cardiac OPD in Tikur Anbessa Specialized Hospital, 2022.

CAD = coronary artery disease, OPD = out patient department.
Discussion
The study aimed at determining the level of KAP toward CAD prevention. The findings revealed good knowledge of 67.2 with mean knowledge score of 58 ± 15.84 SD. The result is higher than the studies done in Oman where only 39.5% had good knowledge and the mean score of participants was 13.52 ± 4.59 (Ammouri et al., 2016), Kuantan 48.3% had good knowledge (Jamaludin et al., 2019), and the study in Malaysia showed 38.2% (Dayal & Singh, 2018). The discrepancy may be due to differences in sociodemographic characteristics, sampling, and sample size. However, the finding is in agreement with the study done in Malaysia, where 55.6% of the participants were reported to have good knowledge score (Yahya et al., 2012).
In the current study, about three quarters (75.3%) of the respondents did not recognize the important symptoms of CVDs such as pain or discomfort in the jaw, neck or back, feeling weak, light-headedness, or faint, sudden numbness or weakness of the face, arm, or leg, sudden confusion or trouble speaking or understanding others. This finding is higher than a study in Lucknow city where proportion of respondents who did not recognize the important symptoms were 50% (Dayal & Singh, 2018). Another study in Sweden also reported that majority (79%) of the respondents knew that chest pain, shortness of breath, and nausea and vomiting are possible symptoms of a myocardial infarction (Henriksson et al., 2012). The difference among the studies may be due to socioeconomic, and participant's educational background variations, and low attention to create awareness between the facilities.
In this study, slightly less than three quarters of the respondents (72.4%) reported that they are willing to make lifestyle changes. This finding is slightly lower than the study in Namibia where, 84% of the respondents indicated that they do want to make some life style changes (De Klerk, 2018).
The present study showed a significant association between gender and knowledge where males were 0.58 times less likely to have good knowledge (AOR = 0.58, 95%CI: 0.340–0.981) as compared to females .This result was consistent with a study by Jensen et al. which indicated that women were more aware of CHD risk factors than their male counterparts (De Klerk, 2018). But the finding is in contrast with a study done in Saudi Arabia where there was insignificant difference between males and females in CAD risk factors knowledge (Jensen & Moser, 2008). The same finding was reported in the Jordanian survey (Mukattash et al., 2012), whereas a study in Oman, no significance was reported between gender and knowledge (Ammouri et al., 2016). The possible explanation may be Women are generally more proactive in seeking health information and medical care leading to greater exposure preventive knowledge (Courtenay, 2000). The study also showed significant association between having other comorbidities and knowledge of CAD prevention, where by the odds of good knowledge toward CAD prevention in patients who doesn’t have other comorbid illness was 2.8 times higher compared to those who had morbidities (AOR = 2.818, 95%CI = 1.029–7.713). We couldn’t find other studies that support or disprove these findings. Unlike the study in Oman, the current study didn’t find correlation between education, and marital status with knowledge of CAD prevention (Ammouri et al., 2016), similarly marital status was associated with knowledge in a study done in Egypt where married participants were negatively correlated with low levels of knowledge about CAD compared to their single counterparts (Ammouri et al., 2016; Seef et al., 2013). Another study in Australia also showed specific marital-related factors, such as family obligations, have been found to result in a lack of time to engage in preventative actions and may therefore contribute to a lack of knowledge about CAD preventive measures (Haidinger et al., 2012).
In this study, participant's occupational status was linked with practice toward CAD prevention. Unemployed patients were 0.55 times less likely to have good practice employed patients (AOR = 0.545, 0.333–0.893). Similarly marital status of the respondents was associated with practice where single patients were 0.566 times less likely to have good attitude as compared to married patients (AOR = 0.566, 95%CI = 0.330–0.968). These findings couldn’t be supported or rejected by similar studies.
The study also showed no association between routine medical checkup, practice and overall KAP score with attitude of the patients. This finding is inconsistent with a study in Bangladesh where patients who had routine medical checkups had better levels of attitude (p < .001) and practice (p < .001).
Study Strengths and Limitations
This study provides important insights into the KAP toward CAD prevention among cardiac patients in Ethiopia an area where data have been limited. The inclusion of relatively large sample size and the use of a validated, reliable, and contextually adapted data collection tools are major strengths that enhance the credibility and applicability of the findings.
However, the study has some limitations. Being a cross-sectional design, it cannot establish cause–effect relationship between variables. Self-reported data may be prone to social desirability and recall bias. Additionally, the study was conducted in a single tertiary institution, which may limit generalizability to broader community settings or rural populations. Despite these limitations, the findings provide a valuable baseline for designing future longitudinal and interventional studies targeting CAD prevention in similar contexts.
Implication for Practice
The study highlights the need for targeted interventions to improve CAD prevention among patient, particularly focusing on males, and single individuals who demonstrated lower knowledge and poor preventive practice. Despite a moderate level of knowledge (67.2%), significant gaps remain in symptom recognition, health attitudes, and consistent lifestyle practices, especially among those with comorbid conditions. Cultural preferences for traditional medicine and reluctance to accept diagnosis also hinder effective prevention. Hospitals, as the primary source of information, should be leveraged to deliver structured, culturally sensitive education and counseling. Strengthening health literacy and preventive behaviors through gender sensitive, accessible, and context-specific program is crucial to improve CAD outcomes in this population.
Nurses play a pivotal role on CAD prevention through patient education, risk assessment, and behavioral counseling. They should deliver evidence-based, culturally sensitive education during every encounter and address misconception about traditional medicine and CAD management.
Conclusion and Recommendation
This study assessed KAP toward CAD prevention among cardiac patients. While 67.2 demonstrated good knowledge and 54.3% showed a positive attitude, only 59% exhibited good preventive practices. Major gaps were identified in lifestyle behaviors such as blood glucose monitoring, and cholesterol levels, and a notable reliance on traditional medicine. Multivariate analysis revealed that male gender, single marital status, unemployment, and presence of comorbidities were significantly associated with lower knowledge and poor preventive practices.
While awareness and attitude toward CAD prevention are moderately good, preventive practices remain inadequate, highlighting the need for comprehensive, patient-centered education integrated into routine cardiac care. Hospitals, cardiac clinics, and health bureaus should collaborate to establish structured patient education and counseling programs, led by nurses and health educators, to promote healthy behaviors, self-monitoring, and adherence to medical advice. Community-based interventions and policy support are essential to address sociodemographic disparities, discourage unsafe traditional practices, and strengthen preventive cardiovascular health services.
Footnotes
Acknowledgments
The authors would like to thank the College of Health Sciences Addis Ababa University, the participant hospital management, data collectors and study participants.
Ethical Consideration
Ethical clearance Ref: NoNUR.119/22was obtained from school of Nursing and Midwifery, College of Health Science Addis Ababa University-institution review committee. An official letter of cooperation was sought and submitted to the cardiology department. Participants were informed about the objectives of the study and those willing to take part in the study were requested to give their consent. Participants were also informed that participation is completely voluntarily, and they can withdraw from the study at any time they wish. All the collected data were kept confidential and no one except the members of the research team have been accessed to the collected information also name was not mentioned or was attached to anything that you say.
Consent for Publication
All authors who took part in the study have agreed publication of the article in the journal.
Authors’ Contributions
Hewan Sibhatu, Tigistu Gebreyohannis Gebretensaye, and Wudma Alemu Kassa conceived the idea and prepared the proposal. All were involved in data collection, analysis, and write-up of the research findings, Semarya Berhe Lemlem reviewed the final document and prepared the manuscript. All authors subsequently reviewed, read, and approved the final draft of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets generated and/or analyzed in the current study are available with the corresponding author on reasonable request.