
Abstract
Introduction
Globally, healthcare organizations have transitioned from paper-based documentation to electronic health records (EHR), including in Saudi Arabia. However, the adoption of EHR at the national level in Saudi Arabia needs more attention. Thus, this study aimed to determine the workflow integration of EHR and associated factors.
Objectives
The specific aims were to examine the level of EHR use and workflow integration among nurses, to determine the differences in EHR use and workflow integration based on nurses’ demographic characteristics, and to determine the association between the predictive factors and EHR workflow integration.
Methods
This is a cross-sectional, correlational descriptive study. The data were collected from 293 nurses using the convenience sampling method. The participating nurses completed a questionnaire that included two measures: the Information System Use Survey and the Workflow Integration Survey (WIS). The data were analyzed using descriptive and multivariate statistics with SPSS software.
Results
The nurses had a positive perception of EHR use and workflow. The EHR use scores differed based on workplace (P < .01), education level (P < .05), and area of practice (P < .001). Similarly, the EHR workflow integration scores varied according to workplace (P < .05), education level (P < .05), and area of practice (P < .001). Education level and workplace significantly predicted information system use. Furthermore, education level and information system use significantly predicted the EHR integration into nurses’ workflow.
Conclusion
The nurses expressed a greater perceived use of EHR regarding the integrated health information system, which was a predictor of EHR integration into nurses’ workflow.
Introduction
Electronic health records (EHR) represent a digital repository of patients’ medical information inputted by healthcare personnel into organizational computer systems (Atherton, 2011). They encompass comprehensive data regarding patients’ health status and medical history, including demographic information, medication records, allergies, laboratory and diagnostic test results, vital signs, treatment plans, and progress notes (Atherton, 2011). EHR systems facilitate the seamless exchange of patient data across various healthcare settings and within the same institution's healthcare team (Gamage et al., 2020; Keshta & Odeh, 2021). The rapid advancement in healthcare digitalization has led to the development of EHR systems that surpass traditional paper-based documentation in terms of content, documentation process, and structural organization (Akhu-Zaheya et al., 2018; Gamage et al., 2020). Traditional paper documentation is plagued by several issues such as incomplete data records, missing nurse signatures in many nursing notes, and illegible handwriting and abbreviations, leading to potential confusion (Akhu-Zaheya et al., 2018; Alruwaili, 2020).
However, the evolution of EHR systems aims to address these shortcomings and improve workflow efficiency, nursing documentation, usability, quality of care, data accessibility, and inter-professional communication between healthcare specialists (Akhu-Zaheya et al., 2018; Janett & Yeracaris, 2020; McCarthy et al., 2019; Tsai et al., 2020). Despite these advantages, EHR systems also present challenges, including potential interruptions compromising data confidentiality and security, as well as concerns regarding malpractice liability (Gamage et al., 2020). Moreover, the implementation of EHR systems raises significant issues related to safeguarding sensitive healthcare data stored in various locations and formats, which can impact patient information confidentiality and security, thereby affecting the adoption rate among healthcare institutions (Gamage et al., 2020; Keshta & Odeh, 2021). These challenges may ultimately influence patient safety and the quality of care delivered to hospitalized individuals (Akhu-Zaheya et al., 2018).
Literature Review
Healthcare organizations worldwide have transitioned from paper documentation to EHR systems (Akhu-Zaheya et al., 2018; Nguyen et al., 2014). In 2008, Saudi Arabia initiated the introduction of EHR in some government healthcare institutions (AlSadrah, 2020). However, the widespread adoption of EHR systems across the country progressed slowly owing to numerous aspects, including variations in EHR systems that may impact hospitals’ needs (AlSadrah, 2020). Additionally, negative attitudes of healthcare professionals toward EHR, limited computer proficiency, and insufficient technical support and training have hindered EHR advancement (AlSadrah, 2020). Addressing these limitations is crucial for optimal EHR implementation and utilization in all Saudi Arabian healthcare institutions. To overcome these challenges, the Saudi government allocated over USD 1 billion (approximately 4 billion Saudi riyals) (AlSadrah, 2020).
Currently, the use of EHR presents several challenges, including technological complexity, loss of access during power outages, potential disruptions in physician–patient communication, security breaches, and time constraints related to data entry (AlSadrah, 2020). Furthermore, factors such as healthcare personnel characteristics (e.g., age, gender, leadership role), financial resources, perceived usefulness, and healthcare setting size influence HER deployment (Alzghaibi & Hutchings, 2022). Nurses’ attitudes also impact EHR system utilization (Alrasheeday et al., 2023). A study by Alrasheeday et al. (2023) revealed that 81.1% of nurses held a positive attitude toward her use, while 18.9% expressed negativity. Investigating how nurses’ attitudes influence her use is essential in understanding its adoption.
Despite widespread EHR implementation in Saudi Arabian healthcare settings, standardized data structures for EHR utilization and unified workflow integration in clinical environments are lacking. Nurses, who frequently interact with their systems on a daily basis often encounter challenges in navigating complex programs or inefficient data entry processes, leading to decreased efficiency and potential errors in patient care (Tsai et al., 2020). Understanding EHR use and workflow integration among nurses is crucial for policymakers and administrators to develop effective strategies for improving their quality. Thus, this study aims to determine factors influencing EHR workflow integration among nurses, with specific aims:
To examine the level of EHR use and workflow integration among nurses. To determine the differences in EHR use and workflow integration based on nurses’ demographic characteristics. To determine the association between the predictive factors and EHR workflow integration.
Methods
Study Design
This study adopts a cross-sectional, correlational descriptive design. Data were collected at single point in time. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE).
Setting and Sampling Design
A non-probability convenience-sampling method was utilized, involving staff nurses from the two tertiary hospitals. The study was conducted in two tertiary hospitals in Saudi Arabia utilizing the same EHR system (namely, Electronic System for Integrated Health Information [eSiHi]). Launched in April 2015, eSiHi is employed by healthcare professionals, including nurses. Hospital A, with 800 beds, is larger and more diversified in specialty compared to Hospital B, which has 234 beds and specializes primarily in ophthalmology and ear, nose, and throat (ENT) care. Despite their differences, both hospitals fall under the same umbrella organization, with a combined annual admission of 45,966 inpatients and 1,229,628 outpatients, with the majority treated at Hospital A.
Inclusion and Exclusion Criteria
Included in the study were staff nurses providing direct patient care, employed for at least 1 year at either hospital, and possessing current access to their hospital's eSiHi system. Excluded were nurses in administrative roles or those opting not to participate, as well as those with limited experience utilizing the eSiHi system.
Sample Size
Sample size determination using G*Power (Version 3.1.7) yielded a minimum required sample of 118 nurses to achieve a medium effect size of 0.15 and a power of 0.80, with a significance level of .05. To mitigate the risk of missing data, 300 questionnaires were distributed.
Data Collection Procedure
A self-administered paper-pencil questionnaire was distributed to participants through collaboration with the research units at both hospitals. Each unit received 150 questionnaires, totaling 300. Upon completion, participants returned the sealed envelopes containing the surveys to the research unit representatives, who then coordinated with the main researcher for collection. Data were collected between May 2022 and June 2022.
Instruments
Data collection employed a structured questionnaire encompassing three parts. The first part included demographic information such as age, gender, marital status, nationality, highest education level, current nursing unit, hospital affiliation, years of experience in the current unit, and training with the eSiHi.
The second part utilized the Information System Use Instrument (ISUI), comprising eight items scored on a 5-point Likert scale (1 = never or almost never to 5 = always or almost always), with total scores ranged between 8 and 40 (Abdrbo et al., 2010). The high score indicates greater benefit of using EHR (Abdrbo et al., 2010). This scale demonstrates good reliability (Cronbach's alpha of 0.82; Abdrbo et al., 2010). In addition, Abdrbo et al. (2010) assessed the construct validity by involving nurses to reflect on their computer experience on a 7-visual analog scale (ranging from novice to expert) and then compared it with the nurses’ scores on ISUI. The Pearson product–moment correlation was used to show a positive relationship between nurses’ computer experience and ISUI score which means the more experience in using computer reflect high use of the systems (Abdrbo et al., 2010).
The third part involved the Workflow Integration Survey (WIS), consisting of 12 items scored on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), with total scores ranging between 12 and 60 (Flanagan et al., 2011). Higher scores indicate high workflow integration (Flanagan et al., 2011). Also, this scale has 6 reversed items of the 12 items with good reliability (Cronbach's alpha of 0.93; Flanagan et al., 2011). Herein, the WIS encompasses four dimensions such as navigation, functionality, ease of use, and impact on the workload (Flanagan et al., 2011).
Ethical Considerations
Approval for this study was obtained from the Institutional Review Board (IRB) of both hospitals. Each questionnaire included a cover letter detailing the study's purpose, benefits and potential risks, participants’ rights, voluntary participation, and confidentiality assurances. Respondents’ data were anonymized, and no incentives were provided for participation. The consent form was waived because the completion of the survey was implied consent.
Data Analysis
Collected data were sequentially numbered for easy reference and entered into an Excel spreadsheet before being transferred to IBM SPSS Version 26. Initial descriptive analyses were conducted to identify missing data. Descriptive statistics were computed for demographic characteristics, EHR use, and workflow integration. Analysis of variance (ANOVA) was used to assess differences in nurses’ perceptions of EHR use and workflow integration, while multiple regression analysis was employed to predict the influence of demographic traits on EHR use and workflow integration. Significance was determined at P < .05.
Results
Demographic Traits
A total of 293 nurses participated in this study across two hospitals (Hospital A = 154; Hospital B = 139). Among them, 28% of nurses were aged 31 to 35, with a mean age of 36.8 years (Table 1). The majority of participants were female (n = 251, 85.7%), married (n = 191, 65.2%), and of Filipino descent (n = 168, 57.3%). Most nurses held a bachelor's degree in nursing (n = 215, 73.4%) and worked in intensive care units (ICUs) (n = 66, 22.5%). The average work experience was 8.9 years. All nurses reported undergoing training related to the EHR systems used in their respective hospitals.
Demographic Traits of the Nurses (N = 293).

Note. N = frequency; % = percentage; SD = standard deviation.
Nurses’ EHR System Use
In Table 2, the overall mean score of the nurses’ perception of EHR system use was 3.51 (SD = 0.94). Notably, nurses reported high utilization of the EHR system for patient notes and nursing reports (mean score = 3.72, SD = 0.73) and searching for patient-related information (mean score = 3.70, SD = 0.72). However, they indicated lower utilization in planning care (mean score = 3.18, SD = 1.13).
Information Systems Use Through the eSiHi System (N = 293).
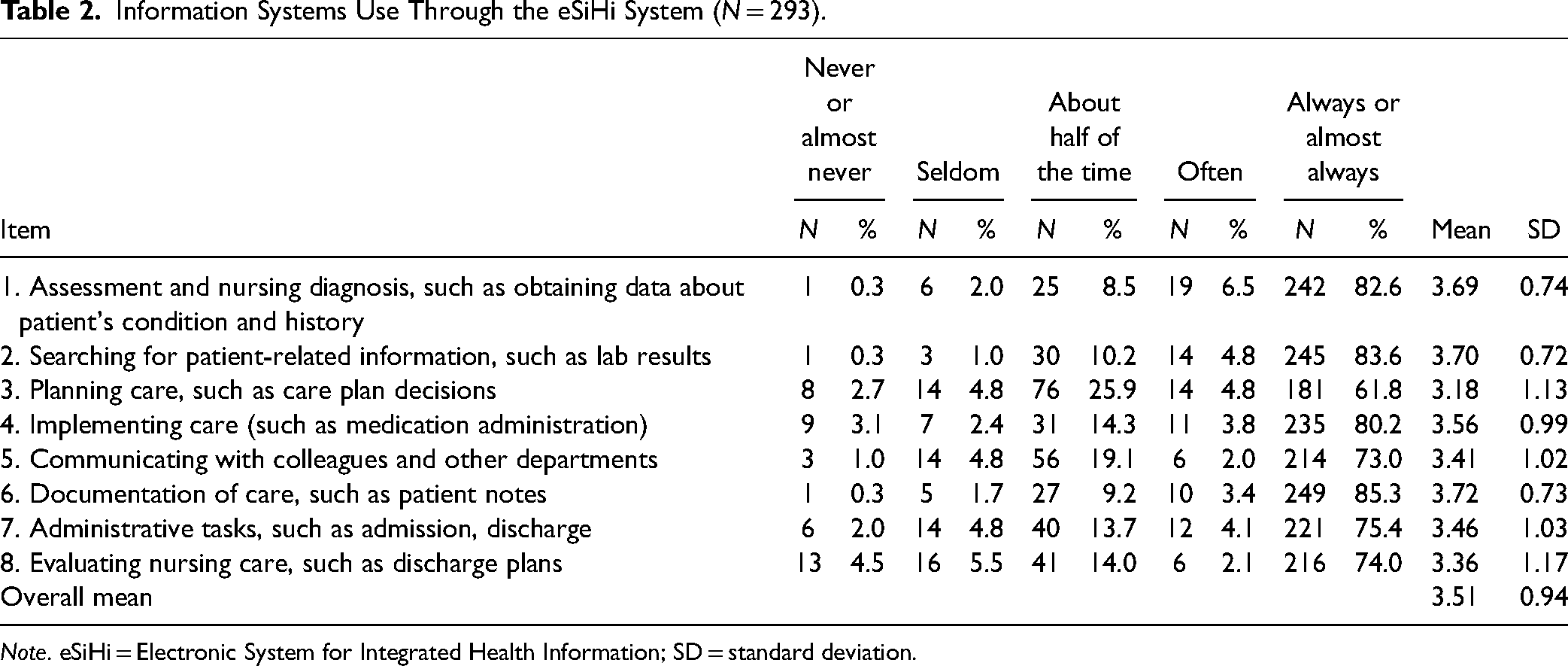
Note. eSiHi = Electronic System for Integrated Health Information; SD = standard deviation.
Nurses’ EHR Workflow Integration
Overall, nurses demonstrated high agreement with EHR workflow integration (mean score = 3.77, SD = 1.13) (Table 3). Among the four dimensions of the WIS, functionality received the highest agreement (M = 4.05, SD = 0.92), followed by navigation (M = 3.99, SD = 0.91), workload (M = 3.68, SD = 1.03), and usefulness (M = 3.37, SD = 1.06).
Workflow Integration When Using the eSiHi System (N = 293).

Note. eSiHi = Electronic System for Integrated Health Information; SD = standard deviation.
The item was reverse-scored.
Differences in EHR Use in Terms of Demographic Traits
Significant differences were observed in nurses’ perception of EHR use depending on the respondents’ demographic traits (Table 4). The nurses working in Hospital A showed significantly higher agreement than those working in Hospital B (F = 8.02; P < .01). The working units were significantly different in terms of nurses’ perception of EHR use (F = 5.44, P < .001). Thus, ANOVA post hoc test was run to determine the deferential between units. By considering the ICUs as the reference variable, the nurses working therein had a lower perception than nurses in the surgical, medical, outpatient, and other units (Table 5). Additionally, nurses with a diploma in nursing demonstrated a more positive perception of EHR use compared to those with bachelor's and master's degrees (M = 25.27, SD = 3.85) (Table 5).
Differences in eSiHi Use and Workflow Integration (N = 293).

Note. eSiHi = Electronic System for Integrated Health Information.
*Significance level at P < .05.
**Significance level at P < .01.
Post Hoc Results: Comparisons Between Groups.

Differences in EHR Workflow Integration in Terms of Demographic Traits
Nurses’ perception of EHR workflow integration significantly differed based on their current area of practice (F = 2.26, P = .03). However, no significant differences were found based on other demographic traits.
Predictors of EHR Use and Workflow Integration
Multiple regression analysis revealed that the highest education level and workplace significantly predicted EHR use (Table 6). Nurses with a bachelor's or diploma in nursing and those working in Hospital A reported more positive perceptions of EHR use. For workflow integration, the highest education level and information system use significantly predicted nurses’ perceptions. Nurses with a diploma agreed more with EHR workflow integration, and higher EHR system use predicted better workflow integration. The regression model for information system use was significant (R2 = 0.062, F = 2.057, P = .033), explaining 20.57% of nurses’ perception regarding EHR uses. Among the demographic traits, the highest education level and workplace significantly predicted EHR use. Nurses with a bachelor's degree (β = 3.40; P = .008) and those with a diploma (β = 3.82; P = .007) had more positive perceptions of EHR uses. Also, nurses working in Hospital A reported a more positive perception of EHR uses (β = −1.64; P = .002) than those working in Hospital B.
Predictors of eSiHi Use and Workflow Integration (N = 293).

Note. eSiHi = Electronic System for Integrated Health Information; β is the unstandardized coefficient; SE-b is the standardized error.
*Significance level at P < .05.
**Significance level at P < .01.
The regression model for the workflow integration was significant (R2 = 0.084, F = 2.515, P = .007), explaining 25.15% of nurses’ perception of EHR workflow integration. The regression model for workflow integration was significant (R2 = 0.084, F = 2.515, P = .007), explaining 25.15% of nurses’ perception of EHR workflow integration. Among the demographic traits, the highest education level (P < .05) and information system use (P < .001) significantly predicted EHR workflow integration. Nurses with a diploma (β = 1.98; P = .04) agreed more with EHR workflow integration than nurses with a bachelor's degree. Last, information system use among nurses significantly predicted workflow integration among nurses (β = 0.30; P = .04).
Discussion
This study aimed to determine the workflow integration of EHR and the associated factors at two public hospitals in Saudi Arabia. The findings provide insight for the government, hospitals, nursing administrators, and EHR developers regarding nurses’ use of EHR and workflow, potentially aiding in the improvement of EHR systems.
The overall perception of information system use showed that the nurses had a positive perception of using EHR in their daily nursing duties. This finding indicates that the nurses integrated the EHR system into their nursing care because hospitals must employ an EHR system for tasks such as documentation and reviewing patient data. Moreover, all participating nurses were trained in how to use EHR, implying that they could be interested in nursing informatics. However, this result should be interpreted with caution as EHR training might be mandatory in study settings. Previous findings also support the current study's results. The use of EHR has been widely considered beneficial since it improves the efficiency of care and yields good patient outcomes, including population health (Wager et al., 2017). This enables the application of EHR systems for organizing and analyzing a large amount of data regarding patient information (Wager et al., 2017). A systematic review of 55 articles revealed that there were more facilitators (e.g., productivity/efficiency, quality and data management, surveillance, preventive care) than barriers (e.g., missing data, no standards, productivity loss, overly complex technology) to using EHR to support public health, implying a certain level of use and acceptance of EHR (Kruse et al., 2018). In the US, a descriptive cross-sectional study among nurses from nursing informatics communities (the American Medical Informatics Association and the Healthcare Information and Management System Society) revealed similar findings that nurses used EHR as part of their job several times a day (Alrasheeday et al., 2023; Gartrell et al., 2015; Holmes et al., 2021).
Although the nurses in this study mostly agreed with the workflow integration of using EHR in assessing patients; formulating a nursing diagnosis; planning, implementing, documenting, and evaluating care; and communicating and performing other administrative tasks, they also expressed that using the system was challenging. This implies that they used EHR to perform daily assessment and diagnosis tasks but found it difficult to integrate the system into their workflow. Accordingly, there is a need to enhance the general usability of EHR as well as to consider other dimensions of workflow integration (e.g., navigation, functionality, workload), which requires nursing administrators to inform EHR developers where the problem was considered or situated as reported by the nurses. However, possible reasons why the use of EHR was challenging for the nurses were not explored; these require further investigation through qualitative research. In a previous study based on the views and experiences of 24 informatics professionals, many factors posed challenges in using EHR among experienced clinicians in the United States: analytics regarding study design, statistics, machine (computer) learning, data privacy and security, data quality and variability, fairness and bias, and the inflexibility of EHR (Holmes et al., 2021). There were also usability challenges specific to access and navigation, engagement in redundant procedures or workarounds, and recovery and analysis of relevant information to complete tasks (Holmes et al., 2021). The harmonization, integration, and storage of EHR also posed challenges relating to many research consortia regarding the COVID-19 pandemic. A previous systematic review of 18 studies, published from 2003 to 2014, also revealed that nurses faced challenges when using EHR, to document and manage symptoms in inpatient settings, which are considered threats to high-quality and safe nursing care (Ozkaynak et al., 2017). An integrative review of 18 studies indicated that navigation of the volumes of patient information was challenging and increased the cognitive workload related to compiling and synthesizing information from EHR among nurses and other clinicians (Wisner et al., 2019). A quantitative, cross-sectional study conducted in New Delhi, India reported similar findings where all participating nurses agreed that the use of EHR enhances nursing documentation; however, they were not comfortable using the system owing to a lack of training (Verma & Gupta, 2016). Tsai et al. (2020) also reported that inadequate or insufficient training and technical and educational support for users are considered frequent impediments to the uptake and use of EHR systems. Similarly, AlSadrah (2020) stated that a lack of training hindered advancement in the use of EHR systems at a national level in Saudi Arabia. Nevertheless, all nurses who participated in the current study reported that they had been trained on how the EHR system of their hospital operated.
Regarding the differences in the perceptions of using EHR and workflow integration, nurses working in Hospital A exhibited significantly higher ratings for using EHR than those working in Hospital B. This difference may relate to the nature of the hospitals and the type of nursing care. Hospital B specializes in ophthalmology and ENT care, while Hospital A has several departments and specialties. The nurses assigned to the outpatient clinics, medical units, and obstetric units had more positive perceptions than other units regarding the incorporation of EHR into their workflow. This disparity might be attributed to the variations in the numbers of patients admitted to the hospital daily and those who sought consultations at the outpatient clinics; such differences may have increased the frequency of using and integrating EHR into the nurses’ workflow. A high frequency of using and integrating EHR into the workflow owing to increased asynchronous communication through messages of varying clinical priority was reported in five Outpatient Department (OPD) clinics in the Netherlands (Vos et al., 2020). Similar findings were observed in a study conducted in the US with 12,923 responses, indicating that nurse practitioners in clinical settings with no on-site physicians were inclined to be assigned to urban areas and worked in OPD/ambulatory settings and primary care specialty units (Jones, 2017).
The present study revealed that the highest education level significantly predicted the usage and integration of EHR into nurses’ daily workflow. Additionally, the hospital where the nurses were working also predicted EHR usability. The nurses working in Hospital A had more positive perceptions of using EHR than those working in Hospital B. This outcome may be explained by the higher number of patient admissions and consultations at the outpatient clinics in Hospital A than in Hospital B. The nurses who had bachelor's degrees also reported higher usage of EHR. An increased perceived usability of EHR also resulted in higher workflow integration among these nurses. The findings are consistent with those of Melnick et al. (2021) that a higher perceived usability of EHR among physicians was associated with greater perceived positive outcomes, through the improvement of the quality of patient care. There were also fewer perceived negative outcomes reported, including worse patient interactions and work–life integration (Melnick et al., 2021).
Limitations of the Study
While the findings offer insights into the factors influencing workflow integration in EHR, the research has several limitations. Variations in EHR implementation among hospitals in the kingdom restrict the generalizability of the results beyond the study settings. Consequently, the findings may not be conclusive at the national level, primarily owing to the use of convenience sampling and the study's confinement to a single region. Thus, generalizing the findings to nurses from private hospitals and other government hospitals outside Riyadh may not be appropriate. Additionally, the use of self-report scales to collect data may introduce biases, such as social desirability bias, which could impact the quality of the nurses’ responses. However, the anonymous completion of the survey may have encouraged participants to provide honest responses regarding their perceptions. Furthermore, it is possible that nurses with a more positive impression of EHR were more inclined to participate in the study, potentially influencing the actual perceptions regarding EHR use and workflow integration.
Implications for Nursing Research and Practice
Future studies must include nurses at the national level across Saudi Arabia to establish generalizable findings. Qualitative research also needs to identify reasons why nurses find EHR usability and workflow integration challenging. The findings can serve as a basis for hospital and nursing administrators to develop future interventions aimed at making EHR usage and workflow integration less challenging for nurses. For EHR developers, the findings can aid in conducting system checks to improve specific areas, particularly the usability of the EHR workflow integration.
Conclusions
Utilizing and integrating EHR systems, such as the eSiHi, into nursing workflow is crucial. In this study, nurses reported frequent use of EHR during daily nursing tasks and procedures. Higher perceived usability of EHR predicted higher workflow integration among nurses. Additionally, the highest education level and perceived usability of EHR were predictors of EHR integration into nurses’ workflow. These findings suggest that nurses have successfully integrated EHR systems into their daily practices, while considering their area of practice and educational level.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Researchers Supporting Project (number: RSP2024R456) at King Saud University, Riyadh, Saudi Arabia.